
Abstract
Ultrasound-guided fine-needle aspiration (FNA) is fundamental in the evaluation of thyroid nodules to distinguish between benign and malignant nodules and to guide subsequent management. 1,2 In adults, FNA is safe and effective and is typically performed without sedation and with only mild patient discomfort. 3,4 In children, FNA is effective, but limited data exist regarding its safety and tolerability. 5,6 Studies of small cohorts have reported that pediatric thyroid FNA can be performed without sedation and with minimal complications. 7 –9 Nevertheless, uncertainty remains about optimal techniques for FNA in children, particularly for managing procedural pain and anxiety and for obtaining adequate samples for cytological evaluation. For these reasons, practices for performing pediatric FNA procedures vary, particularly regarding the use of sedation. We present a retrospective consecutive case series of pediatric thyroid FNA procedures conducted in an academic pediatric thyroid center over 26 years, evaluating the use of sedation, complication rates, and patient-reported pain.
Methods
We reviewed the medical records of consecutive patients under age 18 years who underwent ultrasound-guided FNA of a thyroid nodule in the pediatric Thyroid Center at Boston Children’s Hospital (BCH) and Brigham & Women’s Hospital (BWH) between January 1, 1998, and May 31, 2024. FNAs performed on thyroid bed nodules present after thyroidectomy, lymph nodes, or nonthyroid masses were excluded from analysis.
FNAs were performed in a multidisciplinary pediatric thyroid nodule clinic (Fig. 1). Visits were scheduled for evaluation of a known or suspected thyroid nodule. Sixty minutes prior to each visit, a nurse performed a clinical intake, applied topical eutectic mixture of local anesthetic (lidocaine 2.5%/prilocaine 2.5%) over the anterior neck, and covered it with an adhesive dressing. A clinical evaluation was performed by a pediatric thyroidologist, and ultrasound was performed by a radiologist with expertise in thyroid ultrasonography. A recommendation for FNA was made, if indicated, after joint image review by the thyroidologist and the radiologist. Prior to 2019, FNA was performed for all nodules ≥1 cm in diameter. 10 Subsequently, following the publication of pediatric data regarding sonographic features associated with malignancy, 11 –14 our practice changed to recommend fewer FNAs of sonographically low-risk nodules with significant cystic content.
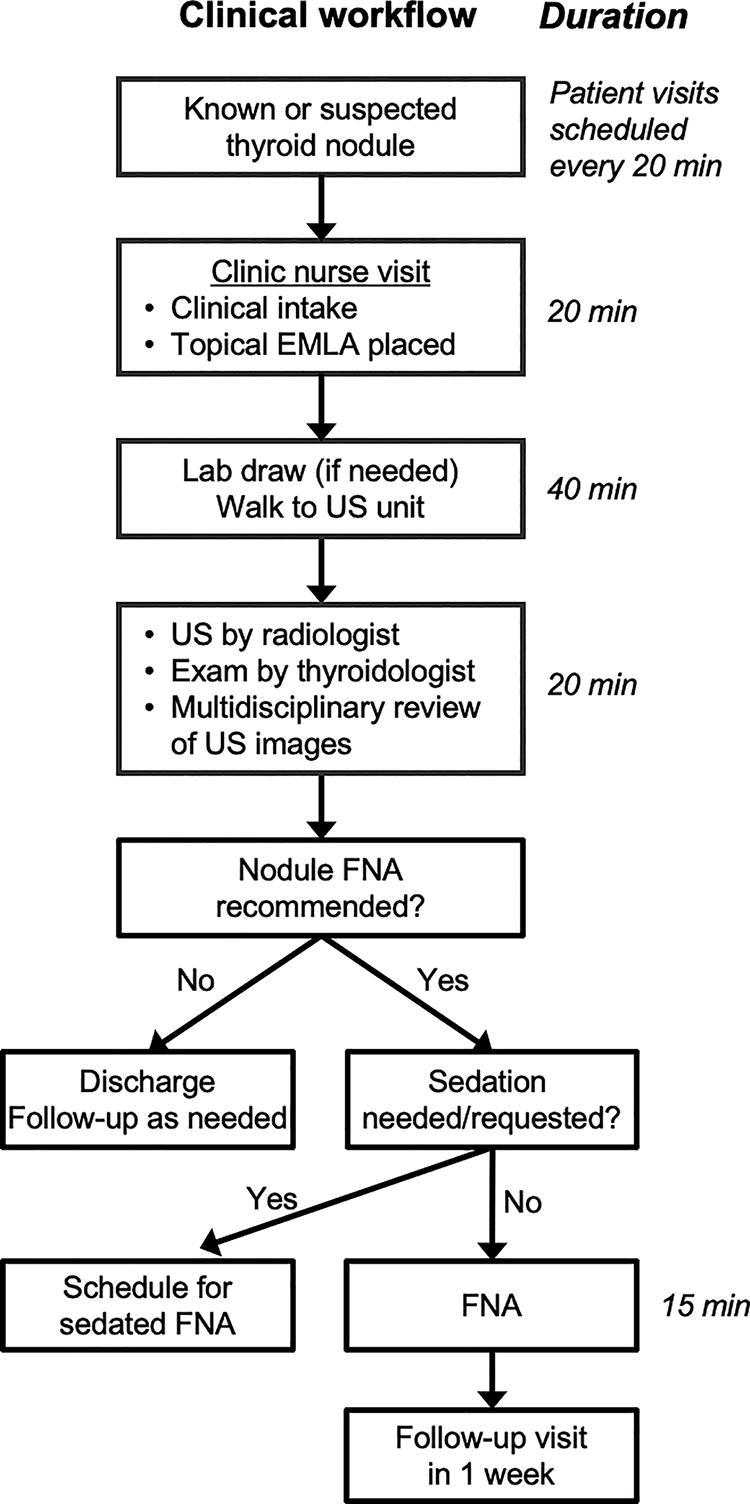
Clinic workflow for a multidisciplinary pediatric thyroid nodule clinic.
If sedation was judged necessary by the physician for safe performance of FNA or was requested by the patient or family, a subsequent visit was scheduled for sedated FNA. Otherwise, FNA was performed at the initial visit. The FNA site was marked, anesthetized with intradermal 1% lidocaine (0.5–1 mL) using a 27–30-gauge needle, and cleaned twice with alcohol before FNA; a full sterile technique was not used. FNA was performed by the thyroidologist using a 5- or 10-mL syringe with a 25-gauge 1.5-inch needle, making three to six passes per nodule with gentle back-pressure on the syringe. Ultrasound guidance was provided by the radiologist using a high-frequency ultrasound probe oriented longitudinally with respect to the needle. Aspirates were processed using a liquid cytology preparation, and cytology was interpreted according to the Bethesda System for Reporting Thyroid Cytopathology. 6 Rapid on-site evaluation (ROSE) of cytology for specimen adequacy was not performed, except in rare cases of repeated nondiagnostic cytology. A parent or family member was present at the bedside throughout the procedure. Behavioral distraction techniques, including use of videos or music, were provided by the thyroidologist or a social worker in collaboration with a parent or family member. 15 In some patients in whom the need for FNA was known in advance, oral lorazepam (0.25–1 mg, 0.005–0.03 mg/kg) was administered 1–2 hours before the procedure.
Patient, nodule, and procedure characteristics, procedure complications, and cytology results were collected from the medical record. Complications assessed included carotid hematoma, tracheal puncture, infection, and needle tract implantation of malignancy; intrathyroidal or soft tissue hematoma was not documented consistently and therefore was not assessed. As part of a quality improvement initiative between September 2020 and January 2023, patient-reported pain was evaluated using Wong-Baker pain scales (0–10) to quantify pain caused by injection of local anesthetic and by FNA needle passes. 16 Patients were requested to complete pain scales anonymously immediately following the FNA procedure. This study was approved by the Institutional Review Boards of BCH (M10-08-0444) and BWH (2017P000660).
Results
During the study period, 496 patients (78.8% female) underwent FNA of 867 thyroid nodules during 727 FNA procedures performed at a median (range) age of 15.3 (1.4–17.9) years. Thirty-eight of 727 procedures (5.2%) were performed on patients younger than 10 years. A total of 150 patients (30.2%) underwent more than one FNA procedure. Characteristics of the patients and procedures are shown in Table 1.
Characteristics of Pediatric Thyroid Patients Undergoing Fine-Needle Aspiration and Procedures
Data reported as n (%) or median (range).
FNA, fine-needle aspiration.
FNA was performed without sedation in 708 of 727 procedures (97.4%). Oral lorazepam premedication was administered in 28 of 727 procedures (3.9%), 14 of which were repeat FNA procedures. FNA was performed with sedation in 19 cases (2.6%). Median patient age was younger for procedures performed with sedation than for those without sedation (9.5 [1.4–17.1] years vs. 15.5 [4.9–17.9], p < 0.001). The primary reasons for sedation were patient/family preference (9/727 1.2%), young age as assessed by the provider (7/727, 1.0%), or developmental delay (3/727, 0.4%). Among the 8 patients who requested sedation, 2 did so for initial FNA, 1 for initial and repeat FNA, and 5 only for repeat FNA. Among 147 patients who underwent initial FNA without sedation and later required subsequent FNA, 141 of 147 (95.9%) underwent repeat FNA without sedation.
Forty-five patients (73.3% female) of median (range) age 16 (10–17) years returned pain scale surveys. Median pain scores were 2 of 10 (range: 0–5, interquartile range [IQR]: 1.5–2) for injection of local anesthetic and 3 of 10 (range: 0–6, IQR: 2–4) for FNA needle passes. The seven patients who underwent FNA of multiple nodules during the same procedure reported no differences in pain with injection of local anesthetic (p = 0.97) or FNA passes (p = 0.31) compared with patients who underwent FNA of a single nodule. No differences in pain scores were observed between male and female patients.
In 727 FNA procedures, no episodes of tracheal puncture, infection, or needle tract implantation of malignancy occurred. One procedure (0.14%) was complicated by a small carotid intramural hematoma that was observed serially by ultrasound and resolved.
Over the 26-year study period, 167 of 867 nodules (19.3%) had nondiagnostic cytology. In the last 5 years of the study period (2019–2024), the rate of nondiagnostic cytology was 14 of 213 (6.6%), significantly lower than in prior years (p < 0.0001).
Discussion
Consensus guidelines recommend FNA for the evaluation of thyroid nodules in children, 1 but the limited data on safety and tolerability of FNA in children may have contributed to practice variations. Particular uncertainty exists about the utility of sedation in children to increase patient comfort and sample adequacy, and additional data to clarify this question are important given the potential risks and costs of sedation.
In our large cohort, pediatric thyroid FNA was performed without sedation in over 97% of cases, including in children as young as 5 years. There were no clinically significant complications, and with use of local anesthetics, distraction techniques, and the presence of a parent/caregiver, patient-reported pain was mild and similar to that reported by adults undergoing thyroid FNA 3,4 and by children experiencing other routine needle stick procedures. 17 Of the few patients in whom sedation was used, in half of cases this was elected by the provider based on their assessment of the child’s ability to tolerate the procedure in view of their age or developmental status. In only 1.2% of cases was sedation requested by the patient/family, mostly for repeat FNA procedures. Notably, most patients requiring repeat FNA did not request sedation (96%), although a few benefitted from a small dose of oral lorazepam. These results suggest that, with appropriate pain management techniques, the vast majority of pediatric thyroid FNA can be performed safely, with only mild discomfort, and without sedation.
Sedation has been advocated to reduce the rate of nondiagnostic cytology and thereby to reduce the need for repeat FNA procedures. Despite minimal use of sedation in this study, the rate of nondiagnostic cytology in the final 5 years (6.6%) was lower than that reported in meta-analyses of adults (12.2%) 18 or children (11.4%) 5 and, notably, similar to that reported in adult studies of FNA performed with ROSE (6.6–9.5%). 19 The markedly higher nondiagnostic rate in prior years reflects the evolution of our clinical practice of selecting nodules for FNA. After 2018, our practice changed to performing fewer FNAs of nodules with increased cystic content, which are less likely to be malignant and more likely to yield nondiagnostic cytology. 20 Therefore, the rate of nondiagnostic cytology in the final 5 years of this study best reflects the current clinical practice of pediatric nodule evaluation and suggests that sedation is not necessary to achieve acceptable adequacy rates for pediatric thyroid FNA.
Strengths of this study include its size, duration, and consistency of data collection. A limitation is that patient-reported pain data were collected in only a subset of patients during a time-limited quality improvement project. In addition, bias may exist in which patients chose to complete the voluntary pain survey. Finally, pain was assessed immediately after the procedure, so its duration was not assessed.
In summary, thyroid FNA in children can be performed safely, with only mild discomfort and acceptable sample adequacy rates, and without sedation in most cases, including repeat FNA procedures for the minority with initial nondiagnostic cytology. Therefore, for routine pediatric thyroid FNA the increased risks and costs of sedation may outweigh its benefits, and we suggest that sedation be considered primarily for children who are young, have developmental delay, or require more complex procedures such as FNA of abnormal lymph nodes.
Footnotes
Authors’ Contributions
S.M.: Investigation, formal analysis, data curation, and writing—original draft. C.E.C.: Conceptualization, methodology, investigation, and writing—review and editing. C.G.: Investigation, data curation, and writing—review and editing. A.D.: Investigation, data curation, and writing—review and editing. B.F.: Investigation, data curation, and writing—review and editing. J.C.S.: Formal analysis and writing—review and editing. D.M.R.: Methodology, investigation, and writing—review and editing. J.R.S.: Conceptualization, methodology, investigation, and writing—review and editing. A.J.W.: Conceptualization, methodology, investigation, formal analysis, data curation, writing—review and editing, and supervision.
Author Disclosure Statement
The authors have no relevant financial relationships or conflicts of interest to disclose.
Funding Information
This work was supported by National Institutes of Health grant 5T32-DK007699-41.