
Abstract

Next-generation sequencing (NGS) of thyroid nodules is becoming increasingly common as a powerful diagnostic and prognostic tool in clinical practice worldwide. Numerous examples at both pre- and postoperative levels have demonstrated the benefits of incorporating NGS into the evaluation of thyroid lesions. However, comprehensive genomic analyses are still limited to certain practices, and many laboratories face challenges with the increased workload and costs associated with these molecular studies. As a result, routine morphology and immunohistochemistry can serve as efficient alternatives for identifying clinically significant genetic changes. For instance, florid nuclear alterations and BRAF p.V600E-mutation specific VE1 immunohistochemistry are reliable indicators of underlying BRAF p. V600E -driven pathogenesis, providing valuable diagnostic and theranostic information.
Recent advances have highlighted the role of aberrant micro-RNA (miRNA) expression in driving subsets of thyroid tumors, often due to mutations in key miRNA regulatory genes. DICER1 syndrome, a relatively newly described familial (inherited) disorder caused by germline DICER1 variants, is a multi-tumor condition with an overrepresentation of thyroid follicular nodular disease (TFND) and follicular-patterned differentiated thyroid carcinomas. Subsequent studies have identified somatic DICER1 mutations in around 3% of follicular-patterned thyroid neoplasms in adults. 1 In contrast, pediatric and adolescent patients with follicular-patterned papillary thyroid carcinoma and poorly differentiated thyroid carcinoma show a higher prevalence of these mutations. 2,3 Because pathogenic DICER1 mutations found in tumor tissue may be germline and syndromic, their identification is crucial for diagnosing inherited (syndromic) disease, which may be a sporadic-looking manifestation. Somatic DICER1 mutations typically cluster at hotspot codons within the regulatory domains, while germline variants are often truncating and can occur throughout the gene. Therefore, whole-gene sequencing is necessary to fully exclude germline involvement and the risk of syndromic disease.
Since 2018, the data on DICER1-related thyroid disease has been increasingly documented in the literature. The identification of multifocal follicular adenoma with papillary architecture characterized by intrafollicular centripetal papillary growth, in association with TFND, follicular patterned-differentiated thyroid carcinoma, and involutional changes in the nontumorous thyroid parenchyma are well-recognized features of germline DICER1-related thyroid manifestations. 4 Recent studies from Sweden have further expanded on additional specific morphological features in thyroid lesions that strongly suggest DICER1 variants. 5 Notably, follicular thyroid tumors with a predominant macrofollicular growth pattern and areas of palely stained involutional changes are two key histological hallmarks of DICER1 mutations (Fig. 1). The involutional (atrophic) changes, in particular, appear to be valuable for detecting DICER1 involvement, demonstrating a sensitivity of 77% and a specificity of 95% in a small cohort study. 6 Importantly, this study also found that 3 out of 12 DICER1-driven tumors identified through histological screening also harbored the same variant in constitutional tissues, highlighting the ability of histology to accurately predict mutations, some of which may be germline and clinically significant. 6 Future studies on fine needle aspiration biopsy samples may also help determine whether cytological features can aid in identifying DICER1 mutations preoperatively.
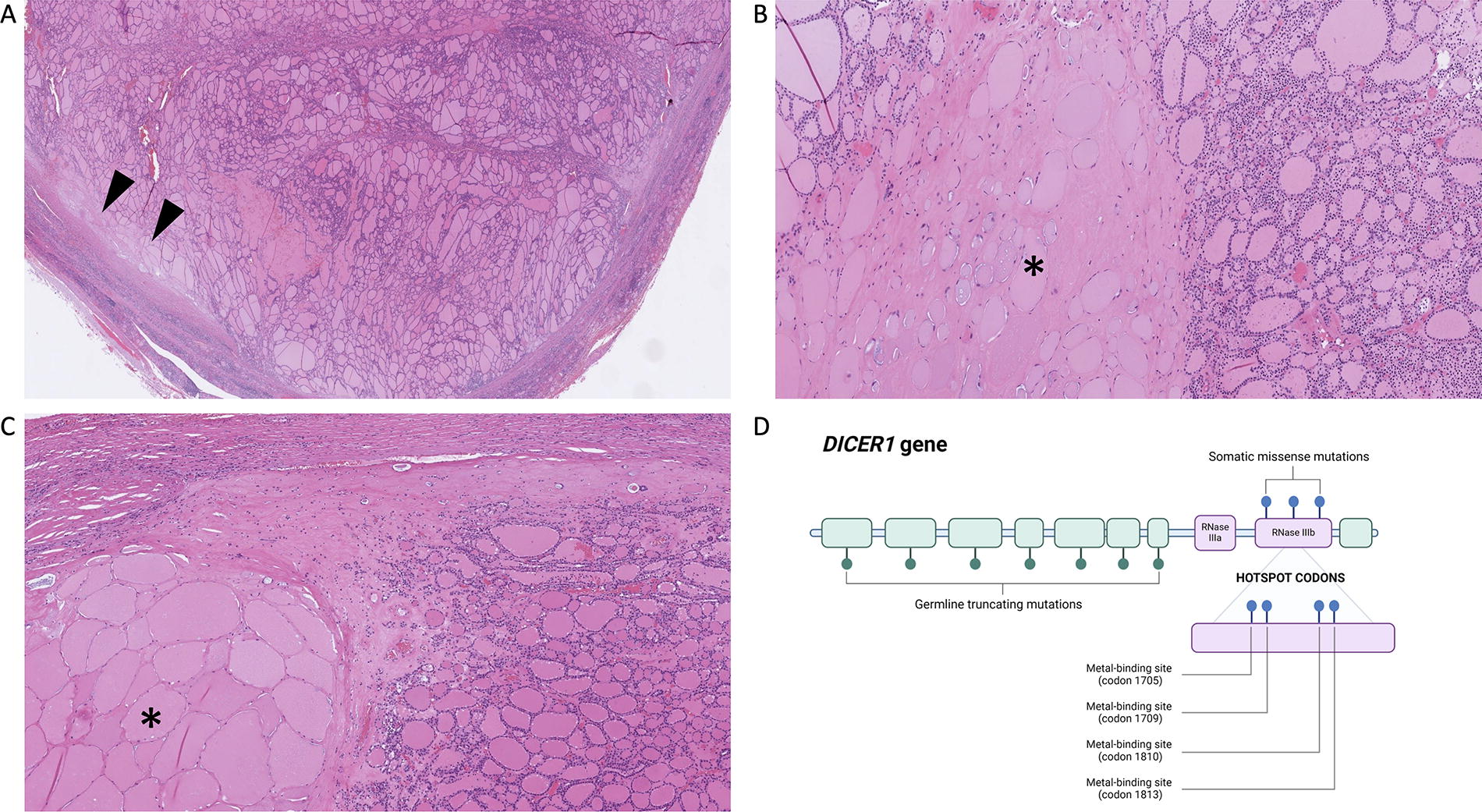
Histological hallmarks of DICER1 mutated thyroid tumors. This minimally invasive follicular thyroid carcinoma displayed macrofollicles and areas of atrophic/involuted change (marked with arrowheads in (
As endocrine pathologists representing two high-volume thyroid centers, we believe that the identification of these histological harbingers is of clinical interest to enhance the distinction of germline DICER1-related thyroid disease.
Footnotes
Authors’ Contributions
C.C.J.: Conceptualization and writing—original draft. O.M.: Conceptualization, writing—review and editing.
Author Disclosure Statement
The authors have no conflicts of interest to disclose.
Funding Information
C.C.J. is funded by the Swedish Cancer Society (Senior Clinical Investigator Award, grant no. 23-0616 SCIA).