
Abstract
Background:
Familial non-medullary thyroid carcinoma (FNMTC) accounts for approximately 9% of differentiated thyroid cancer (DTC). There is conflicting data on the FNMTC aggressiveness compared with sporadic DTC (sDTC), leading to usually more extensive therapy applied for FNMTC, given its autosomal dominant genetic background. This study aimed to compare the progression-free survival (PFS) in patients with FNMTC and sDTC treated with standard therapy.
Methods:
This longitudinal retrospective cohort study included patients with FNMTC, defined as at least two first-degree relatives affected by DTC. FNMTC patients were matched with sDTC in a 1:3 ratio based on age, sex, American Thyroid Association recurrence risk stratification (ATA-R), extent of initial surgery, and diagnosis date. The primary outcome was PFS. Kaplan–Meier curves were used to compare PFS between the groups, and the Cox proportional hazards model was used to assess confounders.
Results:
From 95 affected FNMTC patients, 30 were excluded due to lack of follow-up data. The study population consisted of 65 FNMTC and 170 sDTC patients, with a median follow-up of 4.73 (2.87–10.27) years for FNMTC and 5.83 (2.33–10.79) years for sDTC (p = 0.76). There was 100% matching for ATA-R, sex, surgery type, and year of surgery and a satisfactory matching for age (43.12 ± 15.11 vs. 42.76 ± 12.46 years, p = 0.85). FNMTC exhibited a smaller tumor size (1.20 ± 0.96 vs. 1.89 ± 1.51 cm, p < 0.01) and fewer positive lymph nodes (range 0–13 vs. 0–38, p = 0.009) at presentation. The rate of repeated neck surgeries for persistent/recurrent disease was comparable between the groups: 13.8% (9/65) for FNMTC vs. 17.7% (30/170) for sDTC (p = 0.48). There was no difference in radioactive iodine (RAI) therapy dosage between the groups (104 [100–149] vs. 106 [76–160] mCi, p = 0.82). During follow-up, 15.4% of FNMTC and 18.2% of sDTC patients experienced disease progression (p = 0.61). PFS was non-different between groups (p = 0.56) and was associated with ATA-R (high vs. low hazard ratio [HR]: 9.2, confidence interval [CI]: 2.67–31.85, p < 0.001) and sex (male vs. female, HR: 2.5, CI: 1.11–5.6, p = 0.026).
Conclusions:
No difference in PFS between FNMTC and sDTC patients suggests comparable responsiveness to standard therapy. Therefore, the management of FNMTC should align with the standard of care for DTC to avoid overtreatment of FNMTC.
Introduction
Thyroid cancer, ranking ninth globally in cancer incidence, 1 is predominantly represented by papillary thyroid carcinoma (PTC) and is characterized by a 10-year survival rate exceeding 90%. 2 Despite its generally favorable prognosis, certain pathological factors, like extensive extrathyroidal extension, bulky lymph node involvement, and distant metastases, adversely impact clinical outcomes. 2 Traditional risk factors for PTC development include radiation exposure and familial occurrence. 3 Familial non-medullary thyroid carcinoma (FNMTC), representing up to 9% of non-medullary thyroid carcinomas, is an autosomal dominant disorder with variable penetrance. 4,5 Managing affected families presents challenges, including debates on screening strategy of unaffected family members and appropriate initial therapeutic approaches for affected individuals. 6 Conflicting data on FNMTC aggressiveness and initial therapy response as compared with sporadic differentiated thyroid cancer (sDTC) complicates the advocacy for more optimal treatments. 7
Limited and conflicted evidence exists regarding the natural history of FNMTC and its response to standard treatment compared with sDTC. 8 –12 While some studies controlled for baseline risk stratification differences, others reported diverse baseline characteristics and mixed disease outcomes. This variability may stem from retrospective designs, small sample sizes, inclusion of families with varying affected kindreds, and genetic variability across populations. While most studies reported more aggressive disease at FNMTC presentation, leading to worse outcomes, 13 –18 several others indicated similar outcomes despite more aggressive disease presentation, 19 –23 or similar baseline characteristics resulting in either comparable 12,13,24 or worse outcomes. 25 Therefore, evidence from controlled studies with comparable groups with objective treatment response measures as primary outcomes is crucial for establishment of informed therapeutic strategies. There are limited studies yielding conflicting results that have directly compared FNMTC with matched by baseline characteristic sDTC patients focusing on recurrence-free survival (RFS) or disease-free survival (DFS). 8 –10,12 Notably, these case-control studies relied on the TNM (tumor, node, metastasis) staging system as the matching tool. However, this approach may not accurately predict thyroid cancer progression and recurrence as it is a prognostic measure for disease-specific survival (DSS) rather than progression-free survival (PFS). 26 Therefore, the American Thyroid Association (ATA) risk stratification system was developed to predict the risk of persistent/recurrent progressive disease. 26 However, there are no data on PFS in patients with FNMTC as compared with sDTC that addressed the baseline bias using the ATA risk stratification (ATA-R).
Therefore, the goal of our study was to evaluate the response to standard therapy, defined as PFS, in FNMTC and sDTC patients characterized by similar baseline characteristics. Since PFS depends on age, sex, and ATA-R, we used these variables as matching criteria, forming a novel approach for analysis of the response to therapy in FNTMC and sDTC cohorts. Additionally, we decided to match the study cohorts based on the date of the initial surgery, as well as the type of surgery, considering that thyroid cancer management guidelines have changed over time.
Methods
This was a single-center, longitudinal, retrospective cohort study, approved by the National Institutes of Health (NIH) Institutional Review Board (IRB) and the Office for Human Research Protections (IRB number: 10-DK-0102 and 77-DK-0096, clinicaltrials.gov IDs
Demographic, clinical, pathological, and molecular data were collected from medical records, family history questionnaires, and patient interviews. Family pedigrees, physical examinations, imaging studies, and laboratory tests were obtained. Follow-up studies included serum Tg and anti-Tg antibodies measurements every 6 months to annually, along with ultrasound of the neck. Depending on the clinical presentation, CT scans of the neck, chest, and abdomen, MRI, radioactive iodine (RAI) whole-body scans, and Fluorodeoxyglucose Positron Emission Tomography (FDG-PET) scans were also performed. All pathology slides were reviewed at the authors’ institution by experts in thyroid pathology.
PFS was defined from the initial surgery date to the date of the first evidence of disease progression, with progression defined using RECIST (Response Evaluation Criteria in Solid Tumors) 1.1 criteria. 28,29 Progression criteria are met if there is either an increase of at least 20% in the sum of the largest diameters (LD) of target lesions compared with the smallest sum observed (nadir), using the baseline sum LD as a reference point, or the appearance of one or more new lesions, as well as the unequivocal progression of nontarget lesions. Additionally, in a subset of patients with progressive disease, the tissue diagnosis of progressive disease was established after repeated surgery. Response to therapy was evaluated based on disease status at the last follow-up visit and categorized as excellent response, biochemical incomplete response, structural incomplete response, and indeterminate response, as per ATA guidelines. 27 An excellent response was defined as follow-up studies showing negative imaging and/or a suppressed Tg level of less than 0.2 ng/mL or a stimulated Tg level of less than 1 ng/mL with negative anti-Tg antibodies. Biochemical incomplete response was defined as suppressed Tg level equal to or above 1 ng/ml or rising anti-Tg antibody levels in the absence of detectable disease on imaging. Structural incomplete response referred to persistent or newly identified loco-regional or distant metastatic disease. Indeterminate response included nonspecific biochemical or structural findings that could not be confidently classified as benign or malignant, such as detectable non-stimulated Tg less than 1 ng/ml or stable or declining anti-Tg antibody levels without definitive structural evidence of disease. We also compared PFS differences between subgroups of FNMTC participants with two affected family members versus those with three or more affected family members and sDTC. Furthermore, we compared PFS differences between FNMTC and sDTC across subgroups based on tumor size (>1 cm), presence or absence of lymph node metastases, absence of aggressive histology, and age above and below 55 years (see Supplementary Figures S1, S2, S3, S4 and S5).
Statistical analyses
Patients with FNMTC were matched to patients with sDTC in a 1:3 ratio using the Ccoptimalmatch package 30 in R based on sex, ATA-R, age, surgery type, and date of initial surgery (<2000, 2000–2009, and 2010–2024). The initial cohort consisted of 473 participants: 378 with sDTC and 95 with FNMTC. Thirty participants from the FNMTC group were excluded due to lack of follow-up prior to matching, leaving 65 FNMTC participants for matching. The baseline characteristics of excluded due to lack of follow-up data FNMTC patients were not significantly different of the included participants (Supplementary Table S1). After matching both groups in a 1:3 ratio, 208 participants from the sDTC group were excluded post-matching (Fig. 1). Patients were first matched on sex, ATA-risk, surgery type, and year of initial surgery (100% match) and then matched on age as follows: 37 (21.7%) out of 170 participants with sDTC were matched exactly by age, another 37 (21.7%) were matched within a 1-year age difference, and the remaining sDTC patients (56.5%) were matched as closely as possible.

Participant flow diagram. FNMTC, Familial non-medullary thyroid cancer; sDTC, sporadic differentiated thyroid cancer; ATA, American Thyroid Association.
A power calculation was performed to determine the required sample size prior to analysis. Based on an anticipated reference 5-year progression rate of 20%, 27 the calculation showed that a sample size of 235 participants would provide 97% power to detect a 5-year progression rate of 10% at an alpha level of 0.05. This sample size was deemed sufficient to detect clinically meaningful differences in progression rates between the groups. We also performed a post-hoc power analysis based on actual data.
Baseline characteristics were summarized using mean with standard deviation or median with interquartile range (IQR) for continuous outcomes with normal and non-normal distribution, respectively, and frequencies for categorical outcomes.
Kaplan–Meier (KM) survival curves and log-rank test were used to examine PFS differences between FNMTC and sDTC groups. Cox proportional hazard models were used to assess the cofounding factors of progression. The analysis considered several confounding factors, including ATA risk classification, sex, tumor size, and the presence of lymph node metastases in both the lateral and central neck compartments. SAS 9.4 and R Studio software (Boston, MA) were used for all analyses, with significance set at p value <0.05. All statistical analyses were performed by a qualified statistician (S.A.).
Results
The study cohort consisted of 65 patients with FNMTC and 170 participants with sDTC. Within the FNMTC group, 39 patients had a known thyroid cancer diagnosis before enrollment, while 26 cancer cases were detected by screening (Fig. 1). The follow-up duration did not differ significantly between the groups: the median was 4.73 years (IQR 2.87–10.27) for FNMTC and 5.83 years (IQR 2.33–10.79) for sDTC (p = 0.76). Among FMNTC patients, 20 belonged to families with 2 first-degree relatives affected by thyroid cancer, while the remaining 45 participants were from families with ≥3 members affected (range 3–10).
There were no differences in sex, ATA-R, or the year and extent of the surgical treatment between the study groups due to exact matching. The mean age for FNMTC of 43.1 ± 15.1 was comparable with the sDTC cohort of 42.76 ± 12.46 (p = 0.85). Regarding ATA-R, 46.2% and 43.5% of patients belonged to the low-risk category, 46.2% and 48.8% to the intermediate-risk category, and 7.7% and 7.7% to the high-risk category in the FNMTC and sDTC groups, respectively (Table 1).
Comparison of Baseline Characteristic and Treatment Modalities Between Patients Diagnosed with Familial Non-Medullary Thyroid Cancer (FNMTC) and Sporadic Differentiated Thyroid Cancer (sDTC)
Bold values indicate statistical significance at p < 0.05.
Not associated with familial adenomatous polyposis (AFP).
American Thyroid Association (ATA) Risk of Recurrence Stratification System 2015.
SD, standard deviation; N/A, not applicable; IQR, interquartile range; RAI, radioactive iodine; mCi, millicurie.
Ethnic origin differed significantly between FNMTC and sDTC (p < 0.01), with 100% of FNMTC patients being not Hispanic or Latino, compared to 64.1% in sDTC, while 34.7% of sDTC patients were Hispanic or Latino, and 1.2% were classified as unknown.
No significant differences were observed between FNMTC and sDTC in terms of primary tumor’s multifocality, gross extrathyroidal extension, distant metastases, or tissue molecular mutations (all p > 0.1), though somatic driver data were limited in the FNMTC cohort (Table 1). In contrast, histological subtype differed significantly between groups (p = 0.02), with FNMTC more often presenting as classical PTC (78.5%) and less often as tall-cell PTC (PTCTC) compared to sDTC. Positive surgical margins were more prevalent in sDTC (22.98% vs. 10.7%, p = 0.05). FNMTC exhibited smaller tumor size at diagnosis (mean 1.20 ± 0.96 vs. 1.89 ± 1.51 cm, p < 0.001), with fewer positive lymph nodes (median 0 [IQR: 0–2] vs. 0 [IQR: 0–4], p = 0.01) and a higher prevalence of microcarcinomas (≤1 cm) (58.2% vs. 34.2%, p = 0.002). Lymphadenectomy types and rates were similar between groups. RAI treatment was given to 61.5% of FNMTC patients and 74.1% of sDTC patients (p = 0.06), all of whom had undergone total thyroidectomy. The median RAI dosage did not differ between the groups (p = 0.82), although a subset of patients received additional RAI during follow-up (Table 1).
Final disease status obtained at the last follow-up visit showed excellent response in 70.5% (43/61) of FNMTC vs. 59.3% (96/162) of sDTC patients. Biochemical and structural incomplete responses were nonsignificantly lower in FNMTC (6.6% and 3.3%) than in sDTC (9.3% and 6.7%), while indeterminate response rates were similar (19.6% vs. 24.7%). The differences were not statistically significant (p = 0.44, Table 1). During follow-up, repeat neck surgery was required for 9 out of 65 (13.8%) FNMTC patients, compared to 30 out of 170 (17.7%) in the sDTC group (p = 0.48) (Table 1). Patients from both groups did not receive systemic therapy during follow-up.
Disease progression occurred in 15.4% of FNMTC and 18.2% of sDTC patients, with a lack of difference in PFS probabilities evidenced by comparable KM curves (log-rank p = 0.56, Fig. 2). PFS remained not significantly different after adjustment for cofounding factors (PFS FNMTC vs. sDTC HR: 0.89, 95% CI: 0.35–2.21, p = 0.79, Fig. 3). Significant associations with PFS were found for ATA-R and sex (Table 2). High ATA risk was associated with shorter PFS (HR: 9.22, 95% CI: 2.67–31.85, p < 0.01), while males had a higher progression risk compared to females (HR 2.5, CI: 1.11–5.6, p = 0.026).
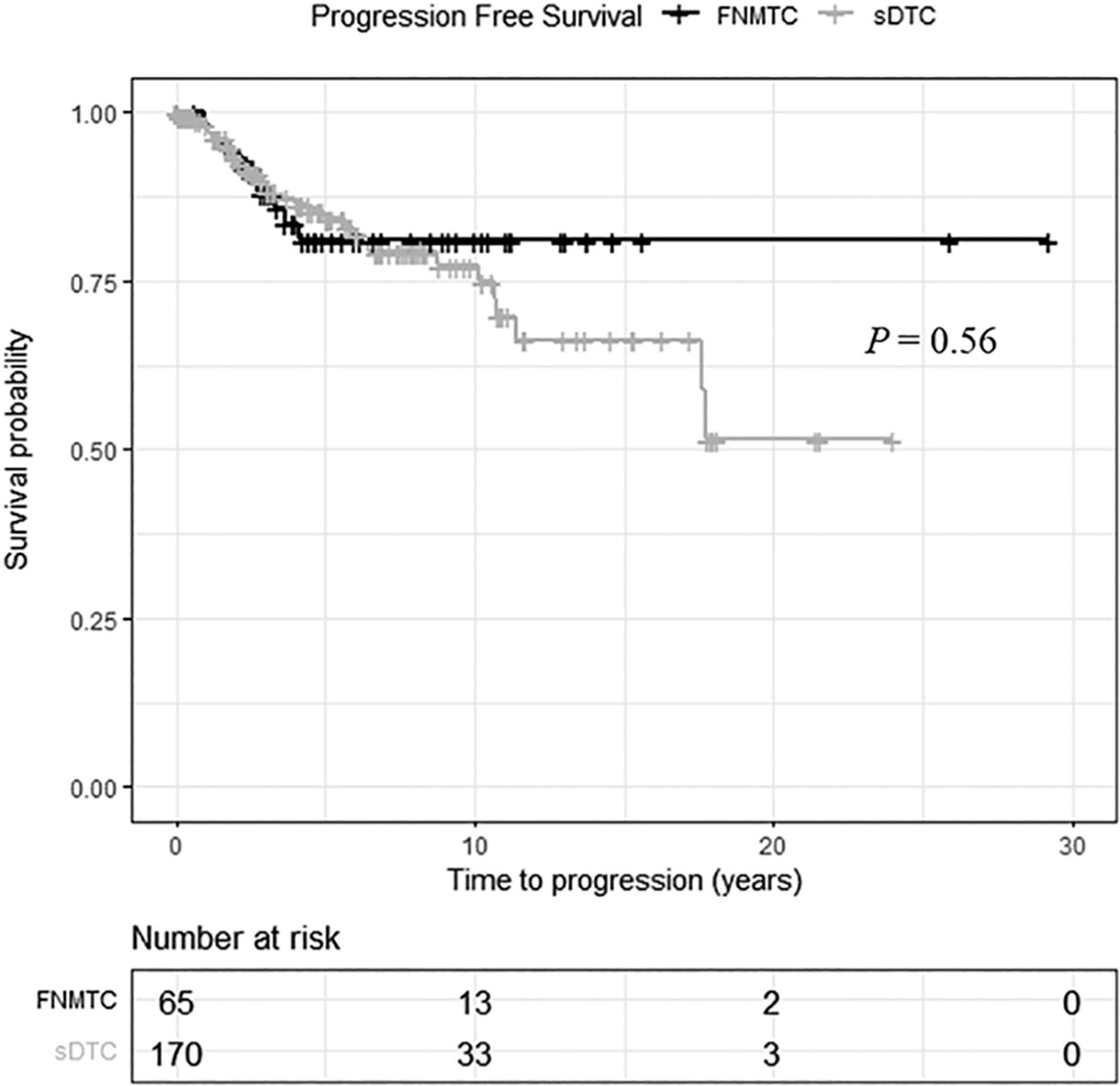
Progression free survival (PFS) curves of familial non-medullary thyroid cancer (FNMTC) and sporadic differentiated thyroid cancer (sDTC). PFS curves were similar (log-rank p = 0.56).
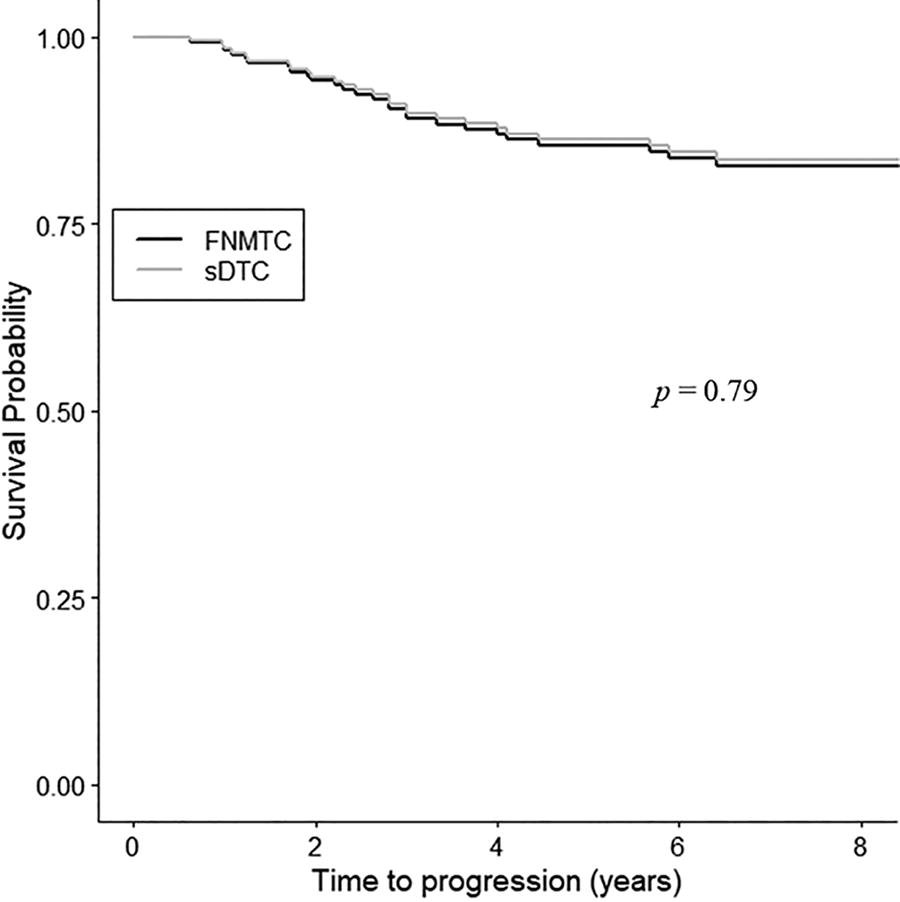
Progression free survival (PFS) curves of familial non-medullary thyroid cancer (FNMTC) and sporadic differentiated thyroid cancer (sDTC) after adjusting for cofounding factors. PFS remained not significantly different (PFS FNMTC vs. sDTC hazard ratio 1.13, 95% confidence interval 0.45–2.83, p = 0.79).
Multivariable Analysis of PFS in FNMTC and sDTC Patients Performed Using the Cox Proportional-Hazards Model Revealing That ATA-R High and Male Sex Are Associated with Worse PFS
Bold values indicate statistical significance at p < 0.05.
HR, hazard ratio; CI, confidence interval.
Since FNMTC in families with 3 or more members affected is more likely to have a genetic background as compared with the pedigrees with 2 affected members, 31 we next performed subgroup analysis focused on families with 3 or more members affected. PFS in this FNMTC subgroup showed no significant difference as compared with FNMTC families with 2 members affected and sDTC (log-rank p = 0.54, Fig. 4). Similarly, PFS between FNMTC and sDTC did not show a significant difference across different subgroups, including those with tumor size >1 cm (Supplementary Fig. S1A, B), the presence or absence of lymph node metastases (Supplementary Fig. S2A, B, S3A, B), the absence of aggressive histology (Supplementary Fig. S4A, B) and patients aged above and below the age of 55 years (Supplementary Fig. S5).
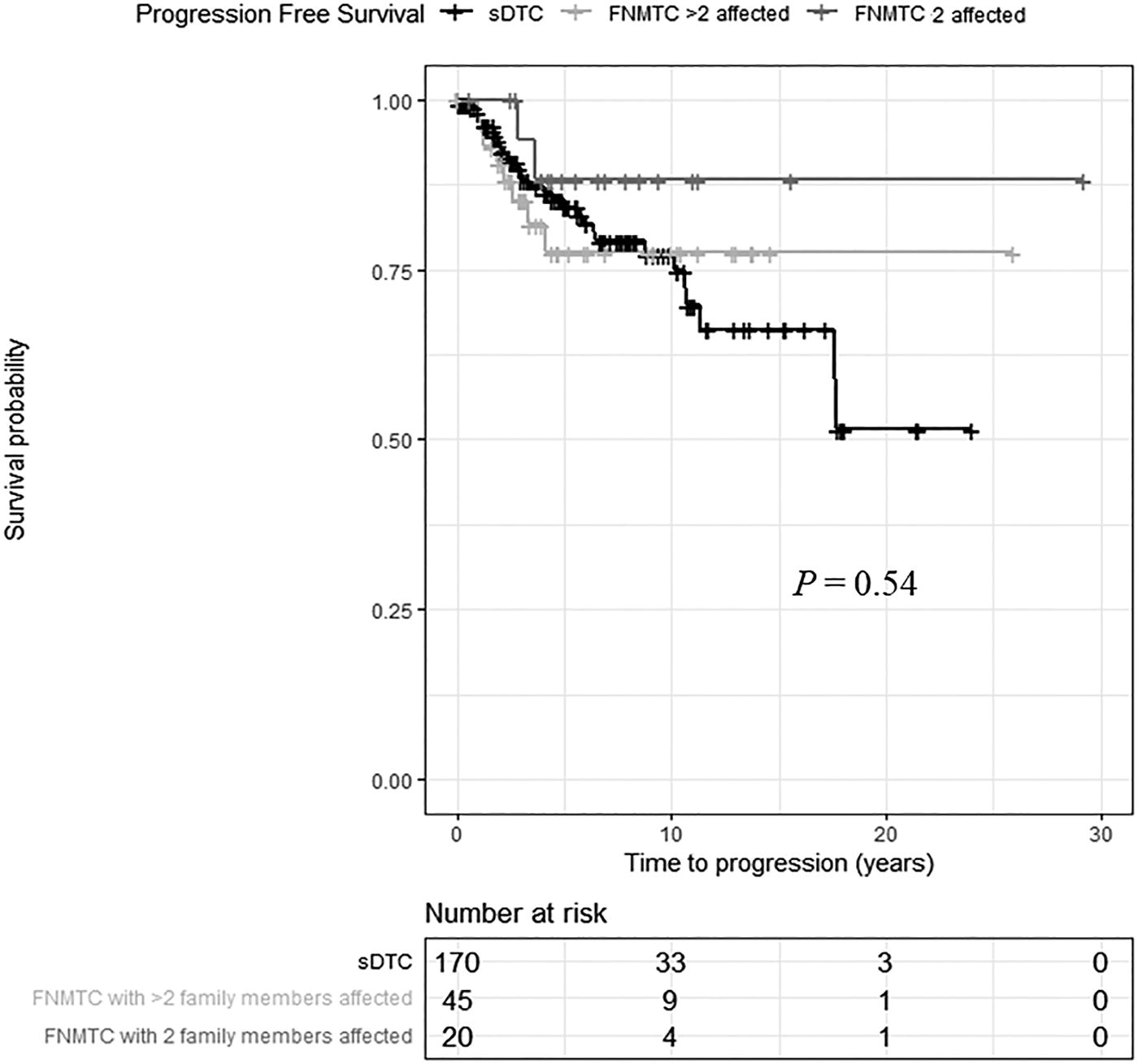
No significant difference in PFS in FNMTC patients with 3 or more affected family members compared to individuals belonging to families with 2 affected members and to sDTC (Log rank p = 0.54).
Discussion
This study suggests that PFS is not significantly different in patients with FNMTC compared to those with sDTC when treated with standard therapy. Interestingly, FNMTC patients presented with smaller tumors and fewer metastatic lymph nodes at diagnosis; that could possibly be attributed to active screening of affected families, with 39% of thyroid cancer detected by screening in our FNMTC cohort. Similarly, the smaller tumor size in the familial group may be attributed to the higher prevalence of microcarcinomas (≤1 cm) in FNMTC, which may have influenced the tumor size distribution compared to sDTC and, again, could have been a function of active screening.
The average age of FNMTC diagnosis aligned with previous studies, 8 –10,12 with one study suggesting an anticipation phenomenon, potentially leading to earlier diagnosis in subsequent generations (<45 years). 10 In order to control for potential anticipation phenomenon and earlier detection of FNMTC due to screening, we matched the FNMTC cohort with the sDTC group by age. Our study also included matching by sex, revealing a higher proportion of women than men in familial and sporadic cases, as typically observed in other matched cohorts. 8 –11
Importantly, we found a significant difference in ethnic origin between FNMTC and sDTC, suggesting that genetic or environmental factors linked to ethnicity may play a role in the pathogenesis of these subtypes. The absence of Hispanic or Latino individuals in the FNMTC cohort, compared to their 34.7% representation in the sDTC group, raises questions about potential protective genetic factors or disparities in healthcare access, early detection, or family history reporting. Data on FNMTC within Hispanic populations is limited; one study investigating the HABP2 G534E germline variant in a Hispanic cohort from Colombia found no significant association with DTC risk, suggesting that this variant is not a causative factor in this population. 15 Given the scarcity of studies focused on FNMTC in Hispanic groups, further research is essential to elucidate the genetic and environmental factors influencing its prevalence and characteristics.
Notably, our analysis revealed significant differences in histological type, particularly a higher proportion of classical PTC and a lower proportion of PTCTC in FNMTC compared to sDTC. A similar distribution has been reported in other matched case-control studies, where classical PTC is the most prevalent, followed by follicular variant PTC, and then PTCTC in the FNMTC cohort. 12 While there are rare reports of OCA associated with FNMTC, 8 OCA was not observed in our FNMTC cohort.
Contrary to some previous studies, 8,12,13,18,19 we observed no significant difference in multifocal tumor growth between FNMTC and sDTC. However, our findings were consistent with some matched case-control studies. 9,11 Due to matching by ATA-R, we have not observed significant differences in gross extrathyroidal extension or presence of locoregional or distant metastases that have been observed in some other studies. 12,32,33
We matched patients to control for the potential association of the extent of initial surgery on outcomes. Since the thyroid cancer management guidelines were changing over time, we also matched our cohorts by the year of initial therapy to assure that we were comparing similar management strategies. It was particularly important given the historical recommendation for an aggressive therapeutic approach due to perceived higher tumor aggressiveness and recurrence rates in FNMTC. 9,18 Our observation that both groups had a comparable prevalence of repeat neck operations and types of lymphadenectomy performed supports a notion of a similar response to standard treatment in familial and sporadic disease. Consistent with our findings, Afiei et al. found no significant difference in the frequency of repeat surgery between FNMTC and sDTC patients. 11 Other match-controlled studies do not specifically address the prevalence of repeat neck surgeries between groups. 8 –10,12
In our study, we observed no significant difference in RAI therapy utilization between FNMTC and sDTC groups. This corroborates with some studies, such as Shafiei et al., who found no difference in cumulative RAI dose between FNMTC and sDTC patients. 11 In contrast, other matched-controlled studies reported higher RAI utilization with higher RAI dosages in patients with FNMTC, 8,10 supporting the perception of a more aggressive clinical behavior of FNMTC by clinicians. 8 The fact that our study groups were comparable in RAI usage is likely associated with the matching by ATA-R that allowed appropriately similar RAI utilization per the ATA guidelines. The relatively high proportion of patients subjected to RAI might be due to its historical universal application, as our study included patients treated before the year 2000, when less selective RAI usage was implemented. 27
Response to therapy during the last follow-up visit, as categorized by the ATA recurrence risk stratification system 27 did not differ between both groups, suggesting similar treatment outcomes. During follow-up, 15.4% of FNMTC and 18.24% of sDTC patients experienced disease progression, with a lack of difference in PFS probabilities, indicating comparable treatment responsiveness. Controlling for cofounding factors using multivariable Cox regression analysis confirmed this observation. However, our study was powered to detect a 6.4% difference in 5-years PFS, so a smaller effect size may not have been captured. In our cohort, ATA high-risk patients demonstrated a markedly increased risk of progression as compared to lower-risk counterparts, confirming the ATA-R system’s validity. 26 Furthermore, males exhibited a substantially higher risk of progression relative to females, consistent with prior studies. 34 These observations are in line with other matched case-control studies showing no significant differences in DFS in FNMTC and sDTC patients. 9,10,12 Other studies revealed no differences in recurrence rates in FNMTC patients and no difference at the 2-year treatment response. 11,18 However, there are data showing a delayed achievement of an excellent treatment response in FNMTC cohort. 11 Some investigators found significantly shorter median DFS for patients in FNMTC compared with their matched controls, with worse outcomes for patients with more than two family members involved. 8 Uchino et al. found in their unmatched study significantly poorer DFS in FNMTC patients. 19 The differences in the above-mentioned studies could be explained by variable sample sizes with different power to detect certain effect sizes of the differences in outcome, variable matching methods or lack of control for bias, or heterogeneity of the studied population, to name just a few.
Limitations
Our study needs to be interpreted in the context of its limitations, namely a retrospective data analysis and a sample size sufficient to detect a 6.4% difference in 5-year PFS with 80% power and alpha of 0.05, based on a reference 5-year progression rate of 18% in sDTC. However, it is reasonable to assume that smaller differences are likely not relevant clinically. Moreover, the careful matching enabled reduction of some cofounding factors associated with this retrospective study design. The statistical power was evaluated only for PFS as the primary outcome, which may have limited the study’s ability to detect significant differences in other clinically relevant endpoints. Another limitation is the difficulty in interpreting the role of pathogenic somatic variants observed in a subset of FNMTC tumors, due to the small number of tissues subjected to molecular testing in this cohort. Furthermore, although no significant baseline differences were observed between FNMTC participants that were included and excluded from the analysis due to lack of follow-up data (Supplementary Table S1), the comparisons are limited by the small number of observations in the unknown follow-up group. Loss to follow-up was primarily due to international patients being unable to return, not due to mortality. This missing data may introduce bias, as potential differences in tumor characteristics remain uncertain.
Conclusion
In conclusion, our study found that patients with FNMTC, including those identified through active screening, exhibit non-different PFS compared to sDTC patients, suggesting comparable tumor biology and responsiveness to standard therapy. These findings suggest that the initial surgical treatment and utilization of RAI therapy for FNMTC should align with the standard of care for sporadic thyroid cancer, without necessitating more extensive surgery or higher RAI dosages for FNMTC.
Footnotes
Acknowledgments
The authors would like to thank the patients and their families for participating in our study, and the health care providers who cared for them at our institution and who referred them to our institution for evaluation through our clinical protocol. They thank Dr. Lee Weinstein for his critical review of the article. Additionally, they would like to thank Jesse Troy, PhD, and Dr. Liana Puscas, MD, MHS, from the Clinical Research Training Program at Duke University for their valuable input on the design and methodology of this project.
Authors’ Contributions
E.C. and J.K. are joint corresponding authors. J.K. conceived and designed the study. J.K., A.M., S.G., P.V., and C.C. supervised the study. N.U. performed data extraction of clinical variables from the Electronic Medical Records. N.H. confirmed and identified disease progression in the participants. S.K. was involved in the molecular profiling of the tumors. S.A. performed the statistical analysis. All authors contributed to the acquisition, analysis, or interpretation of the data. E.C. and J.K. drafted the article. All authors revised the report and approved the final version before submission. E.C. and J.K. are the guarantors and attest that all listed authors meet authorship criteria and that no individuals meeting the criteria have been omitted.
Data Sharing
All the data will be made available upon request to the corresponding author. Proposals will be reviewed and approved by the sponsor, investigator, and collaborators based on scientific merit. After approval of a proposal, data will be shared through a secure online platform after the signing of a data access agreement.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This research was supported by the Intramural Research Programs of the National Institute of Diabetes and Digestive and Kidney Diseases and the Center for Cancer Research, National Cancer Institute, National Institutes of Health. Clinical trial registration number: NCT-01109420. Principal Investigator: Joanna Klubo-Gwiezdzinska, intramural funding #ZIA DK047053-17.
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
Supplementary Figure S4
Supplementary Figure S5
Supplementary Table S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.