
Abstract
Background:
Intravenous glucocorticoids (IVGCs) are the first-line treatment for active moderate-to-severe thyroid eye disease (TED) in many countries worldwide, mainly because of their anti-inflammatory efficacy.
Methods:
Retrospective cohort study of 64 patients with active moderate-to-severe TED, without dysthyroid optic neuropathy, treated between 2003 and 2023 at a single tertiary centre with the 12 weeks IVGC EUGOGO (European Group on Graves Orbitopathy) protocol. All patients were evaluated for response to IVGC according to the clinical judgment (CL) and 44/64 (69%) patients were also evaluated with the EUGOGO 2021 revised composite index (CI).
Results:
The mean patients’ age at IVGC initiation was 51.7 ± 11 years, 47/64 (73.5%) were women, 56/64 (87.5%) were Caucasians, and 33/64 (51.5%) were active smokers. At 6 months after IVGC, 48 out of 64 (75%) patients evaluated with CL and 32 out of 44 (73%) patients evaluated with EUGOGO CI responded to the treatment. Nonresponders tended to be older than responders (56.6 ± 10.2 vs. 50.1 ± 10.8 years, p = 0.040 for CL and 56.5 ± 11.9 vs. 50.3 ± 11.6 years, p = 0.131 for EUGOGO CI) and had higher clinical activity score (CAS) before IVGC (5.0 ± 1.1 vs.4.2 ± 1.1, p = 0.022 for CL and 4.7 ± 0.6 vs. 3.1 ± 0.8, p < 0.001 for EUGOGO CI). In patients evaluated with CL or EUGOGO CI, respectively, multivariable logistic regression identified age at IVGC initiation (odds ratio [OR] = 0.92 [95% confidence interval (CI) 0.86–0.99], p = 0.024 and OR = 0.88 [CI 0.77–0.99], p = 0.046) and CAS before IVGC (OR = 0.53 [CI 0.31–0.90], p = 0.021 and OR= 0.08 [CI 0.01–0.38], p = 0.001) but not active smoking as independent factors associated with response to IVGC. The optimal cut-off associated with poorer response to IVGC was CAS ≥4.5/7 (66.7% specificity, 56.3% sensitivity; Area Under the Curve [AUC] = 0.689 [CI 0.54–0.83], p = 0.010) in patients evaluated with CL and CAS ≥3.5/5 (65.6% specificity, 91.7% sensitivity; AUC = 0.910 [CI 0.80–1.01], p < 0.001) in patients evaluated with EUGOGO CI.
Conclusion:
Older age and higher CAS before treatment were associated with poorer response to IVGC. Patients with these characteristics could be offered other immunotherapies as a first-line treatment for active moderate-to-severe TED.
Introduction
Active moderate-to-severe thyroid eye disease (TED) concerns up to 10% of patients with Graves’ Disease (GD). 1 One of the aims of treatment of active TED is to stop orbital inflammation and reduce subsequent orbital tissues remodeling. Glucocorticoids achieve this by inhibiting the activity of the proinflammatory cytokines and by decreasing the number and activity of circulating dendritic and plasma cells. 2 In addition, glucocorticoids have immunosuppressive actions, which may be relevant giving the autoimmune nature of TED. 3 Current European Group on Graves Orbitopathy (EUGOGO) guidelines recommend intravenous glucocorticoids (IVGCs) as a first-line treatment for active moderate-to-severe TED. 4 A 2022 consensus statement by the American Thyroid Association and European Thyroid Association suggested that IVGC should be the preferred treatment in these patients when soft tissue inflammation or diplopia are the prominent features. 5 The recommended IVGC treatment is a cumulative dose of 4.5 g methylprednisolone, given in 12 weekly infusions (six infusions of 0.5 g, followed by six infusions of 0.25 g), but higher dose up to a cumulative dose of 8 g/cycle can be administered in more severe cases. 4,5 The outcome of treatment is assessed 3–6 months after the last therapeutic intervention using standardized measures. 4 Recent surveys of professional thyroid societies confirm that IVGC is the most prescribed treatment for active moderate-to-severe TED worldwide, except in North America, due to its availability and low cost. 6,7 However, although patients receiving IVGC for TED can achieve an overall response rate of up to 80% in randomized controlled trials, 3 they are at risk of serious adverse events and the effect of this treatment on proptosis, a major disabling manifestation of TED and a determinant of patients’ negative feelings, 8 is very limited. 9 Moreover, about 20–41% of IVGC treated patients experience disease relapse. The emergence of new immunotherapies with different safety profiles and with a better improvement of diplopia and/or proptosis with comparable anti-inflammatory efficacy urges the identification of potential nonresponders to IVGC treatment.
The aim of our study was to determine factors associated with IVGC response in patients with active moderate-to-severe TED.
Material and Methods
This is a retrospective cohort study of 1631 patients with GD or TED seen at a single tertiary center between 2003 and 2023. Patients under 18, with hyperthyroidism caused by other conditions than GD and patients with dysthyroid optic neuropathy (DON) were excluded. The final analysis included 64 patients with active moderate-to-severe TED, treated with the 12 weeks IVGC EUGOGO protocol and for whom at least 6 months follow-up was available. Disease activity was based on CAS assessment and, whenever possible, orbital MRI. TED was considered active when CAS ≥3/7. The clinical features were presented on a per-patient basis and the most affected eye was considered. Figure 1 illustrates the study selection process in detail.
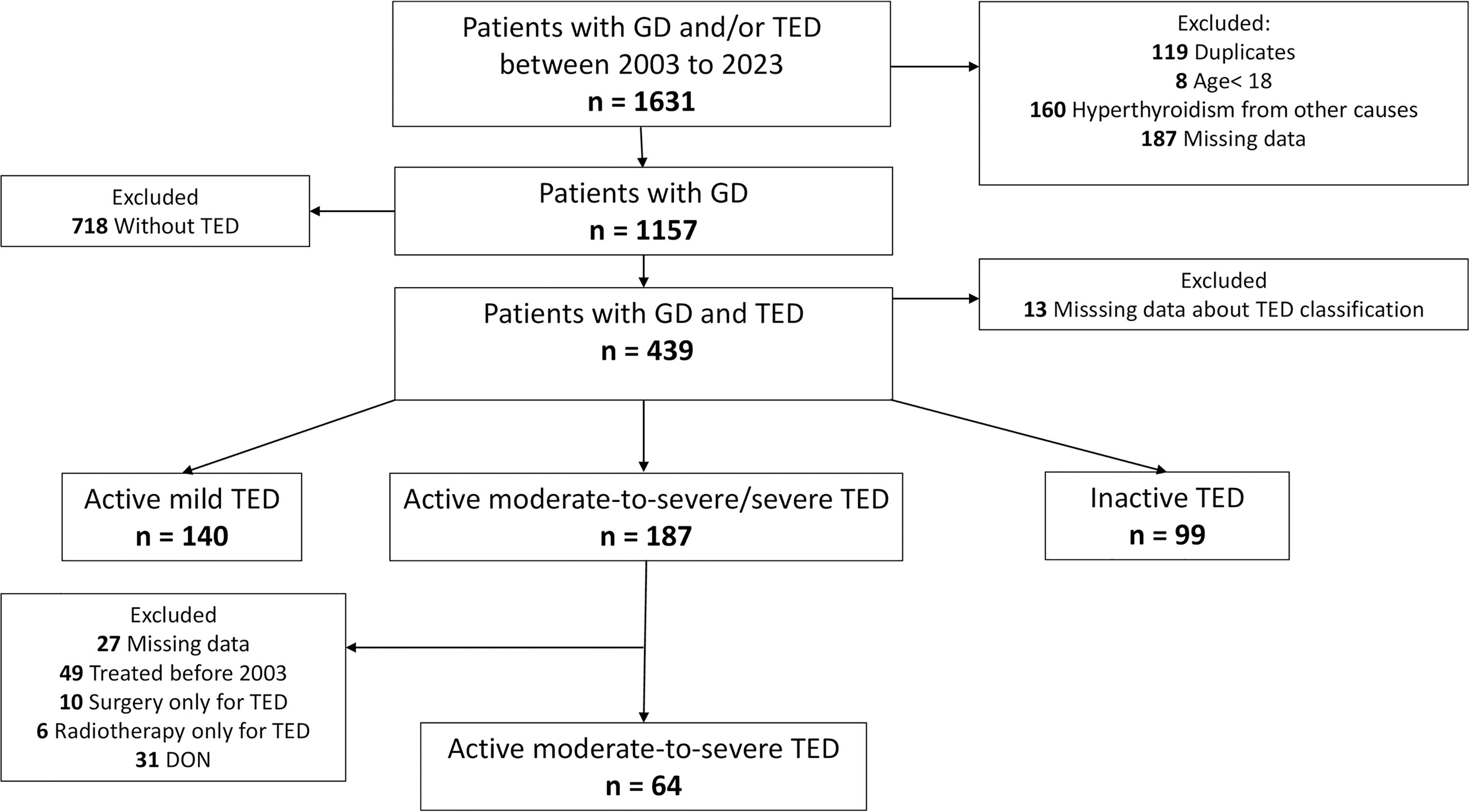
Flow chart of patients with active moderate-to-severe TED treated with the 12 weeks IVGC EUGOGO protocol. EUGOGO, European Group on Graves Orbitopathy; IVGCs, intravenous glucocorticoids; TED, thyroid eye disease.
IVGC treatment for TED and assessment of the response
All patients received six infusions of 0.5 g intravenous methylprednisolone once weekly, followed by six infusions of 0.25 g once weekly, except for one patient who received six infusions of 0.75 g, followed by six infusions of 0.5 g. The response to IVGC was evaluated 6 months after treatment, in all patients, according to clinical judgment (CL), with criteria that varied in time but took into account changes in CAS score, exophthalmos and ocular motility, but also the impact of the treatment on the capacity of the patient to resume his/her usual daily activities. The response to the treatment was also evaluated in 44 out of 64 (69%) patients with the EUGOGO 2021 revised composite index (CI): ≥2 mm reduction of lid aperture, ≥1 point reduction in five-item CAS (excluding subjective, patient-reported spontaneous or gaze-evoked pain), ≥2 mm reduction in exophthalmos, and ≥8° increase of eye muscle duction. Improvement in ≥2 features in one eye without deterioration in the other eye was considered as a positive response to treatment. 3 Patients needing additional treatments during the active phase or presenting TED reactivation during the 6 months after IVGC administration were considered nonresponders. The ophthalmological evaluation was performed by the same investigator.
Thyroid function tests and thyroid status at IVGC initiation
Before June 2014, TSH, free T4, and thyroid antibodies were measured with a chemiluminescent immunoassay (DXL, Beckman Coulter) and after June 2014 using an electrochemiluminescent immunoassay on a Cobas e602 analyzer (Roche Diagnostics). Thyrotropin receptor antibodies (TRAb) were measured by ELISA (Medizym, Medipan) between 2003 and 2016 and then by immunoassay (TRAK, Kryptor, Thermofisher) after 2016. Euthyroidism was defined as TSH and free T4 within reference ranges, hypothyroidism as TSH above upper normal range, and hyperthyroidism as TSH below lower normal range.
Statistical analyses
Statistical analyses were performed using the IPSS Statistics© software from IBM© (version 28.0). A p-value of less than 0.05 was considered significant. Continuous variables were described either as mean ± standard deviation or median with the percentiles 25 and 75. Discrete variables were described using their frequency. Subgroup analyses were performed using Pearson’s X2 test for categorial unpaired variables. For comparing continuous variables, we performed both nonparametric (Mann–Whitney U test) and parametric (analysis of variance) tests, with concordant results in terms of statistical significance. We selected the p-values based on the size of the groups, with nonparametric tests preferred if one or more groups was small (n < 30), and parametric tests if all groups compared were larger than n = 30. We performed univariable and multivariable logistic regression analyses (MVR) and a receiver operating characteristic (ROC) curve analysis to determine variables associated with the response to IVGC and their optimal cut-offs.
This study protocol was reviewed and a waiver for patient consent was approved by the local Ethics Committee (Comité d’Ethique Hospitalo-Facultaire des Cliniques Universitaires St-Luc, Université Catholique de Louvain, Brussels, Belgium, approval number 2023/08MAI/220, BE registration number B 403).
Results
Characteristics of patients evaluated with clinical judgment for response to IVGC
All 64 patients who received IVGC for moderate-to-severe TED were evaluated with CL for treatment response. Their characteristics are described in Table 1. TED was diagnosed at a median 1.0 (0.0–7.7) months after GD diagnosis and IVGC treatment was started at a median 4.0 (2.0–8.0) months after TED diagnosis. Only 8/56 (14%) of patients had more than 12 months duration of TED. At the time of TED diagnosis: 2/64 (3%) of patients had no treatment, 45/64 (70%) were on antithyroid drugs and 17/64 (26%) on levothyroxine only. The mean age at IVGC initiation was 51.7 ± 11 years, the majority of patients were Caucasian women, 51.5% active smokers and 6% were diabetics. Almost half of them (47%) had already been treated with selenium and 9% were taking statins. At the time of IVGC initiation, 34/64 (53%) patients were euthyroid, 22/64 (34.5%) were hyperthyroid, and 8/64 (12.5%) were hypothyroid. The majority of patients (89%) had bilateral TED and in half of them TED was present at GD diagnosis. The mean clinical activity score (CAS) before IVGC measured on a seven-point scale was 4.4 ± 1.2 and 73% of patients had CAS ≥4/7 at IVGC initiation.
General and Thyroid Eye Disease Characteristics of Patients Evaluated with Clinical Judgment for Response to Intravenous Glucocorticoid
Results are shown as mean ± standard deviation or median (percentile 25–75).
IVGC, intravenous glucocorticoids; GD, Graves’ disease; TgAb, thyroglobulin antibodies; TPOAb, thyroperoxidase antibodies; TRAb, thyrotropin receptor antibodies; +, positive; ULN, upper normal limit; TED, thyroid eye disease; CAS/7, 7-points scale clinical activity score.
Response to IVGC of patients evaluated with clinical judgment
Among patients evaluated with CL, 48/64 (75%) responded to the treatment. There were no differences in term of sex, ethnicity, thyroid function at IVGC initiation, changes in TRAb levels, or the time between the diagnostic of GD and the diagnostic of orbitopathy or the time to the treatment of TED between responders and nonresponders (Table 2). Responders were younger at IVGC initiation (mean age 50.1 ± 10.8 vs. 56.6 ± 10.2 years, p = 0.040) and smoked less (33% vs. 12.5% never smoked, p = 0.047), compared with the nonresponders. There were more thyroperoxidase antibodies positive patients among the nonresponders (12/16 (7%) vs. 22/46 (48%), p = 0.06) but the thyroglobulin antibodies prevalence was not different. Diabetes and statin use were not different between responders and nonresponders.
General and Thyroid Eye Disease Characteristics of Responders and Nonresponders to Intravenous Glucocorticoid Evaluated with Clinical Judgment
Results are shown as mean ± standard deviation or median (percentile 25–75); in bold: p value <0.05 considered significant.
Nonresponders had higher CAS score before IVGC than the responders (5.0 ± 1.1 vs. 4.2 ± 1.1, p = 0.022) and there were more patients with CAS ≥4/7 before treatment among nonresponders (15 [94%] vs. 32 [67%] patients, p = 0.034), as showed in Table 2. Higher CAS scores persisted in nonresponders after IVGC (81% of nonresponders had CAS ≥3/7 vs. no patient in the responders group, p < 0.001).
The nonresponders received more often than responders oral glucocorticoids before IVGC and more often orbital radiotherapy, second line immunotherapy, or orbital decompression during the active phase of TED in case of IVGC failure (p < 0.001 for all) (Supplementary Table S1). There was no difference between responders and nonresponders regarding a previous treatment with selenium (Supplementary Table S1).
Characteristics of patients evaluated with EUGOGO CI for response to IVGC
Among the 64 patients, there were enough data to evaluate the response to IVGC with EUGOGO CI in 44 patients. Patients who could not be evaluated with the EUGOGO CI had similar general, thyroid disease and TED characteristics as the population evaluated with these criteria, with the difference that orbitopathy was more frequently bilateral in patients with EUGOGO CI (unilateral/bilateral 1 (2%)/43 (98%) vs. 6 (30%)/14 (70%), p = 0.001). In particular, the CAS score on a seven-point scale before IVGC was not different between the EUGOGO CI group and the other patients (4.4 ± 1.1 vs. 4.2 ± 1.2; p = 0.489). Asymmetrical TED, defined as disease present in both eyes with one or more of the following features: a difference between the two eyes in exophthalmometer readings by two or more mm; difference in palpebral aperture by two or more mm, difference in eyelid swelling by one or more grades; difference in eyelid erythema by one or more grades; difference in conjunctival redness by one or more grades, was present in 12/44 (47%) of patients.
Response to IVGC of patients evaluated with EUGOGO CI
Among patients evaluated with EUGOGO CI, 32/44 (73%) responded to IVGC treatment. Responders versus nonresponders characteristics were similar to those of the patients evaluated with CL. Although the differences regarding the age at IVGC initiation and smoking were no longer statistically significant, there were more active smokers among nonresponders than responders (66% vs. 44%, p = 0.302) (Table 3). There were no significant differences between responders and nonresponders regarding asymmetrical TED (17/32 (53%) vs. 3/12 (25%), p = 0.095) (Supplementary Table S2). The response of the individual ocular parameters (lid aperture, exophthalmos, eye ductions, and CAS) according to 2021 EUGOGO CI was significantly better in responders (p < 0.05 for all, at the exception of muscle duction) and its amplitude is described in the Supplementary Table S2.
General Characteristics of Responders and Nonresponders to Intravenous Glucocorticoid Evaluated with European Group on Graves Orbitopathy Composite Index
Results are shown as mean ± standard deviation or median (percentile 25–75).
CI, composite index; EUGOGO, European Group on Graves Orbitopathy; CAS/5, 5-point scale clinical activity score.
Like the patients evaluated with CL, nonresponders according to the EUGOGO CI had higher CAS before IVGC measured on a five-point scale than responders (4.7 ± 0.6 vs. 3.1 ± 0.8, p < 0.001) and all had CAS ≥3/5 at IVGC initiation (Table 3).
Factors associated with response to IVGC
In the univariable logistic regression analysis, CAS score before IVGC and age at IVGC initiation were factors associated with response to IVGC in patients evaluated with CL (p = 0.027 and p = 0.050, respectively), while TRAb before IVGC, active smoking, and time to TED diagnosis were not (Table 4). Only CAS before IVGC was associated with the response in the univariable logistic regression analysis when patients were evaluated with EUGOGO CI (p = 0.001) (Table 5). CAS before IVGC and age at IVGC initiation were associated with response in MVR both in patients evaluated with CL or EUGOGO CI, in a model including active smoking as variable (Tables 4 and 5).
Uni- and Multi-variable Logistic Regression Analysis of Factors Influencing the Response to IVGC in Patients Evaluated with Clinical Judgment
Values are odds ratio with Cls.
CI, 95% confidence interval; OR, odds ratio; in bold: p value <0.05 considered significant.
Uni- and Multi-variable Logistic Regression Analysis of Factors Influencing the Response to Intravenous Glucocorticoid in Patients Evaluated with European Group on Graves Orbitopathy Composite Index
Values are odds ratio with 95% confidence intervals; in bold: p value <0.05 considered significant.
ROC curve analysis showed that the optimal cut-off associated with poorer response to IVGC was a CAS ≥4.5/7 before IVGC, when the response was assessed with CL (66.7% specificity, 56.3% sensitivity; Area Under the Curve [AUC] = 0.689 [95% confidence interval (CI) 0.54–0.83], p = 0.010) or CAS ≥3.5/5 when the response was assessed with the EUGOGO CI (65.6% specificity, 91.7% sensitivity; AUC = 0.910; [CI 0.80–1.01], p < 0.001) (Fig. 2A and B).
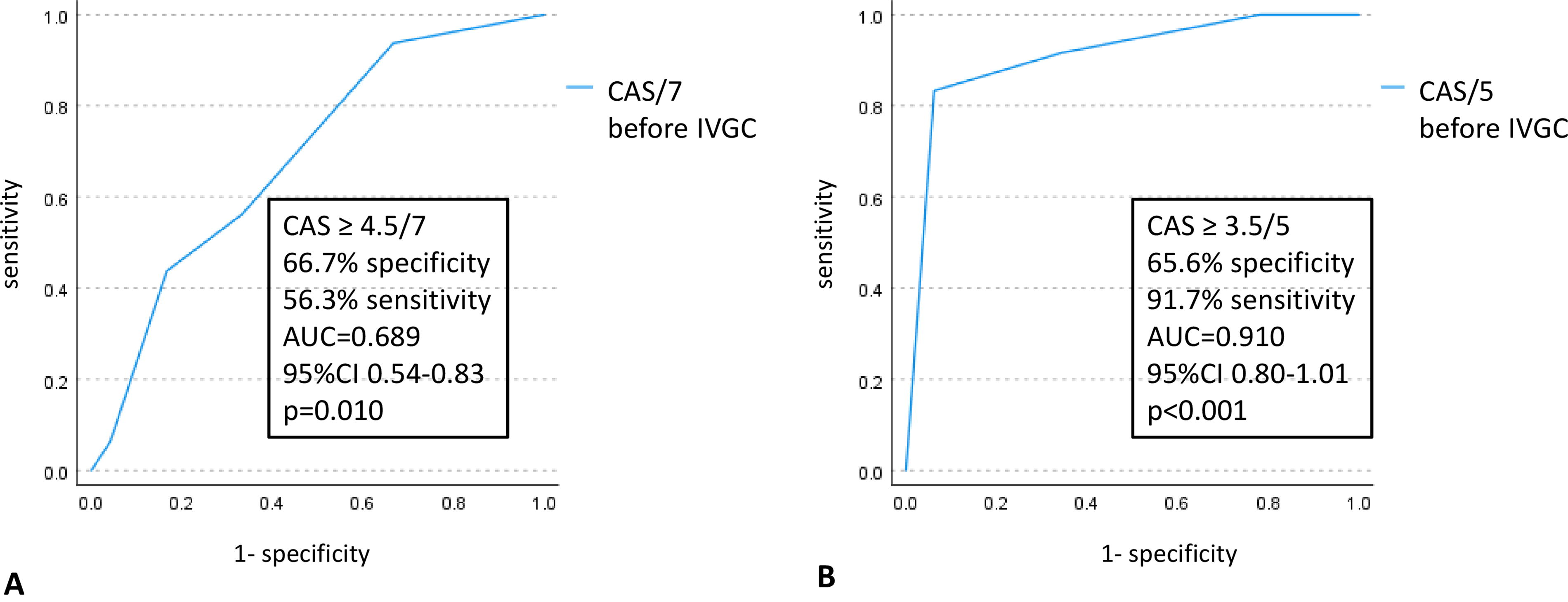
ROC curve for the CAS score associated with a poor response to IVGC in patients evaluated with CL
Discussion
This study shows that the response rate to IVGC as first-line treatment for active moderate-to-severe TED is similar to that previously reported by some studies 10 –13 but different than in others. 14 –17 The comparison of different studies is difficult due to the different study design, the utilization of different IVCG protocols, the evaluation of outcome(s) with different criteria, and the inclusion of patients with different clinical characteristics. In particular, when only changes in CAS are assessed as primary outcome, this may not entirely reflect proliferative manifestations of the disease resulting in proptosis and diplopia, complications that considerably impact patients’ quality of life (QoL). 8,18 The utilization of a CI as primary outcome, especially of the revised CI proposed by EUGOGO in 2021 has the advantage to describe the overall changes in the different components of TED using objective criteria. 19 In order to reduce the bias related to the use of different criteria for evaluating the response to the treatment, we studied our population with two criteria, of which one is currently recommended by the international guidelines and found similar response rates and factors associated with response.
Several clinical, biological, and imaging markers associated with insufficient response to glucocorticoids have already been discussed in the literature, 20 among them smoking, 21,22 the CAS, 12,13,15,23 older age, 16 higher baseline TRAb levels 10,11,16,24 and longer duration of TED. 15 In our study, of all these variables included in univariable analysis, only CAS before IVGC and age at IVGC initiation were associated with the response to treatment in MVR.
In contrast to our findings, higher baseline CAS was associated with a good response after oral GC 23 and in some studies with IVGC, 12,13,15 but not all. 10,11,17 In our study, higher CAS before treatment, particularly CAS ≥4.5/7 or CAS ≥3.5/5 was associated to poorer response to IVGC according to the method used to assess the response. Higher CAS was associated with a high risk of poor IVGC response (odds ratio [OR] 2.530 [1.246–5.136], p = 0.010) in 93 South Korean patients with CAS ≥4/7 at diagnosis, treated with the cumulative 4.5 g IVGC EUGOGO protocol and in whom a response, defined as obtention of CAS <3 and no symptoms of recurrence were seen in 78% of patients at 3 months. 11 Interestingly, high baseline CAS (cut -off >5/7; 40.2% sensitivity, 94.1% specificity) was associated with unresponsiveness to IVGC in patients with DON. 25 CAS was introduced in the 80’s by Mourits et al 26 as a measure of disease activity and a potential predictor of response to anti-inflammatory treatment 27 and the seven-points scale CAS was used in many studies as a primary treatment outcome. However, the clinical relevance of CAS score is challenged by its binary interpretation (absent/present) that does not allow severity grading, the fact that all features are given equal weighting and were established only in Caucasian patients and by the interobserver variability. 27 A number of recent publications advocate the need for improving the performance of the CAS or searching other methods to assess activity of the disease. More recently, EUGOGO suggested a five-point scale for CAS evaluation and removed the points related to subjective symptoms as spontaneous retrobulbar pain and pain on attempted upward or downward gaze. 4 Should CAS be predictive of response to IVGC, this may question the place of this treatment in first line for patients with high baseline CAS. On the other hand, there is no study to date to prospectively compare the response to IVGC versus other immunotherapies according to different baseline CAS scores.
In our study, older patients responded less to IVGC, irrespectively of the criteria used for evaluation. Older age was also a risk factor for poorer response to IVGC of Korean patients with active moderate-to-severe TED. 16 This could be explained by the fact that older patients, especially men, present more severe forms of TED, 28 including DON. As for CAS, the published studies lack analysis of response to IVGC stratified by age group.
Smoking is a well-known risk factor for TED occurrence and progression. 4 In a post-hoc analysis of a randomized study, radioiodine-associated progression of TED was more frequent in smokers than in nonsmokers. 29 However, the impact of (active) smoking on the efficacy of steroids is more controversial. Some studies showed that smokers have a delayed or worse response to oral 21 or intravenous steroids, 22 whereas some did not. 15 In the EUGOGO study of the response to three different IVGC doses for active moderate-to-severe TED assessed with a composite score, age, gender, smoking, TRAb levels, or the duration of TED were not related to treatment efficacy. 14 In our study, active smoking was not related to the response to IVGC in a MVR model including CAS and age at IVGC initiation, possibly due to the small sample size and different definition of smoking status.
In a recent EUGOGO study asymmetrical TED, defined by the presence of one or more criteria, including unilateral DON, accounted for 31% of the cohort, and asymmetry was associated with more severe and active TED than bilateral or unilateral TED. 30 In our series, asymmetrical TED does not seem to be associated with a poorer response to IVGC, but our findings might be biased by the definition of asymmetrical TED and inclusion of a different TED population than in the study by Perros et al. 30
We, as well as other studies 13,15,17 were not able to show an association between TRAb levels and response to IVGC. TSH receptor is not the only autoantigen involved in TED pathogenesis and TRAb circulating levels might not completely reflect the immune changes within the orbit, although they were generally related to TED activity and severity. 31 Moreover, TRAb activities might be different at thyrocytes and orbital fibroblast level. 32
Longer duration of TED exceeding 12 months was associated to poorer response to IVGC. 14 In our study, duration of TED was not associated to response to the treatment, possible because of rather early diagnosis during the course of the disease, both in responders and nonresponders.
The variability of individual predictive capability of treatment response of different markers pointed out the need for TED prediction models for treatment response resulting from the combination of clinical, biological and imaging markers. A recent meta-analysis of predictive models for IVGC response in TED concluded that one of the most robust and reliable prediction models incorporate multivariable regression analysis of clinical characteristics combined with laboratory indexes and/or imaging metrics. 33 From this perspective, our study has the strength of including most of the clinical markers related to IVGC response (age, smoking, time to TED diagnosis, CAS), several biological markers including TRAb and to assess the response to treatment in a multivariable model. It is also one of the rare studies analyzing these factors in a predominantly Caucasian population, this ethnic group being more often concerned by TED occurrence. 34 Our findings are strengthened by the fact that we found the same factors associated with response using two different assessment methods, of which one recommended by the current international guidelines. 4,5
Our study has several limitations. Our conclusions concern mostly Caucasian patients, although similar data for age and CAS at IVGC initiation were published in Asian patients assessed with different response criteria. 11,16 Due to the retrospective nature of our study, some data were not available in all patients and could not be analyzed, especially the lipid profile, hypercholesterolemia being one of the biological markers that has been recently related to a poorer response to IVGC. 35,36 We did not include in our analysis imaging data. More importantly, our patients were not evaluated for QoL changes with a standardized tool (ex GO-QoL), subjective patient-reported outcomes being part of the currently recommended evaluation of the response to treatment, together with objective clinician-reported outcomes. 4,5
Conclusions
In a predominantly Caucasian population with active moderate-to-severe TED treated with the 12 weeks IVGC EUGOGO protocol, older age and higher CAS before treatment were associated with poorer response to IVGC, irrespective of the method used to evaluate the response to the treatment. Patients with these characteristics could be offered other immunotherapies as a first-line treatment for active moderate-to-severe TED. Further studies comparing the efficacy of IVGC while stratifying patients for age and CAS score are needed.
Footnotes
Authors’ Contributions
M.C.B.: Conceptualization (lead); writing—original draft (lead); and writing—review and editing (equal). N.B.: Conceptualization (supporting) and writing—review and editing (equal). O.A.: Formal analysis (lead) and writing—review and editing (equal). S.C.M.: Formal analysis (supporting) and writing—review and editing (equal). C.D.: Writing—review and editing (equal). M.C.: Writing—review and editing (equal). A.B.: Conceptualization (supporting) and writing—review and editing (equal).
Author Disclosure Statement
M.C.B., C.D., M.C., and A.B. are members of EUGOGO. N.B., O.A., and S.M.C. have no disclosures to declare.
Funding Information
No funding sources to declare.
Supplementary Material
Supplementary Table S1
Supplementary Table S2