
Abstract
Background:
Factors contributing to the development of reproductive concern, fertility intention and pregnancy outcomes in young women following thyroidectomy are unclear. This study aimed to compare the reproductive concern, fertility intentions and pregnancy outcomes between young women who had either thyroid cancer (TC) or benign thyroid disease and were treated with total thyroidectomy (TT) or thyroid lobectomy (TL).
Methods:
This prospective cohort study enrolled women aged 20–40 and scheduled for thyroid surgery at a tertiary hospital in China from November 2019 to October 2021 (ChiCTR1900027205). Reproductive concern and intention were evaluated preoperatively and at 1, 3, 6, 12, 18, and 24 months postoperatively using Reproductive Concerns After Cancer (RCAC) and Fertility Intention Scale (FIS), respectively. Pregnancy outcomes were monitored.
Results:
Of the 482 eligible women, 402 women had TC (157 [39.1%] underwent TT), and 80 had benign thyroid disease (10 [12.5%] underwent TT). Compared with the benign group, the TC group had significantly higher RCAC scores from 3 months to 2 years postoperatively (all p < 0.05). The TC group had significantly lower postoperative FIS scores from 3 to 12 months after surgery than the benign group (all p < 0.05). Women with TC in the TT group had significantly higher RCAC scores than TL group at time points from 1 months to 2 years postoperatively, and had significantly lower postoperative FIS scores from 1 to 18 months after surgery (all p < 0.05). During the 2-year follow-up, 78 women became pregnant and 13 (16.7%) suffered pregnancy loss. No significant differences in adverse pregnancy outcomes were found between the TC group and benign thyroid disease group, or those between the TT group and the TL group of women with TC. Women with planned pregnancy and preconception counseling had significantly lower rates of pregnancy loss than those with unplanned pregnancy and no preconception counseling (4.0% vs. 22.6% and 11.7% vs. 33.3%, both p < 0.05).
Conclusions:
It is important to address reproductive concern and fertility intention postoperatively in young women with TC. Preconception counseling and planned pregnancy may be associated with a reduced risk of pregnancy loss after thyroid surgery.
Introduction
Thyroid cancer (TC) is one of the most common malignant tumors in women. In the United States, TC is expected to become the second leading malignancy in women by 2030. 1 In China, the age-standardized incidence rate of TC was the highest of female malignant tumors. 2 Approximately 45.6% of Chinese patients with TC were diagnosed between ages 20 and 40 years. 3 In general, differentiated thyroid cancer (DTC) is the most common type of TC and its overall survival rate and disease-specific survival rate of DTC is 92% and 99%, respectively. 4,5 For young women, the diagnosis and treatment of TC may potentially alter their fertility plans. 6 Given the good prognosis, the reproductive concerns and intentions of young women with TC should be addressed during treatment and follow-up.
However, the fertility issues of young adult patients with cancer have not been given sufficient attention in clinical practice. 7 In a Swedish survey, 48% of young female cancer survivors reported that they received information about fertility during treatment, and only 14% received guidance on fertility. 8 Unaddressed reproductive concern and intention affected the general quality of life and contributed to decisional conflict regarding posttreatment fertility among young adult female cancer survivors. 9 A comprehensive understanding of the reproductive concern and intention of young women with cancer will help clinicians provide more effective medical care, psychological counseling, and fertility guidance. However, no studies have focused on reproductive concern in young women with TC.
Thyroid hormones play a critical role in the maintenance of maternal health and the development of the fetus during pregnancy. 10 Both hypothyroidism and hyperthyroidism in pregnancy may lead to adverse outcomes. 11 –13 The risk of hypothyroidism during pregnancy increased in women with TC who underwent total thyroidectomy (TT) or thyroid lobectomy (TL), while postoperative thyrotropin (TSH) suppression therapy may lead to hyperthyroidism during pregnancy. 14 Moreover, in order to reduce the risk of recurrence, some women with DTC need radioactive iodine treatment after surgery, which may impair ovarian reserve. 15 –17 All of the treatments for TC can trigger reproductive concerns in young female patients. Although there have been several previous retrospective studies showing that a history of TC with treatment does not increase the risk of adverse pregnancy outcomes, 18 –20 prospective studies have not addressed the association between a history of treatment for TC and adverse pregnancy outcomes in women.
Therefore, we conducted a prospective cohort study to compare the reproductive concerns, fertility intentions, and pregnancy outcomes after thyroid surgery in young women with TC and those with benign thyroid disease, and to investigate factors that might influence adverse pregnancy outcomes.
Methods
Design and population
This prospective cohort study was conducted at the First Affiliated Hospital of Sun Yat-sen University, China. Women were enrolled from November 2019 to October 2021. The inclusion criteria were: (1) women aged 20–40 years; (2) underwent thyroid surgery; (3) surgical pathological findings indicative of DTC or benign thyroid disease. Exclusion criteria were: (1) other concurrent malignant tumors; (2) a history of infertility; (3) prior thyroid surgery; (4) severe cardiovascular disease, hepatic or renal disease, and autoimmune disease or immunodeficiency other than thyroid autoimmune disease; (5) severe mental illnesses; (6) poor compliance per investigators evaluation. The study was approved by the Ethics Committee of the First Affiliated Hospital of Sun Yat-sen University (Approval No. [2019] 389) and registered in the Chinese Clinical Trial Registry (ChiCTR1900027205). Written informed consent was obtained from all participants.
Data collection
All women completed a preoperative questionnaire including baseline characteristics. Following surgery, surgical approaches, pathological types, and postoperative levothyroxine dose were collected from medical records. All women enrolled were asked to complete an online version of routine postoperative questionnaire and scales at 1, 3, 6, 12, 18, and 24 months postoperatively. All questionnaires and scales were sent via WeChat, text message, or email at each follow-up time point. For those who did not respond within 1 week, the questionnaires and scales were sent again via the above methods and a telephone reminder was given in order to increase the response rate. All participants were followed up at the next scheduled time, regardless of whether they had responded at the previous time. All eligible women completed two scales at preoperative and each postoperative follow-up time point: The Reproductive Concerns After Cancer (RCAC) 21 and Fertility Intention Scale (FIS). 22 Both scales were available in Chinese language and validated in Chinese women. 23,24 RCAC included 18 items and six subscales to evaluate different dimensions of reproductive concerns: fertility potential, partner disclosure, child’s health, personal health, acceptance of possibly infertility, and becoming pregnant. Total scores ranged from 18 to 90 points, and high score indicated a greater level of concern. The 15-item FIS included four subscales to evaluate different dimensions: pregnancy risk, disease control, social support, and happiness. Total scores ranged from 15 to 75 points, and a high score indicated a more positive fertility intention. A detailed description of the above scales can be found in the Supplementary Data. If pregnancy was confirmed during follow-up visits, RCAC and FIS scales were not sent at the subsequent visits. Pregnancy-related data were collected. The detailed information of preoperative questionnaire, routine postoperative questionnaire, pregnancy-related questionnaire, and preconception counseling topics are presented in the Supplementary Data. The information of planned pregnancy included: (1) measurements of thyroid function, liver function, kidney function, and neck ultrasound; (2) adjustment of levothyroxine dosage to achieve the targeted TSH according the risk stratification of 2015 American Thyroid Association guidelines 4 ; (3) other beneficial preparations for pregnancy, such as weight loss for obese or overweight women, folic acid and vitamin supplements, quitting smoking of cigarettes and avoiding alcohol.
Exposures and outcomes
The primary outcomes included postoperative reproductive concern scores and fertility intention scores. Pregnancy outcomes after thyroidectomy were considered as secondary outcomes. Differences in postoperative reproductive concern scores and fertility intention scores were analyzed using TC or benign thyroid disease, and TT or TL for TC as exposure factors, respectively. When analyzing pregnancy outcomes, exposure factors were defined as TC or benign thyroid disease, TT or TL, planned pregnancy or not, and preconception counseling or not. The adverse pregnancy outcomes included pregnancy loss, preterm delivery, gestational diabetes mellitus, pregnancy-induced hypertension, eclampsia/preeclampsia, congenital malformations, fetal distress, large size for gestational age, and small size for gestational age.
Statistical analysis
Since China had not yet implemented the “Three-Child Policy” at the time of recruitment, women who had already given birth to two children or more were not included in the statistical analysis in order to avoid the influence of policy factors on fertility intentions. The preplanned analyses included: (1) to compare postoperative reproductive concern scores, fertility intention scores, and pregnancy outcomes between women with TC and those with benign thyroid diseases; (2) to compare postoperative reproductive concern scores, fertility intention scores, and pregnancy outcomes between women with TC undergoing TT and those undergoing TL; (3) to analyze the association of planned pregnancy and preconception counseling on pregnancy outcomes. The impact of specific pregnancy time periods after thyroid surgery on pregnancy outcomes was a post hoc analysis.
Continuous variables consistent with a normal distribution were described using mean (standard deviation [SD]). The Student t-test was used for two-group comparisons, and one-way analysis of variance was used for multiple comparisons. Nonnormally distributed continuous variables were described as median (interquartile range [IQR]). Mann-Whitney U test was used for two-group comparisons, and Kruskal-Wallis H test was used for multiple comparisons. Categorical variables were described as frequency (percentage). The χ2 test or Fisher exact test was used for intergroup comparisons. All the analyses were performed using SPSS version 25.0 (IBM Corporation, Armonk, NY, USA). A two-sided p-value <0.05 was considered statistically significant.
Results
Participant characteristics
A total of 482 women aged 20–40 years and scheduled for thyroid surgery were included in the analysis (Fig. 1 and Supplementary Table S1 in Supplementary Data). Respectively, 465 (96.5%), 471 (97.7%), 482 (100%), 480 (99.6%), 481 (99.8%), and 480 (99.6%) women responded to the questionnaires at 1, 3, 6, 12, 18, and 24 months after surgery. The 33 nonresponders were missed at only one follow-up time point. None of enrolled women was completely lost to follow-up after thyroid surgery. The cumulative number of pregnancies during the 2-year postoperative follow-up period was 78 (16.2%) in 482 women.
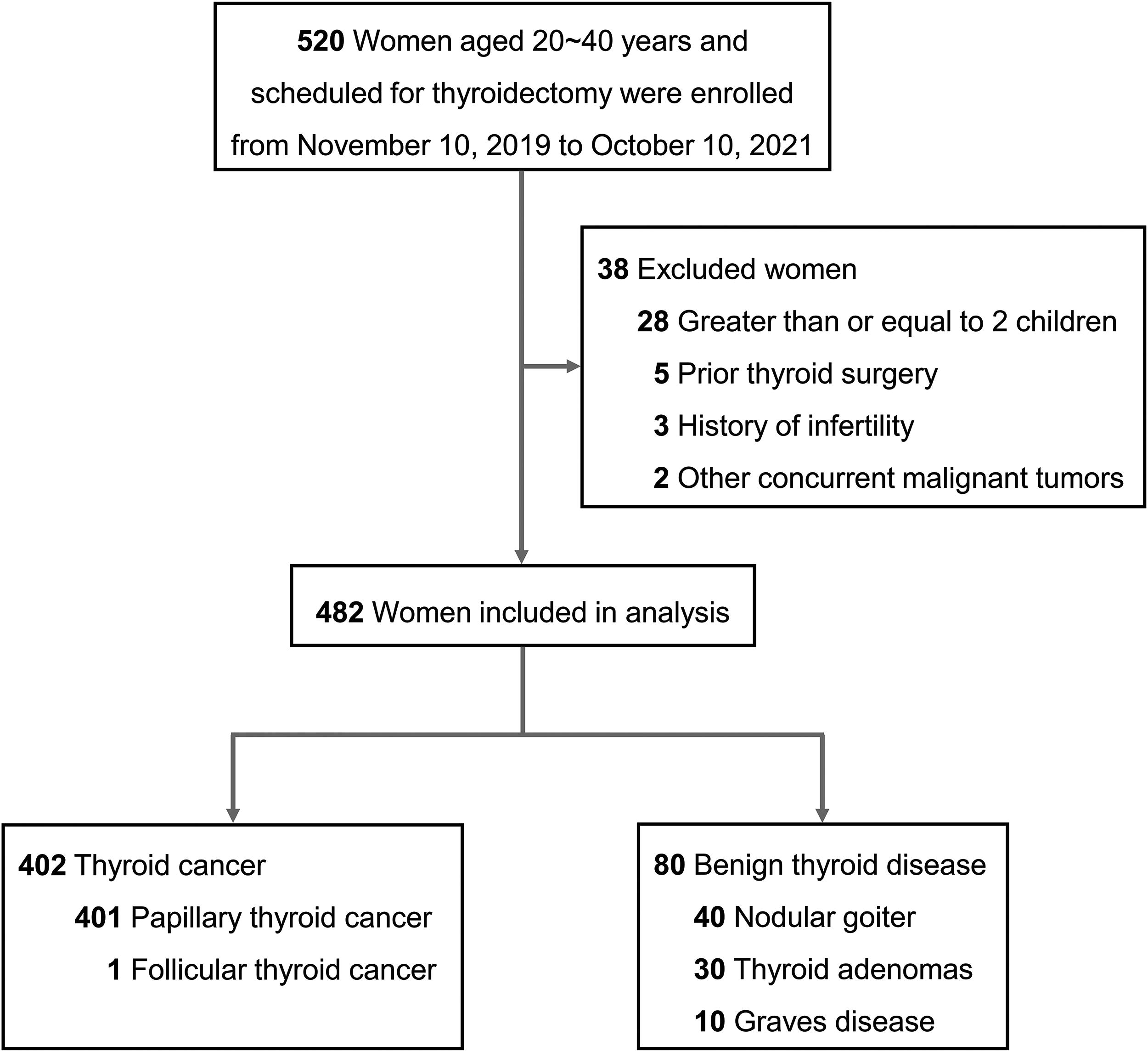
Diagram of the data collection process.
Of the 482 eligible women, 402 were confirmed as having TC (all DTC), and 80 were confirmed to have benign thyroid disease by postoperative pathology. In the TC group, 157 women underwent TT (39.1%) and 245 underwent TL (60.9%). The baseline characteristics of groups are reported in Table 1 and Supplementary Table S2 in Supplementary Data.
Characteristics of Participants
Risk of recurrence was evaluated based on the 2015 ATA Initial Risk System.
IQR, interquartile range; RAI, radioactive iodine; SD, standard deviation; TC, thyroid cancer; TL, thyroid lobectomy; TT, total thyroidectomy.
Comparison of RCAC and FIS scores between TC and benign thyroid disease
RCAC scores and FIS scores of women in the TC group and benign group are shown in Figure 2a, b. Compared with the benign group, the TC group had significantly higher RCAC scores at time points from 3 months to 2 years postoperatively (60.1 ± 6.5 vs. 58.1 ± 4.7, 65.5 ± 5.4 vs. 61.4 ± 8.6, 66.6 ± 6.4 vs. 57.4 ± 6.3, 52.6 ± 9.0 vs. 49.9 ± 6.1, and 52.9 ± 7.5 vs. 50.8 ± 4.5, respectively, all p < 0.05). RCAC scores of TC group reached the peak at 1 year postoperatively. The TC group had significantly lower postoperative FIS scores from 3 to 12 months after surgery than the benign group (46.9 ± 3.8 vs. 49.3 ± 3.0, 44.1 ± 3.2 vs. 49.0 ± 3.9, and 40.7 ± 3.1 vs. 50.7 ± 3.3, respectively, all p < 0.05). At 1 year after thyroid surgery, the TC group reported the lowest FIS score.

Longitudinal changes of Reproductive Concerns After Cancer (RCAC) and Fertility Intention Scale (FIS) scores.
Subgroup analyses of reproductive concern and fertility intention according to pregnancy plan within 2 years after surgery are shown in Supplementary Fig. S1 in Supplementary Data. Among women who planned to become pregnant or were undecided, RCAC scores persisted significantly higher in the TC group than those in the benign thyroid disease group from 1 to 18 months after thyroid surgery (all p < 0.05). For fertility intention, the TC group had lower FIS scores at 6 months and 1 year after surgery than the benign thyroid disease (all p < 0.05). There were no significant differences in FIS scores between the two groups at other time points. Among women who did not plan for pregnancy within 2 years after thyroid surgery, RCAC scores were significantly higher in the TC group than those in the benign thyroid disease group at 1 year after surgery (p < 0.001). No significant differences were found in between the two groups at other time points. In terms of fertility intention, the TC group had lower FIS scores at 6 months and 1 year postoperatively than the benign thyroid disease group (all p < 0.05). No significant differences were found in FIS scores at other time points.
Subgroup analyses of RCAC and FIS scores according to the history of childbirth before thyroid surgery are shown in Supplementary Fig. S2 in Supplementary Data. Among women who had one child before surgery, RCAC scores were significantly higher in the TC group than those in the benign disease group at 6 months and 1 year after surgery (all p < 0.001). FIS scores were significantly lower in the TC group than those in the benign lesion group at 6 months and 1 year after surgery (all p < 0.01). No significant differences were found in RCAC scores and FIS scores at other time points. Among women who had no children before surgery, the TC group reported higher RCAC scores from 6 months to 18 months after surgery than the benign disease group (all p < 0.05), while FIS scores were significantly lower in the TC group from 3 months to 1 year after thyroid surgery (all p < 0.05).
Comparison of RCAC and FIS scores between TT and TL groups among TC
RCAC scores and FIS scores of women with TC in the TT group and TL group are shown in Figure 2c, d. The TT group had significantly higher RCAC scores than TL group at time points from 1 month to 2 years postoperatively (58.8 ± 7.5 vs. 55.3 ± 9.3, 62.9 ± 7.9 vs. 58.3 ± 4.8, 66.6 ± 6.0 vs. 64.8 ± 4.8, 71.3 ± 5.8 vs. 63.5 ± 4.6, 54.9 ± 4.2 vs. 51.1 ± 4.1, and 54.8 ± 4.3 vs. 51.7 ± 4.4, respectively, all p ≤ 0.001). RCAC scores of TT group reached the peak at 1 year postoperatively. The TT group had significantly lower postoperative FIS scores than the TL group from 1 to 18 months after surgery (47.6 ± 3.8 vs. 49.5 ± 3.5, 44.2 ± 3.1 vs. 48.6 ± 3.2, 40.1 ± 3.3 vs. 46.7 ± 3.9, 36.6 ± 3.7 vs. 43.5 ± 3.7, and 49.9 ± 3.8 vs. 52.7 ± 4.8, respectively, all p ≤ 0.01). At 1 year following thyroid surgery, both groups had the lowest FIS scores. Changes in levothyroxine dosage and TSH levels during the follow-up period in the two groups are shown in Supplementary Table S3 in Supplementary Data. Supplementary Table S4 in Supplementary Data shows the response to therapy 1 year after initial therapy.
Subgroup analyses of RCAC and FIS between TT and TL groups among women with TC according to pregnancy plan within 2 years after thyroid surgery are shown in Supplementary Fig. S3 in Supplementary Data. Regardless of the presence of a pregnancy plan, RCAC scores remained significantly higher in the TT group than those in the TL group from 1 month to 2 years after surgery (all p < 0.05). Among women with TC who had a pregnancy plan or were undecided about the intention for pregnancy within 2 years after thyroid surgery, the TT group reported lower FIS scores than the TL group from 3 months to 18 months after surgery (all p < 0.05). Among those without a pregnancy plan within 2 years after thyroid surgery, the TT group showed lower FIS scores than the TL group from 1 month to 18 months after thyroid surgery (all p < 0.05).
Subgroup analyses of RCAC and FIS scores between TT and TL groups among women with TC by the history of childbirth before thyroid surgery are shown in Supplementary Fig. S4 in Supplementary Data. Among women with TC who had one child before surgery, RCAC scores were higher in the TT group than those in the TL group from 3 months to 2 year after thyroid surgery (all p < 0.05). For those who had no children before surgery, TT group reported higher RCAC scores than the TL group from 1 month to 2 years after surgery (all p < 0.05). FIS scores were significantly lower in the TT group than those in the TL group from 1 month to 18 months postoperatively for women with one child before surgery (all p < 0.05). For women without children before thyroid surgery, FIS scores were significantly lower in the TT group than those in the TL group from 1 month to 18 months after surgery (all p < 0.05).
Evaluation of pregnancy outcomes
During the 2-year follow-up period after thyroid surgery, 78 women became pregnant. RCAC scores and FIS scores of pregnant women and non-pregnant women are shown in Supplementary Fig. S5 in Supplementary Data. Pregnant women had significantly lower postoperative RCAC scores and higher FIS scores than non-pregnant women from 1 to 12 months after surgery (all p < 0.001). In total, 13 out of 78 pregnant women had pregnancy loss (8 suffered spontaneous abortion and 5 medically induced abortion). The characteristics of pregnancies are listed in Supplementary Table S5 in Supplementary Data. Table 2 shows the comparison of characteristics between pregnant women with pregnancy loss and those having live births. Compared with women who had a live birth, women who suffered pregnancy loss had lower rates of planned pregnancy (53.8% vs. 81.5%, p = 0.021) and preconception counseling (7.7% vs. 36.9%, p = 0.039), and conceived earlier postoperatively (median time to conception after surgery: 6 months vs. 13 months, p = 0.006).
Comparison of Characteristics Between Pregnant Women with Pregnancy Loss and Those Who Had Live Births
TSH, thyrotropin.
We performed further comparisons of pregnancy outcomes across different exposure factors. The proportion of pregnancy loss in women who conceived within 6 months postoperatively was 53.8%, which was significantly higher than those conceived after 6 months postoperatively (Fig. 3; p < 0.001). No significant differences in postoperative pregnancy outcomes were found between the TC group and benign group, nor between the TT group and TL group of women with TC (Supplementary Tables S7 and S8 in Supplementary Data). Women who planned pregnancy had a lower rate of pregnancy loss than those with unplanned pregnancy (11.7% vs. 33.3%, p = 0.021) (Table 3). Women with preconception counseling had a significantly lower rate of pregnancy loss than those without preconception counseling (4.0% vs. 22.6%, p = 0.039) (Table 4).

Frequency of pregnancy loss in women who conceived at different time periods after thyroid surgery.
Adverse Pregnancy Outcomes in Pregnant Women Who Planned Pregnancy and Unplanned Pregnancy
Adverse Pregnancy Outcomes in Pregnant Women With and Without Preconception Counseling
Discussion
This was the first study to focus on reproductive concerns and fertility intention after thyroid surgery in women of childbearing age with TC. The results of this study showed that significantly higher reproductive concern persisted in women with TC compared to those with benign thyroid disease for 2 years after thyroid surgery, and young women with TC who underwent TT exhibited higher reproductive concern than those who underwent TL. There were no significant differences in adverse pregnancy outcomes between women with TC and those with benign thyroid disease, nor between women with TC in the TT group and TL group. We found that women who underwent thyroid surgery were more likely to suffer pregnancy loss if they became pregnant within 6 months postoperatively, and that planned pregnancy and preconception counseling was associated with a reduced risk of pregnancy loss.
Our study indicated that reproductive concern was consistently elevated in childbearing-age women with TC or benign thyroid disease for 6 months after surgery. Reproductive concern was higher in women with DTC who underwent TT. This may be related to the short-term complications that occurred after thyroid surgery. Previous studies have shown that complications such as transient hypoparathyroidism and recurrent laryngeal nerve palsy usually resolve within 6 months after thyroid surgery. 25 Our preliminary study also found a short-term reduction in quality of life after thyroid surgery in patients with DTC, and a higher prevalence of temporary hypoparathyroidism and recurrent laryngeal nerve injury in the TT group. 26 Other studies showed that postoperative levothyroxine dosage was positively correlated with anxiety and depression scores in patients with DTC. 27 In our study, the postoperative levothyroxine dose was significantly higher in women with DTC who underwent TT than those who underwent TL. In addition, we found that the RCAC scores of women with TC continued to rise from 6 months until the peak at 1 year postoperatively, and then gradually declined. This may be related to reassessment of recurrence risk at 1 year postoperatively. In China, for patients with DTC with an initial low-to-intermediate risk of recurrence, dynamic risk reassessment is recommended 1 year postoperatively. 28 Most women were assessed as having a low risk of recurrence at 1 year postoperatively, which may reduce their concern about the disease. Thus, 1 year after thyroid surgery may be a turning point regarding reproductive concerns for young women with TC. Furthermore, the FIS scores of women with TC continued to decrease within 1 year postoperatively. The overall low number of pregnancies in this study may be due to the low intention for fertility after thyroidectomy.
A recent meta-analysis showed that a history of TC and treatment did not increase the risk of adverse pregnancy outcomes. 29 In our study, there were also no significant differences in adverse postoperative pregnancy outcomes between TC group and benign group. Therefore, given that a history of TC did not further increase the risk of adverse pregnancy outcomes, women with a history of TC can be reassured about fertility. For young women with TC who reported high reproductive concerns during treatment and follow-up, physicians should provide information to address any potential reproductive concerns.
In this study, 16.7% of women suffered pregnancy loss during the 2-year follow-up postoperatively. Our previous work based on the Chinese National Free Prepregnancy Checkups Project showed that the rate of pregnancy loss was 2.3% in the general pregnancies. 30 There are no guidelines or studies on the timing of postoperative pregnancy in women undergoing thyroid surgery. Current guidelines only address the timing of pregnancy in women treated with radioactive iodine therapy, which recommend delaying pregnancy for 6–12 months. 4,14,31 This conservative recommendation to delay pregnancy was based on various factors, including the half-life of radioactive iodine, and the time needed for thyroid function to reach homeostasis after radioactive iodine therapy. 32 Anesthesia and surgery have been shown to influence thyroid function. 33,34 Although levothyroxine supplement after thyroid surgery treats hypothyroidism, homeostasis of thyroid hormone levels may not be achieved for some months. Our study showed that women who underwent thyroid surgery were more likely to have a pregnancy loss if they became pregnant within 6 months postoperatively. Early pregnancy after thyroid surgery might result in pregnancy loss due to unstable thyroid hormone levels, which may affect fetal development. However, as there were few pregnancies in our study occurring within 6 months after thyroid surgery, future studies are needed for further verification.
Women who received guidance and consultation before pregnancy had better pregnancy outcomes. 35 Similarly, we found that preconception counseling and planned pregnancy could reduce the risk of pregnancy loss after thyroid surgery. This may be partly owing to preconception counseling and preparation resulting in better control of TSH levels. Maternal peripheral thyroid hormone requirements increase during pregnancy. 36 Subclinical or even overt hypothyroidism are more often encountered in pregnancies following thyroid surgery. For this reason, it was possible that the dosage of levothyroxine during pregnancy in women after thyroid surgery may need to be increased to maintain TSH in the target range. Thus, preconception counseling, planned pregnancy, and evaluation of thyroid function are necessary for young women with a history of thyroid surgery. However, the preconception counseling rate of pregnant women in this study was only 32.1%. As most of the young women in our study were not aware of the importance of preconception counseling, both physicians and patients would benefit from education in this regard.
The present study has several limitations. First, the factors influencing reproductive concern and fertility intention were not collected simultaneously at the postoperative follow-up visits, making it difficult to analyze the real-time factors that led to changes in reproductive concern and fertility intention. Secondly, the small number of pregnancies after thyroid surgery may affect the analysis of adverse pregnancy outcomes. A continued follow-up of the women included in this study is needed to collect more cases of pregnancy for further investigation. Finally, as this was a single-center study conducted in China, a future international multicenter study could expand its external validity.
Conclusion
This study indicates that it is important to address reproductive concerns and fertility intention postoperatively in young women with TC. Preconception counseling and planned pregnancy may be associated with a reduced risk of pregnancy loss after thyroid surgery.
Footnotes
Acknowledgments
The authors thank the participants who took part in this study. Xiaofeng Huang and Xiaofeng Chen from Clinical Trial Unit, the First Affiliated Hospital of Sun Yat-sen University, helped with the collection of questionnaires. Compensation was provided for their assistance.
Authors’ Contributions
Y.L., W.L., and H.G.: Supervised the study. Y.L., F.L., W.L., and R.B.: Conceived and designed the study. F.L. and Y.L.: Had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. F.L., Wanna C., J.Z., Wenxin C., Wenke C., Y.Z., Y.H., Y.H., X.L., Y.Y., T.X., Y.H., X.C., and B.L.: Were responsible for data collection. S.P., J.L., B.L., and H.G.: Contributed to administrative, technical, and material support. F.L., Wanna C., J.Z., Wenxin C., Wenke C., and Y.Z.: Did the statistical analysis and wrote the drafted report. Y.L., W.L., H.G., and R.B.: Critically revised the article. All authors approved the final version before submission.
Author Disclosure Statement
The authors declare no competing financial interests. H.G. is an Associate Editor at Thyroid but she had no role in peer review of this article and was blinded to the peer review process.
Funding Information
This work was supported by the Noncommunicable Chronic Diseases-National Science and Technology Major Project (2024ZD0525600), National Natural Science Foundation of China (82372047 and 82103035), Guangzhou Science and Technology Project (2022342), Kelin Talent Program (R07018), and the China Postdoctoral Science Foundation (2022M723614).
Supplementary Material
Supplementary Data
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.