
Abstract
Background:
We investigated if thyroid nodule taller-than-wide (TTW) feature and sphericity metrics are helpful in separating benign neoplastic thyroid nodules (follicular and oncocytic adenomas) from follicular thyroid carcinomas (FTC) and oncocytic thyroid carcinomas (OCA).
Methods:
This is a retrospective study of TTW sonographic feature as reported by radiologists and nodule sphericity metrics at two academic health systems. Surgical pathology reports for benign and malignant follicular and oncocytic neoplasms, non-neoplastic nodules (hyperplastic and adenomatoid), and classic papillary thyroid cancers (PTC) were extracted from enterprise data warehouses. We independently reviewed each ultrasound and recorded nodule dimensions to identify nodules that were TTW and determine if the proportion of TTW nodules is different in benign and malignant thyroid nodules of various histologies. We also evaluated the sphericity index and sphericity ratio, two quantitative measures of how close the 3D shape of the nodule is to a sphere.
Results:
In total, 1110 nodules were analyzed: 209 non-neoplastic nodules (hyperplastic and adenomatoid), 398 benign neoplasms (follicular and oncocytic adenomas), and 503 malignant neoplasms (FTC, OCA, PTC, and follicular variant-PTC [FV-PTC]) and noninvasive follicular thyroid neoplasm with papillary-like features (NIFTP). There was no statistical difference for the TTW feature when follicular and oncocytic adenomas were compared with FV-PTC, OCA, FTC, and NIFTP (χ2, p = 0.08, sensitivity of 28% [confidence interval 23–24%]), when follicular adenoma was compared with FTC (χ2, p = 0.64) or when oncocytic adenoma was compared with OCA (χ2, p = 0.08). Benign and malignant neoplasms were more likely than non-neoplastic nodules to be TTW (χ2, p = 0.02). In contrast, the sphericity index and sphericity ratio were significantly different in most comparisons of benign and malignant nodules (Wilcoxon, p < 0.03) except for oncocytic tumors.
Conclusions:
TTW shape has limited utility in distinguishing benign follicular and oncocytic neoplasms from malignancy. This sonographic feature was more common among all benign and malignant neoplasms when they were compared as a group to non-neoplastic nodules, which suggests this sonographic feature is an indicator of neoplastic growth (benign or malignant) but not cancer. Alternative methods, such as measures of sphericity, are needed to distinguish benign and malignant oncocytic and follicular neoplasms.
Background
Follicular thyroid carcinomas (FTC) and oncocytic thyroid carcinomas (OCA) account for 10–15% and 3–5% of all thyroid cancers, respectively, and are generally considered to be more aggressive, more likely to metastasize, and more likely to be resistant to radioactive iodine therapy than papillary thyroid cancer (PTC). 1 –3 Unfortunately, these cancers are also difficult to diagnose on ultrasound as they frequently do not manifest suspicious sonographic features such as punctate echogenic foci, irregular borders, or hypoechogenicity (Fig. 1). 4 –9 To capture these cancers, the current guidelines from the American Thyroid Association (ATA) 10 and American College of Radiology Thyroid Imaging Reporting and Data System (ACR TI-RADS) 11 recommend a biopsy of thyroid nodules above a certain size threshold, even if they appear benign on ultrasound (ATA low suspicion sonographic pattern and ACR TI-RADS TR3 nodules, respectively). Many of these thyroid biopsies produce benign or indeterminate cytological results. 12
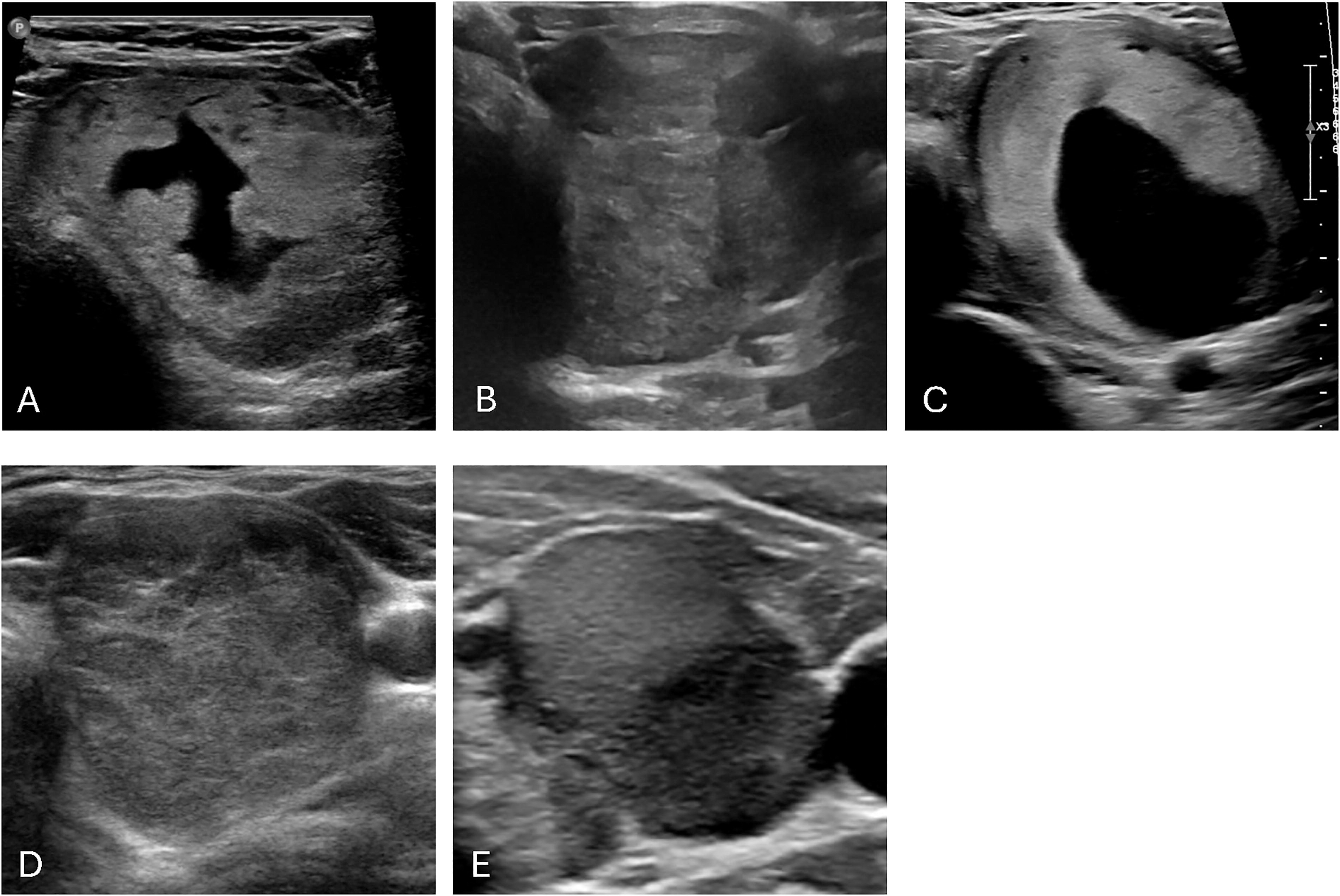
Ultrasound images of taller-than-wide thyroid nodules. Images illustrate how follicular and oncocytic neoplasms are difficult to diagnose based on ultrasound appearance. These nodules are all taller-than-wide. A. Follicular variant of papillary thyroid cancer. B. Oncocytic carcinoma. C. Follicular thyroid carcinoma. D. Follicular Adenoma. E. Oncocytic adenoma.
An important component of the 2015 ATA 10 and ACR TI-RADS 11 risk stratification algorithms is the taller-than-wide (TTW) feature, which is defined as a nodule that has an anteroposterior dimension greater than a transverse dimension. This is a sonographic feature that was first shown to be a predictor for malignancy by Kim et al. in 2002. 13 Previous studies showed that TTW shape has a high specificity and high positive predictive value for malignancy. However, these pivotal studies have either only focused on PTC or have included a few cases of follicular or oncocytic cancers in their analysis. 13 –18 Table 1 summarizes studies that evaluated TTW feature in follicular and/or oncocytic cancers. A large study of over 800 nodules found that there was a statistically significant difference for TTW feature among neoplastic follicular-patterned lesions (follicular adenoma [FA], FTC, follicular variant of PTC [FV-PTC], and noninvasive follicular thyroid neoplasm with papillary-like nuclear features [NIFTP]) compared with hyperplastic nodules. 19 However, a subgroup analysis from a large multicenter study in 2021 did not show a statistically significant difference in TTW shape among adenomatous nodules/adenomatous goiter (n = 606), FA (n = 288), or FTC (n = 101). 20 Two smaller studies evaluating sonographic features of FTC and OCA did not find TTW feature as significantly associated with malignancy. 21,22 Other proposed methods to improve ultrasound-based risk stratification of thyroid nodules include establishing a TTW cutoff ratio ≥1.2 25 and evaluating for overall spherical shape. 26 While the latter was shown to be an independent predictor of malignant risk, these studies focused mostly on PTC and did not include many follicular or oncocytic cancers.
Research Studies Evaluating TTW Feature in Follicular and Oncocytic Cancers
FA, follicular adenoma; FTC, follicular thyroid carcinoma; FV-PTC, follicular variant of papillary thyroid cancer; NIFTP, non-invasive follicular neoplasm with papillary-like nuclear features; OA, oncocytic adenoma; OCA, oncocytic thyroid carcinoma; PTC, papillary thyroid cancer; TTW, taller-than-wide.
We hypothesized that the TTW feature is characteristic of neoplastic growth (benign or malignant), and it is not specific to cancer. To test this hypothesis, we analyzed data for 1110 nodules collected from two large academic health care systems enriched for difficult-to-diagnose FTC, OCA, FV-PTC, and NIFTP and corresponding benign neoplasms such as FA and oncocytic adenomas (OA). We also explored whether sphericity metrics could be an alternative method to separate benign neoplastic nodules (follicular and oncocytic adenomas) from malignant nodules (follicular and oncocytic carcinomas).
Methods
Study design and population
This retrospective study was conducted using data acquired as part of routine clinical care for thyroid nodules at two large health care systems, UC Health and UW Medicine, affiliated with the University of Colorado (Aurora, CO) and the University of Washington (Seattle, WA), respectively.
The inclusion criteria were the availability of thyroid ultrasound images and histopathologic diagnosis for the thyroid nodule. We excluded thyroid nodules where ultrasound imaging and histopathologic diagnosis could not be unambiguously matched. All ultrasound studies measured and reported nodule dimensions in three planes. Most thyroid ultrasounds were performed at the radiology facilities from the UC Health or UW Medicine health care systems using the following ultrasound systems: GE LOGIQ E9 and E10, Siemens ACUSON S2000 and Sequoia, and Philips iU22 and EPIQ 7G. We did not restrict ultrasound studies based on the protocols used by radiologists. Most radiology reports used ACR TI-RADS 11 or ATA nodule sonographic risk patterns. 10
Thyroid surgical pathology reports (n = 7467) were extracted from enterprise data warehouses at two universities to identify benign neoplasms (FA and OA) and malignant neoplasms (FTC, OCA, FV-PTC, and NIFTP). A similar number of non-neoplastic nodules (hyperplastic and adenomatoid) and classic PTC were also randomly selected for comparison (Table 2). We reviewed images from each ultrasound study and recorded nodule dimensions as labeled by a clinical radiological or ultrasound technician. We did not re-measure the nodules to minimize bias in our study and because we were interested in TTW feature performance as it is used by clinicians in practice. The investigators were not blinded to the outcomes of the study.
Counts of All and TTW Nodules Stratified by Histological Diagnosis
AN, adenomatoid nodule; HN, hyperplastic nodule.
TTW feature was defined as an anteroposterior dimension that is greater than a transverse dimension of a nodule. We also tested an anteroposterior dimension to transverse dimension ratio of 1.2 (TTW-1.2) as proposed by Grani et al. 25
Sphericity index was calculated as
Statistical analysis
Statistical analyses were performed in R version 4.2. Pearson’s chi-squared and Wilcoxon tests were used to compare groups. The R packages caret and epiR were used to calculate confusion matrix statistics. Exact binomial confidence intervals (CIs) were calculated for sensitivity, specificity, and positive and negative predictive values. R package pROC was used to estimate the area under the receiver operating characteristic curve, and CI was computed with the help of the DeLong test. Sphericity metrics optimal cutoffs for a binary benign versus malignant thyroid nodule classification were calculated to minimize Youden J-index (sensitivity + specificity − 1). A p-value of 0.05 or less was considered statistically significant. Reproducible computer code and the source data are available at https://github.com/pozdeyevlab/ttw.
Results
A convenience series of 1110 nodules was studied (Table 2). Based on surgical histopathology reports, this series included 209 benign non-neoplastic nodules (91 hyperplastic and 118 adenomatoid nodules), 398 benign neoplasms (282 FA and 116 OA), and 503 thyroid cancers and NIFTP (200 PTC, 54 FTC, 175 FV-PTC, 34 OCA, and 40 NIFTP). NIFTP was included in the malignant group since it is treated with surgery. 29
Classic PTC was more likely to be TTW than non-neoplastic benign nodules (Table 3, χ2, p = 0.01), which is consistent with published data 13 –18 ; 28.5% of PTC were TTW compared with 17.7% of adenomatoid and hyperplastic nodules. The TTW shape, when used to predict PTC, had high specificity and high positive predictive value (82% and 61%, respectively) but a low sensitivity of 28% (Table 4). When all malignant nodules were compared with all benign ones, TTW was significantly more prevalent in thyroid cancers and the NIFTP group (Table 3, χ2, p = 0.004), supporting TTW feature use in clinical risk stratification schemas.
TTW Feature and Sphericity Metrics of Thyroid Nodules of Various Histological Subtypes
AUROC, area under receiver operating characteristic curve; CI, confidence interval; IQR, interquartile range; TTW-1.2, modified TTW feature defined as anteroposterior/transverse dimension ratio of 1.2.
TTW Feature and Sphericity Metrics as Predictors of Malignancy
Confidence interval is shown in square brackets; optimal cutoff for sphericity metric was selected to maximize sensitivity and specificity.
NPV, negative predictive value; PPV, positive predictive value.
Less than one-third of follicular and oncocytic cancers and NIFTP were TTW (Table 2). There was no statistical difference for TTW feature (χ2, p = 0.08) when combined FV-PTC, OCA, FTC, and NIFTP were compared with FA and OA. The accuracy of TTW feature as a predictor for malignancy was 57% and was not different from the no information rate (56.8%, when all nodules are assigned to a majority benign class not using TTW as a predictor). TTW feature had a lower specificity and positive predictive value: 78% and 49%, respectively (Table 4).
We also compared follicular and oncocytic adenomas with FTC and OCA, cancers that frequently do not manifest other suspicious features on ultrasound 4 –9 and cannot be diagnosed based on fine-needle aspiration (FNA) results alone. The proportion of TTW nodules was not different in benign and malignant nodules (Table 3, χ2, p = 0.40). In addition, FTC was no more likely to be TTW than follicular adenoma (χ2, p = 0.64), and OCA was no more likely to be TTW than oncocytic adenoma (χ2, p = 0.08).
Overall, benign and malignant neoplasms (FA, OA, PTC, FTC, FV-PTC, OCA, and NIFTP) as a group were more likely to be TTW than benign non-neoplastic nodules (χ2, p = 0.02).
An alternative anteroposterior/transverse dimension ratio of 1.2 (TTW-1.2) was proposed as more specific for malignancy. 25 In our analysis, TTW-1.2 feature had lower sensitivity, and it was not significantly different in benign and malignant nodules (Table 3). TTW-1.2 was not designed to be used alone and may perform better when combined with other sonographic risk features.
TTW feature uses two dimensions of the three-dimensional nodule shape. We tested a sphericity index, a quantitative measure of how close the shape of the nodule is to a sphere, leveraging all three dimensions of the nodule. The sphericity index was significantly higher in malignant nodules in all comparisons (Table 3, Wilcoxon, p < 0.03) except for oncocytic tumors. While highly significant, the absolute difference in median sphericity index between benign and malignant nodules was small (Table 3, 0.01–0.05).
We also tested the sphericity ratio metric proposed by Pappa et al., 26 which is defined as a ratio of the longest to shortest nodule dimension. The sphericity index and ratio were strongly correlated (Spearman correlation [ρ] −0.93, p < 2.2e-16). The sphericity ratio was significantly lower in cancers (indicating a more spheric shape) in all comparisons of benign and malignant thyroid nodules except for oncocytic tumors (Table 3, Wilcoxon, p < 0.03). The difference in sphericity ratio did not reach a significance threshold when neoplastic nodules (including benign adenomas) were compared with non-neoplastic nodules (p = 0.1). Notably, most differences in sphericity index and sphericity ratio remain significant when conservative Bonferroni correction is used to adjust for multiple hypotheses testing (Table 3, significance threshold of 0.002).
Confusion matrices for sphericity metrics were computed using thresholds that maximize sensitivity and specificity (Table 4). Overall, sphericity measures had higher sensitivity for detecting cancer than the TTW feature. There was a nonsignificant (as indicated by overlapping CIs) trend toward higher accuracy for sphericity measures when compared with TTW feature.
Discussion
Thyroid nodules that are TTW are considered at higher risk for malignancy per current thyroid nodule guidelines 10,11 and are more likely to be biopsied than nodules that do not possess these features. The widely used ACR TI-RADS thyroid nodule risk stratification algorithm 11 assigns 3 points to the TTW feature, which, in the absence of any other scoring features, leads to a recommendation to biopsy for nodules that are more than 2.5 cm in size. 11
This recommendation is based on several studies demonstrating high TTW feature specificity and positive predictive value for malignancy. However, these studies have focused on PTC, 6,8,13,16 –18,20 which usually has other suspicious features on ultrasound, such as hypoechogenicity, irregular borders, and/or punctate echogenic foci, and frequently are not challenging to detect on imaging. Only a few studies looked at the TTW shape for follicular and oncocytic cancers, which typically lack the suspicious sonographic features seen in PTC. These studies summarized in Table 1 do not support TTW shape as a useful feature that can separate malignant (FTC and OCA) and benign neoplasms. 20 –22 This limitation is significant because benign and malignant follicular and oncocytic neoplasms frequently produce indeterminate cytology on fine needle aspiration biopsy and cannot be distinguished cytologically.
In this retrospective study, we focused on benign and malignant follicular and oncocytic neoplasms. We demonstrated a statistically significant difference in TTW feature when benign and malignant follicular and oncocytic neoplasms as a group were compared with adenomatoid and hyperplastic nodules, but importantly there was no difference in the frequency of TTW shape when follicular and oncocytic adenomas were compared with follicular and oncocytic malignancies (FTC, OCA, FV-PTC, and NIFTP) (Table 3). Thus, while TTW feature is useful when separating PTC from hyperplastic and adenomatoid nodules, the TTW feature has limitations when used to distinguish FTC and OCA from FA and OA.
Distinguishing between benign and malignant follicular and oncocytic neoplasms remains an unsolved challenge in the diagnostic evaluation of thyroid nodules. Figure 1 shows examples of TTW nodules and illustrates the diagnostic challenge of distinguishing benign and malignant follicular and oncocytic neoplasms. To our knowledge, no single sonographic feature has been shown to differentiate these benign and malignant neoplasms except when clear signs of invasive growth or metastatic lymph nodes are present on ultrasound. Of particular importance is that follicular and oncocytic adenomas are clonal neoplasms, frequently identified to have oncogenic genetic alterations such as mutations in RAS genes, PPARG or IGF2BP3 gene fusions, and chromosomal copy number alterations, and require thyroid surgery for definitive diagnosis. 23,24,30 Our study demonstrated that TTW feature does not help to solve this diagnostic challenge.
Using sphericity index and previously proposed sphericity ratio, 26 we demonstrated that malignant thyroid nodules (including challenging-to-classify FTC and OCA) are less ellipsoid and are more spherical than benign tumors and non-neoplastic thyroid nodules. Roundness and sphericity were previously proposed as useful metrics to stratify thyroid nodules. 26,31 Our data corroborate and extend these studies, showing that sphericity is useful in challenging scenarios such as separating FTC from FA. Additional work is needed to establish optimal sphericity index and sphericity ratio thresholds. Using all three dimensions (or automated nodule segmentation of both transverse and longitudinal images) when training machine learning or artificial intelligence-based thyroid nodule classifier may be beneficial.
Our study has limitations. This was a retrospective study that relied on histopathologic diagnosis and, therefore, only included patients who had thyroid surgery. The prevalence of OCA in our study was low (2.7%), which is consistent with published estimates. 1 FV-PTC comprises most cancers in our study. However, even when FV-PTC was excluded from the subgroup analysis, there was no statistical difference in the frequency of TTW shape, when follicular and oncocytic adenomas were compared with FTC and OCA. Furthermore, we used the thyroid nodule dimensions as reported by the radiologist. This approach was chosen to evaluate the TTW feature as it is used in routine clinical practice. We acknowledge that the TTW feature may perform differently when highly trained radiologists use it in research studies. The interobserver variability when measuring thyroid nodules on ultrasound images is significant. 32,33
In summary, our study demonstrates that the TTW feature is not useful in distinguishing non-PTC thyroid malignancies from their benign neoplastic counterparts. The data support the hypothesis that TTW is a characteristic of neoplastic clonal growth and is not specific to cancer. Additional methods of distinguishing benign and malignant thyroid neoplasms are needed, including machine learning analysis of ultrasound images (which may identify features not obvious to the human reader) or sophisticated tests that recognize molecular signatures of invasive and metastatic growth. Reducing the weight of the TTW feature or replacing the TTW feature with sphericity metric in future ultrasound-based risk stratification algorithms may be beneficial.
Footnotes
Authors’ Contributions
C.B.: Conceptualization (equal), investigation, writing—original draft (lead), visualization (lead), project administration (equal), and funding acquisition (equal). S.L.W.: Software (equal), validation (equal), formal analysis (lead), and data curation (equal). T.T.: Conceptualization (support) and writing—review and editing (support). M.D.: Conceptualization (support) and writing—review and editing (equal). A.L.G.: Conceptualization (support) and writing—review and editing (equal). W.G.: Conceptualization (support) and writing—review and editing (equal). S.M.: Conceptualization (support) and writing—review and editing (equal). B.R.H.: Supervision (equal), conceptualization (support), and writing—review and editing (support). N.P.: Conceptualization (equal), methodology (lead), software (equal), validation (lead), formal analysis (equal), investigation (lead), resources (lead), writing—original draft (equal), supervision (equal), and funding acquisition (equal).
Author Disclosure Statement
C.B. is a principal investigator for a study supported by Veracyte, Inc. T.T. is on a data monitoring committee for a clinical trial sponsored by Abbvie. M.D. receives funding from Philips Medical Imaging and Elsevier for her role as editor of the World Federation for Ultrasound in Medicine and Biology Ultrasound Open. W.G. was a member of the National Comprehensive Cancer Network Thyroid Cancer Guidelines and is currently a member of the American Thyroid Association Thyroid Cancer Guidelines workgroup. S.M. is a member of the American Thyroid Association Thyroid Nodule Guidelines workgroup. N.P. and B.R.H. receive research support from Veracyte, Inc., unrelated to this study. S.L.W. and A.L.G. have no disclosures.
Funding Information
C.B. received funding support from Endocrine Fellows Foundation. N.P. received funding from the National Institutes of Health (NCI R21 1R21CA282380). S.L.W., T.T., M.D., A.L.G., W.G., S.M., and B.R.H. have no funding to disclose.