
Abstract
Background:
Active surveillance (AS) has emerged as an established management strategy for patients with low-risk papillary thyroid microcarcinoma (PTMC). However, prior studies have suggested accelerated tumor growth during pregnancy, which raises concerns about the suitability of AS for reproductive-age patients. This study evaluates the longitudinal impact of pregnancy on tumor dynamics and validates the safety of AS management in this population.
Methods:
From February 2020 to October 2024, a single-institution prospective AS cohort enrolled 260 female patients diagnosed with low-risk PTMC. Eighteen female patients (21 pregnancy events) with complete series of ultrasound documentation underwent longitudinal analysis of changes in tumor size and growth velocity, with time-stratified comparisons before pregnancy, during pregnancy, and after delivery. Tumor doubling rate (TDR) was calculated to quantify tumor growth or shrinkage patterns across these periods. An increase in tumor size of 3 mm or more was defined as substantial enlargement.
Results:
Over a median follow-up of 59.0 (interquartile range 38.5, 72.0) months, tumor enlargement (>3 mm) was observed in 19.0% (4/21) of the PTMC cases by the last follow-up. During pregnancy, 76.2% (16/21) of tumors exhibited accelerated growth (TDR >0.5/year) or moderate growth (TDR 0.1–0.5/year), whereas postpartum stabilization (TDR −0.1 to 0.1/year) or regression (TDR <−0.1/year) occurred in 71.4% (15/21). The TDR peaked during pregnancy and decreased after delivery (0.39/year vs. −0.01/year, p = 0.006). Delayed surgery was required in only two patients and no instances of expanded surgical scope, T-stage progression, or tumor recurrence were observed.
Conclusion:
While pregnancy may transiently accelerate tumor growth in low-risk PTMC, most gestational changes are self-limited, with stabilization or regression commonly observed postpartum. AS remains a safe and effective strategy for reproductive-age patients, balancing oncologic safety with fertility preservation. Confirmatory studies incorporating extended follow-up and advanced imaging modalities are essential to further validate these findings and optimize clinical frameworks.
Introduction
Over 200,000 women in China are newly diagnosed with thyroid cancer annually, reflecting a significant public health burden in recent years. It is estimated that more than 85% of these cases are attributable to overdiagnosis, according to the International Agency for Research on Cancer. 1,2 Papillary thyroid carcinoma (PTC) is the pathological type responsible for the increasing incidence of thyroid cancer, accounting for approximately 84% of all cases. 3 Enhanced perinatal healthcare and widespread ultrasound screening have led to a higher frequency of overdiagnosis of low-risk papillary thyroid microcarcinomas (PTMCs, i.e., PTC ≤1 cm) in women of reproductive age (18–45 years). From 2012 to 2020, nearly half of all patients with PTC who underwent thyroidectomy at our center were PTMCs in women of reproductive age. 4
Active surveillance (AS) has been considered an alternative to immediate surgery for low-risk PTMC, with only a small number of patients requiring delayed surgery due to tumor progression or new lymph node metastasis. However, during pregnancy, elevated levels of human chorionic gonadotropin (hCG) and estrogen may promote the proliferation of thyroid follicular cells, potentially accelerating tumor growth. 5 Two observational studies of PTC in women during pregnancy from Kuma Hospital and Asan Medical Center reported tumor enlargement (≥3 mm) in 7.8% (4/51) and 15.8% (3/19) of cases, respectively, during short-term gestation follow-up. 6,7 In contrast, long-term AS cohorts from the same institutions demonstrated tumor progression rates of 4.7% (58/1235) over a mean follow-up of 60 months and 14.1% (27/192) over a median follow-up of 30 months. 8,9 These findings suggest that the risk of tumor progression in pregnant patients managed by AS may be greater than that in their nonpregnant counterparts.
The 2015 American Thyroid Association guidelines recommend delaying surgery for pregnant patients newly diagnosed with PTC unless substantial tumor growth (defined as ≥20% increase in two dimensions [+2 mm] or >50% volume increase [Section A24]) occurs before 24 weeks of gestation. For such cases, pregnancy surgery may be considered; surgery may be considered; however, if the tumor stabilizes by mid-gestation, surgery can be postponed until after delivery (Recommendation 31). 10 Critically, current guidelines lack explicit recommendations for managing low-risk PTMC in patients already undergoing long-term AS prior to pregnancy. This omission underscores a key clinical gap, as existing protocols prioritize nongravid populations, leaving clinicians without evidence-based strategies for balancing oncologic safety against maternal-fetal well-being in this unique cohort.
In this study, we reviewed the medical records of all patients with low-risk PTMC who experienced pregnancy in our AS cohort. We selected 21 pregnancy events with complete ultrasound images across three periods: before pregnancy, during pregnancy, and after delivery. Using a controlled before-after approach, we evaluated the natural course of the tumor during pregnancy and determined the impact of pregnancy on tumor progression and long-term outcomes in patients with low-risk PTMC.
Materials and Methods
Patients and study design
A prospective AS cohort (KMU-AS cohort) was established at the First Affiliated Hospital of Kunming Medical University in February 2020. Inclusion criteria comprised patients diagnosed with papillary thyroid microcarcinoma (PTMC) meeting the following parameters: (1) tumor diameter ≤1 cm, (2) Bethesda category V/VI cytology or presence of a BRAF mutation, and (3) absence of extrathyroidal extension, lymph node involvement, or distant metastases. 11 As of October 2024, 260 female patients were enrolled. Among these, 29 patients experienced 33 pregnancies and deliveries, while the other 2 experienced miscarriage (Fig. 1). The criteria for delayed surgery were derived from the Japanese Consensus Statement of AS. 12 A sustained increase in at least two examinations with tumor diameter greater than 3 mm was considered a relative surgical indication, and patient preference was fully considered.
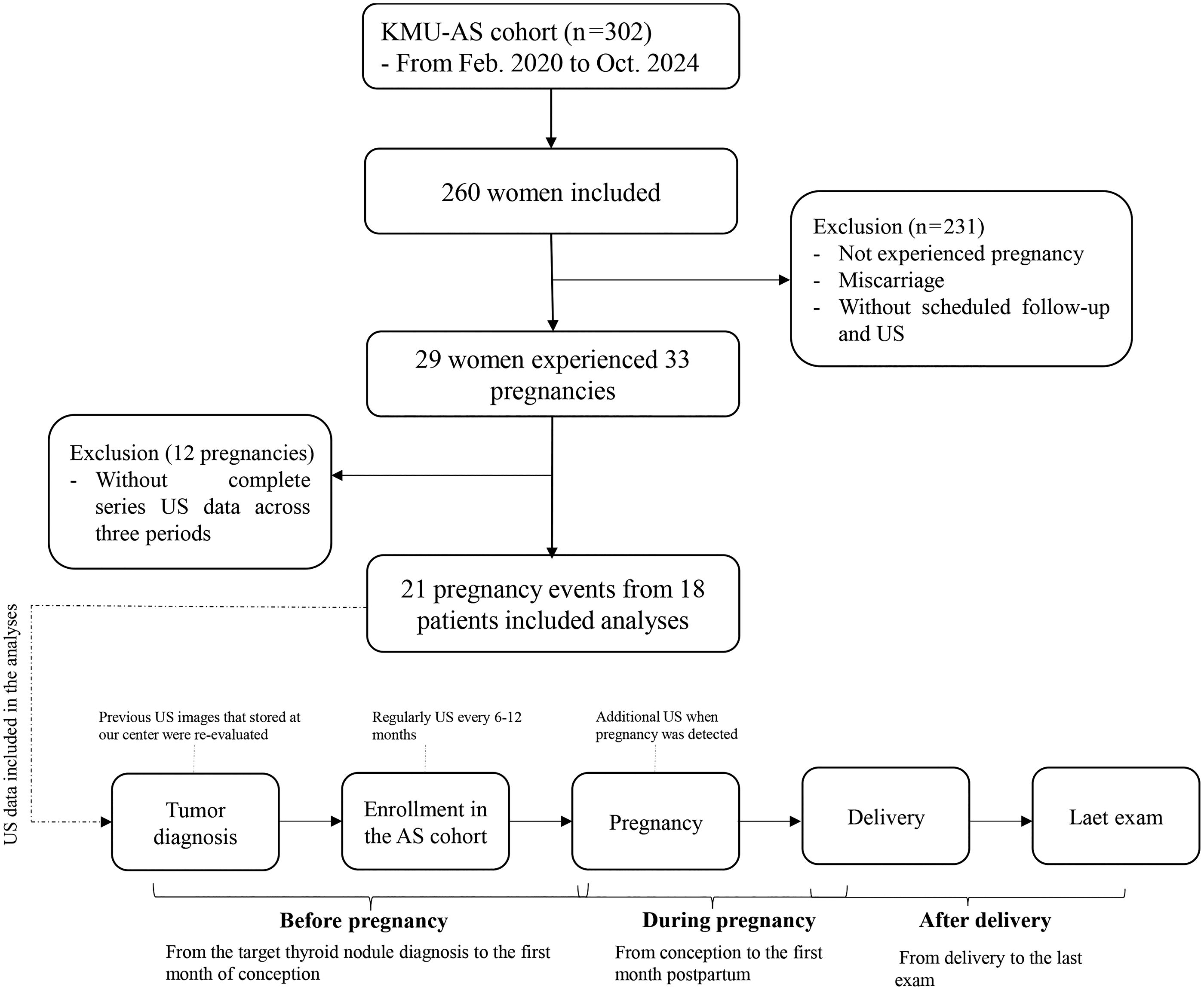
Flowchart of the included patients and ultrasound monitoring strategy. AS, active surveillance; US, ultrasound.
We analyzed ultrasound images across three periods:
Ultimately, 21 pregnancy events from 18 patients with complete AS data across all three periods were included in this controlled before-after study. In accordance with the recommendations of the Chinese guidelines for the diagnosis and management of thyroid disease during pregnancy and postpartum (second edition) and Japanese consensus statements on AS, a thyrotropin (TSH) level ≥2.5 mIU/L was established as the intervention threshold for both pregnancy and postpartum periods to mitigate tumor progression risks. 12,13 Thyroid function (TSH, T3, T4, free-T3, free-T4) was measured during each trimester. Levothyroxine therapy was initiated in three patients during pregnancy, none of whom required delayed surgical intervention. One patient discontinued treatment after the lactation period due to normalized TSH levels, while the other two continued therapy postpartum as part of their ongoing clinical management.
This study was approved by the Ethics Committee of the First Affiliated Hospital of Kunming Medical University (2020 Ethical Review L No. 16). Informed consent was obtained from all participants at the time of enrollment.
Ultrasound evaluation
Patients were regularly followed up with neck ultrasonography (US) every 6–12 months, as previously reported. 11 Upon detection of pregnancy, patients were scheduled for an additional US. All US examinations were performed by the same experienced radiologist (W.C.) using identical equipment (LOGIQ™ E10 Series, GE HealthCare, USA) with a linear high-frequency probe 4–20 MHz to minimize measurement variability. Additionally, some patients with low-risk PTMC underwent follow-up and US surveillance for several years prior to enrollment. Previous images stored at our center were re-evaluated by the same US specialist and were included in the analyses.
Serial US examinations were used to assess tumor size or volume. Maximal tumor size and two- or three-dimensional tumor volume calculation were performed to evaluate changes in size and volume, respectively. The tumor volume was calculated according to the ellipsoid equation π/6 × D1 × D2 × D2 or π/6 × D1 × D2 × D3. The tumor doubling rate (TDR), defined as the reciprocal of tumor multiplication time, was calculated via the “Doubling Time & Progression Calculator” program published by Kuma Hospital (http://www.kuma-h.or.jp/english/). The TDR serves as an index for assessing the tumor growth rate and determining the necessity of surgical interventions. A TDR >0.5/year indicates rapid tumor growth, whereas a TDR of 0.1–0.5/year signifies moderate growth. Conversely, a TDR between −0.1 and 0.1/year denotes tumor stability, while a TDR <−0.1/year indicates tumor shrinkage. 14,15
Statistical analysis
Statistical analyses were performed via IBM SPSS Statistics version 26.0, and graphs were generated by GraphPad Prism 9.5. Continuous variables are presented as medians with interquartile ranges (IQRs) or as means with standard deviations. Categorical variables are expressed as frequencies with corresponding percentages. For comparisons of repeated measurements before pregnancy, during pregnancy, and after delivery, repeated-measures analysis of variance was used for normally distributed data, whereas the Wilcoxon signed rank test was applied for non-normally distributed data. A p-value of <0.05 was considered statistically significant.
Results
Monitoring the outcomes of patients with PTMC during pregnancy
Table 1 shows the baseline characteristics of 21 pregnancy events in patients under AS management. The mean age at PTMC diagnosis was 29.3 years, and the mean age at pregnancy was 31.1 years. With a median AS duration of 59.0 (IQR: 38.5–72.0) months, four patients (19.0%) presented an increase in tumor size of more than 3 mm at the last US examination compared with the initial diagnosis. One patient developed new central lymph node metastasis. Two patients underwent a 3 mm increase in tumor size and refused surgery. Notably, no significant clinical symptoms were observed throughout the study period. When comparing pregnant with nonpregnant female patients in the entire AS cohort, tumor enlargement >3 mm occurred in 20.7% (6/29 patients) of pregnant patients compared with 7.0% (16/229 patients) of nonpregnant patients (p = 0.025).
Baseline Clinical Characteristics and Active Surveillance Outcomes of Pregnant Patients with Low-Risk Papillary Thyroid Microcarcinoma
Cumulative tumor changes across surveillance phases.
AS, active surveillance; IQR, interquartile range; PTMC, papillary thyroid microcarcinoma; SD, standard deviation.
During the three predefined periods (preconception, gestational, and postpartum phases), the mean US frequency was 2.6, 2.3, and 3.2 scans, respectively. All participants underwent ultrasound examinations during both the first and third trimesters, with six patients receiving ultrasound monitoring across all three trimesters. Serial measurements in six patients revealed no statistically significant changes in tumor size between trimesters (first vs. second trimester: p = 0.496; second vs. third trimester: p = 0.108). Notably, no cases demonstrated either a >3 mm increase in maximum tumor diameter or the development of new lymph node metastasis.
Delayed surgery was performed in two cases (9.5%) at 12 and 35 months postdelivery, following total monitoring durations of 54 and 65 months, respectively. In Case 1, the tumor size increased by 4.6 mm during pregnancy but subsequently shrank during extended AS (maximum size: 10.6 mm during pregnancy vs. 9.7 mm at final follow-up). However, central lymph node metastasis was detected via US 12 months postpartum and confirmed by postoperative histopathology. In Case 2, the tumor exhibited persistent growth, increasing from maximum size of 4.0 mm at diagnosis to 4.8 mm during pregnancy, and further enlarging to 8.7 mm by the final follow-up. Notably, neither case required expanded surgical scope, nor was T-stage progression or recurrence observed postoperatively.
The natural course of PTC with pregnancy
The TDR was utilized to assess the growth rates of PTC with or without pregnancy. Compared with the prepregnancy period, 61.9% (13/21) of cases presented accelerated tumor growth during pregnancy. Specifically, 76.2% (16/21) of cases exhibited either rapid tumor growth (TDR >0.5/year) or moderate tumor growth (TDR 0.1 to 0.5/year) during pregnancy. Postdelivery, the tumor growth rate decreased significantly, and 71.4% (15/21) of PTMCs were stable (TDR −0.1 to 0.1/year) or shrank (TDR <−0.1/year). Only 19.0% (4/21) and 9.5% (2/21) of cases continued to exhibit rapid and moderate growth, respectively (Fig. 2).

The tumor growth rate distributions in patients with papillary thyroid carcinoma at different time points. TDR, tumor doubling rate.
Furthermore, continuous serial US monitoring was employed to evaluate the natural growth rates of PTMCs across the three periods: before pregnancy, during pregnancy, and after delivery. The average TDRs were 0.18/year before pregnancy, 0.39/year during pregnancy, and −0.01/year after delivery (P = 0.037), which indicates a statistically significant change. As illustrated in Figure 3, the TDR peaked during pregnancy and subsequently declined after delivery. Paired comparison revealed that this downward trend was statistically significant (prepregnancy vs. during pregnancy p = 0.737, and during pregnancy vs. postpartum p = 0.006).
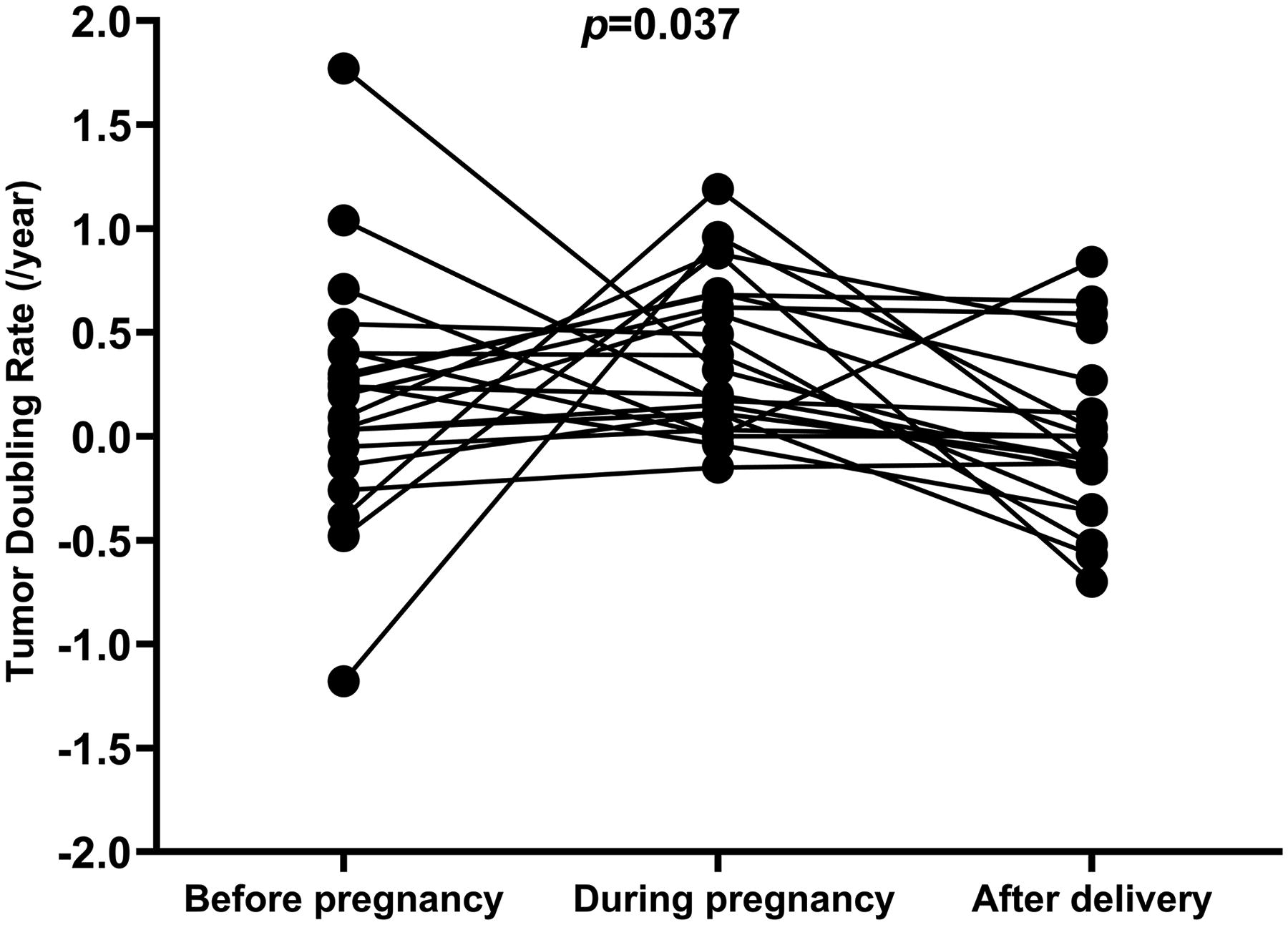
The natural course of tumor doubling rate in the before-after pregnancy cohort.
Discussion
This longitudinal cohort study provides critical insights into the dynamic behavior of low-risk PTMC during pregnancy and postpartum periods. By prospectively analyzing 21 pregnancy events in 18 patients under AS, we observed a transient acceleration in tumor growth velocity during gestation, with 61.9% (13/21) of cases demonstrating increased tumor growth rates compared with prepregnancy baselines. Notably, no tumors exceeded the 3 mm size threshold for clinical concern during this phase. More importantly, 71.4% (15/21) of cases exhibited stabilization or shrinkage postpartum, aligning with the physiological resolution of pregnancy-associated hormonal stimuli. These findings reinforce two key clinical tenets: (1) pregnancy-related tumor kinetic changes in low-risk PTMC are predominantly self-limited and (2) AS remains a safe and feasible strategy for reproductive-age patients with low-risk PTMC.
The Japanese Consensus Statements for AS endorse AS as a viable option for both pregnant patients and those planning pregnancy. 12 This recommendation stems from the low incidence of clinically significant tumor enlargement (≥3 mm) during pregnancy, exemplified by the Kuma Hospital cohort, the birthplace of AS, where only 8% (4/50) of PTMC cases exhibited such growth. Among these, two patients underwent surgery after delivery and had no recurrence, while the remaining two continued AS due to tumor stability postdelivery. 6 Several other studies of AS during pregnancy have also reached the consensus that delaying surgery until the postpartum period does not result in worse outcomes for patients with PTC. 7,16,17 However, current clinical guidelines lack explicit recommendations for managing patients with AS during pregnancy, leaving clinicians without evidence-based strategies to balance oncologic safety with maternal-fetal well-being in this unique cohort. 10,12
Our clinical observations reveal a distinct tumor kinetic pattern in PTMC during pregnancy, characterized by transient growth acceleration followed by postpartum deceleration. TDRs demonstrated phase-specific shifts: rising from a prepregnancy average of 0.18/year to 0.39/year during gestation, then declining sharply to −0.01/year postpartum (p = 0.037). This trajectory underscores the transient nature of gestational growth acceleration. Delayed surgery was ultimately required in only two patients—one due to sustained tumor growth (>3 mm) and another for emerging lymph node metastasis. Critically, no instances of expanded surgical scope, T-stage progression, or recurrence were observed postoperatively. These findings underscore that AS remains a safe strategy even for PTMCs exhibiting transient gestational growth acceleration, as most pregnancy-associated tumor changes are self-limiting or reversible postpartum. Consequently, AS should be prioritized as a viable management approach for this population, balancing oncologic safety with fertility and lactation demands and quality-of-life considerations.
The dynamic growth pattern of PTC during pregnancy appears to mirror the physiological trajectory of pregnancy-associated hormonal fluctuations. The transient acceleration of tumor growth may be attributed to synergistic effects of gestational hormones: hCG sharing structural homology with TSH through its alpha subunit, exerts mitogenic effects on thyrocytes through competitive TSH receptor binding. 18 More significantly, estrogen establishes a pro-tumorigenic milieu through dual mechanisms—transcriptional activation of survival pathways via hypoxia-inducible factor-1 signaling in cancer cells and paracrine stimulation of angiogenesis through vascular endothelial growth factor-mediated endothelial activation. 19,20 Our clinical observations substantiate this hormonal dependency, likely reflecting the abrupt withdrawal of estrogen-driven proliferative signals following placental expulsion.
Notably, our team’s multiomics investigations reveal an underappreciated dimension of PTC biology. 21 Single-cell RNA sequencing (scRNA-seq) profiling coupled with functional validation has identified tumor-infiltrating B lymphocytes (TIL-B) as key modulators of PTC indolence—a population potentially susceptible to estrogenic regulation given their constitutive expression of estrogen receptors (ER) α and β. This sexual dimorphism in immune microenvironment composition (evidenced by sex-specific B-cell differentiation patterns in scRNA-seq datasets) may explain the clinical paradox wherein female predominance in PTC incidence contrasts with male propensity for aggressive disease. 22 The estrogen-TIL-B axis potentially serves as an immunological rheostat, modulating tumor progression through hormone-responsive lymphocyte populations. 23 Further elucidation of ER signaling networks within this unique immune ecosystem could unveil the effect of pregnancy on changes in PTC growth velocity.
The present study has several limitations. First, the definition of the three periods overlapped: “before pregnancy” spans from the time of the target thyroid nodule diagnosis to the first month of conception, and “during pregnancy” extends from conception to the first month postpartum. Given the extremely slow progression of PTMC, the postpartum recovery period and scheduling delays for US appointments, we believe that this grouping design did not significantly impact the study results. Second, 95.2% of the included cases exhibited indolent tumor features before pregnancy (Table 1), which may have introduced potential selection bias. However, considering the similarly meaningful tumor progression rates reported in other large AS cohorts, the effect of selection bias on the reproducibility of our findings is likely minimal. Third, the median follow-up duration after delivery was 24.0 months, which is insufficient for the evaluation of long-term prognosis, as most patients did not undergo surgery, and thus detailed pathological characteristics were not obtained. Finally, this study included three cases with second pregnancies; the potential cumulative effect of endocrine influences during multiple pregnancies warrants careful evaluation in larger sample sizes.
In conclusion, this study demonstrates that pregnancy may transiently accelerate tumor growth in low-risk PTMC, but such changes are predominantly self-limited, with most cases stabilizing or regressing postpartum. AS remains a safe and feasible strategy for reproductive-age patients, harmonizing oncologic safety with fertility preservation and quality-of-life priorities. However, confirmatory research—incorporating extended follow-up, advanced imaging modalities, and mechanistic investigations into hormonal-immune interactions—is essential to validate these findings and refine clinical frameworks for managing PTMC during pregnancy.
Footnotes
Authors’ Contributions
W.L.: Conceptualization, writing—original draft, writing—review and editing, and funding acquisition. Z.D.: Writing—original draft, writing—review and editing, formal analysis, and visualization. W.C., H.J., Y.L., and P.L.: Resources, data curation, and investigation. X.Y. and R.C.: Writing—review and editing, project administration, and conceptualization. All authors have reviewed the final article and take responsibility for this work.
Author Disclosure Statement
The authors declare that they have no competing interests.
Funding Information
This study was supported by the National Natural Science Foundation of China (Grant No. 82360612), the Yunnan Health Training Project of High Level Talents (Grant No. H-2024050), the Yunnan Revitalization Talent Support Program, and 535 Talent Project of First Affiliated Hospital of Kunming Medical University (Grant No. 2025535Q02).