
Abstract
Background:
The management of advanced thyroid cancer has rapidly evolved as several multikinase, and gene-specific inhibitors have substantially improved survival for patients with most types of thyroid cancer. Optimizing management of the treatment-related adverse events (TRAEs) from these medications is important to improve quality of life and outcomes for patients with thyroid cancer. This narrative review discusses common and clinically significant TRAEs of treatments for thyroid cancer and effective management approaches.
Summary:
Published literature was reviewed to summarize available information on the incidence of TRAEs with medications used to treat thyroid cancer and management approaches for these TRAEs. There are common TRAEs across many treatments for advanced thyroid cancer including fatigue, hypertension, gastrointestinal toxicities, rashes, and hand-foot syndrome. Additionally, several other TRAEs with thyroid cancer treatments are significant because of their frequency with specific medications (e.g., pyrexia syndrome) or their severity (e.g., thromboembolic events and cardiac impairment). Data from clinical trials and real-world data along with expert guidelines and insights from experienced clinicians can guide management approaches for many of these TRAEs.
Conclusions:
The toxicity profiles are well established for treatments for advanced thyroid cancer, there are evidence-based management approaches for many commonly encountered scenarios. Following these approaches to optimizing management of TRAEs can improve the quality of life and outcomes for patients with thyroid cancer.
Introduction
In 2020 there were 500,000 incident cases of thyroid cancer globally and 46,000 cases in North America with over 40,000 deaths globally and 1,000 deaths in North America. 1 Differentiated thyroid carcinomas (DTC), which include papillary thyroid carcinoma (PTC), follicular thyroid carcinoma, oncocytic thyroid carcinoma, and high-grade thyroid carcinomas represent approximately 95% of thyroid carcinomas. The remainder of thyroid cancers include medullary thyroid carcinoma (MTC) and anaplastic thyroid carcinoma (ATC), a rare and aggressive subtype of thyroid cancer.
Most thyroid carcinomas present as early-stage disease and are managed with surgery with or without radioactive iodine (RAI) and have an excellent prognosis. Five-year survival rates are 98–100% for stage I disease and 85–95% for stage II disease. 2 Advanced thyroid cancer is defined as disease that is inoperable, recurrent, RAI-refractory (RAIR) or disease with distant metastases, aggressive histology, a biochemical or volumetric doubling time of <6 months. 3 Disease is defined as RAIR if malignant lesions do not concentrate RAI or disease progresses despite concentration of RAI. 4,5
Patients with advanced thyroid cancer can be on systemic therapy for many months or years, so optimizing quality of life and managing treatment-related adverse events (TRAEs) is particularly important. Effective management of TRAEs is associated with improved adherence, quality of life and outcomes. 6 –8 This review discusses common and clinically important TRAEs of systemic therapies used for thyroid cancer and outlines approaches to optimize management.
Systemic Therapies for Thyroid Cancer
Therapeutic options for patients with advanced thyroid cancer have rapidly evolved in recent years, and treatment selection depends on the histology and molecular profile. Most patients with advanced DTC are initially treated with multikinase inhibitors (MKIs). For patients with DTC without targetable molecular alterations, lenvatinib is the preferred first-line systemic therapy based on data showing a response rate of 65% and progression free survival (PFS) of 18.1 months. 9,10 Vandetanib, sofrafenib and cabozantinib have also been studied in advanced RAIR DTC and were shown to have PFS of 11.1, 10.8 and 11.0 months, respectively. 11 –13 Dabrafenib/trametinib has shown activity in BRAF V600E mutated PTC. 14 In patients with RET alterations and NTRK fusions, selective RET inhibitors (selpercatinib and pralsetinib) and TRK inhibitors (larotrectinib and entrectinib) have high response rates and durable responses. 15 –18 Other drugs such as sunitinib and ALK inhibitors are used in select cases, but are not discussed here. 19
More than 50% of MTCs harbor RET alterations, and RET inhibitors are the recommended first-line treatments for these patients. 16,20 For advanced MTC without RET alterations, cabozantinib and vandetinib are the recommended first-line treatment options. 21,22 For ATC with BRAF V600E mutations, dabrafenib/trametinib are frequently used. 14 Other cases of advanced ATC are treated with chemotherapy and/or immunotherapy, the most common situations in which these classes of medications are used to treat thyroid cancer. 10 Because of the infrequent use of chemotherapy and immunotherapy in thyroid cancer and extensive literature outlining management of chemotherapy- and immune-related AEs, these therapies are not detailed here. 23
Common Toxicities and When to Expect Them
Some TRAEs are common across all drugs and others that only occur in specific drug classes or specific drugs. Overall, the incidence and severity of various TRAEs are higher with MKIs than targeted therapies, though targeted therapies can still have substantial TRAEs (Table 1). This review will focus on TRAEs that occur with all therapies (i.e., fatigue and gastrointestinal), TRAEs associated with certain drug classes (i.e., hypertension in MKIs and RET inhibitors) and other clinically significant TRAEs such as pyrexia and cardiovascular TRAEs.
The Incidence of Common and Significant Treatment-Related Adverse Events with Kinase Inhibitors Used to Treat Thyroid Cancer a
Rates of TRAEs reported here represent the rates reported in the experimental arm of the phase II or phase III clinical trial evaluating the use of each drug in patients with thyroid cancer. For therapies with multiple phase II or phase III trials in thyroid cancer, rates from the trial with the higher number of participants were reported. All numbers reported are rates of any grade of TRAE unless otherwise noted. Table is restricted to TRAEs that occurred in >10% of patients or TRAEs of particular clinical significance.
Due to the small sample size of the phase II trial of dabrafenib and trametinib in differentiated thyroid carcinoma, the rates of uncommon, significant TRAEs reported here are from the phase II trial of dabrafenib/trametinib in patients with melanoma.
Rates listed based on trials evaluating the use of drugs in patients with any malignancy with NTRK fusions.
Cr, serum creatinine; CVD, cardiovascular; DVT, deep vein thrombosis; G3+, grade 3 or greater; GI, gastrointestinal; HFS, hand-foot syndrome/palmar-plantar erythrodysesthesia; LFT, liver function tests; LVEF, left ventricular ejection fraction; NR, not reported; plts, platelets; TRAEs, treatment-related adverse events.
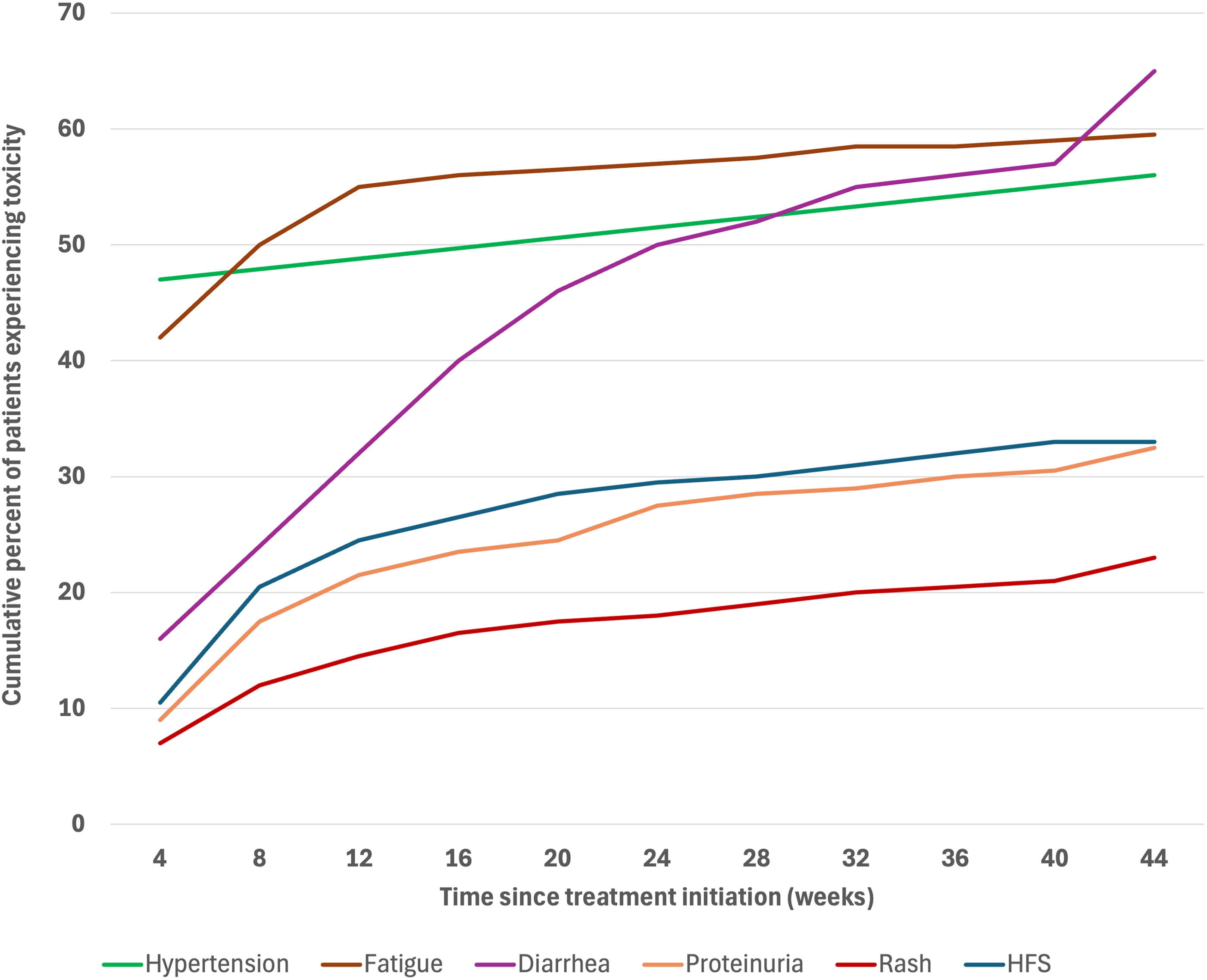
Different TRAEs occur at different times after treatment initiation. With MKIs such as lenvatinib, fatigue and hypertension usually develop within days or weeks after treatment initiation while proteinuria and dermatologic TRAEs are rare in the first few weeks of treatment and develop later (Fig. 1). 26,27 Diarrhea can develop at any point during treatment but is most commonly seen several months after starting treatment, and some cardiac TRAEs, such as electrocardiogram (EKG) changes, thrombosis and arrhythmias may develop more than a year after starting treatment. 28 Recognizing these patterns can help clinicians provide anticipatory guidance to patients and monitor for TRAEs most likely to develop at different points in the treatment course.
How Toxicities Affect Management Prior to Treatment Initiation
Initial management of advanced thyroid cancer differs from management of many other metastatic tumors. While systemic therapy is started shortly after diagnosis for most metastatic cancers, advanced thyroid cancer is often monitored for months or years before systemic therapy is started, and there is no consensus on the optimal timing to start systemic therapy in patients with advanced thyroid cancer. Placebo-controlled clinical trials for DTC and MTC allowed for crossover to the treatment arm after patients progressed on placebo, and several of these trials did not show an overall survival benefit despite substantially improved PFS. These results suggest patients may be able to delay treatment initiation without reducing overall survival, which would allow patients with advanced thyroid cancer more time before exposure to the potential TRAEs of systemic therapy. However, further analysis of study data has shown some patient populations such as those with larger lung metastases may have improved survival with earlier treatment initiation. 29 Thus, the optimal timing of systemic therapy initiation remains unknown. 27,30 Shared decision making with patients about when to start systemic therapy is important to ensure patient preferences are considered alongside factors such as histological diagnosis, disease burden, pace of disease progression and patient comorbidities.
Throughout this period before treatment initiation, we recommend assessing patients’ comorbidities, functional status, and health-related behaviors. These discussions can identify potential issues that may arise with treatment and create opportunities for ‘prehabilitation,’ prospectively working to improve patients’ physical and mental health to help them withstand the challenges of future treatments. 31,32 All patients using tobacco should be encouraged to quit and provided appropriate counseling, and providers should work with multidisciplinary teams to ensure patients’ comorbidities are managed. Using this time to counsel patients on the benefits of physical activity, mobility exercises, nutrition, stress management may also improve quality of life and treatment tolerability. 31,32
Treatment Initiation and Symptom Monitoring
After deciding to start treatment, providers should identify comorbidities that may affect the risk of common TRAEs, and a review of medications to identify QTc prolonging medications and medications metabolized by CYP enzymes, which can be inhibited by several thyroid cancer treatments. All patients should have a laboratory assessment of liver function, creatinine, BUN, comprehensive blood counts, and thyroid function tests, and patients starting a MKI should have a urinalysis to assess for proteinuria. Patients starting a MKI or a RET inhibitor should receive an EKG to record a baseline QTc interval, and any patient with known cardiac issues should have an echocardiogram to document baseline cardiac function. 33,34 All females of childbearing age should have a negative pregnancy test within 72 hours before treatment initiation, and they should be counseled on the importance of effective contraception while on treatment.
Providing anticipatory guidance on potential TRAEs and encouraging prompt symptom reporting enables early intervention. Patient should be provided written information about what TRAEs to anticipate, when to seek help and instructions on how to contact their care team during and outside of regular working hours. Given high rates of diarrhea and nausea with most thyroid cancer treatments, providers should discuss how and when to use loperamide and discuss potential antiemetics if nausea develops. Clinicians should emphasize that there are effective management approaches for most TRAEs, but symptoms may persist and intensify if patients continue treatment without intervention.
After starting treatment, a standardized approach to lab and symptom monitoring can help ensure patients are on appropriate prophylaxis and that potential AEs are not missed. When starting lenvatinib, we recommend the monitoring regimen shown in Figure 2 during the first 8 weeks of treatment. Subsequent lab and symptom monitoring can be tailored based on the patient’s experience during the first few weeks of treatment.
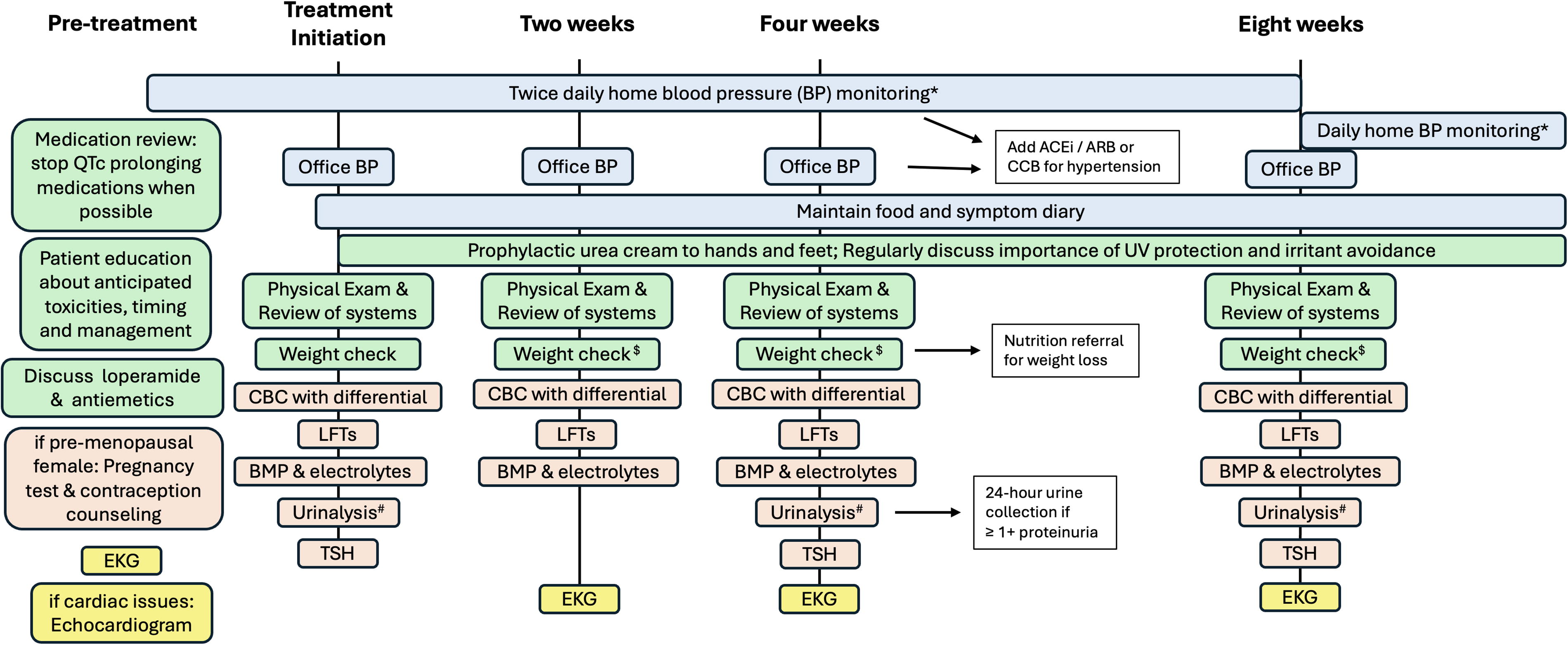
Suggested monitoring approach of potential adverse events after starting lenvatinib and other multikinase inhibitors.^
Dose Modifications When Managing TRAEs
For most TRAEs seen with thyroid cancer treatments, supportive care should be maximized before considering dose reductions. Randomized data show that lenvatinib has greater efficacy when started at 24 mg daily compared to 18 mg daily, and significantly, the rate of grade 3 side effects was similar at the lower dose. 35 Additionally, data suggest that quality of life is not better at lower doses. 36 Therefore, the goal of TRAE management should be to help patients remain on the highest dose possible and maximize supportive care to improve quality of life. However, due to severe or persistent symptoms, dose holds and reductions are frequently required.
Some data suggest that necessary dose holds may not reduce treatment efficacy. 25 Dose holds should be kept short, ideally less than 2 weeks, as shorter dose have been associated with better outcomes. 37 Additionally, any time treatment, particularly TRK inhibitors, is held, patients are at risk of withdrawal pain, so patients should be counseled about this possibility and clinicians should be prepared to assist with pain management. 38 While guidelines can provide assistance, managing TRAEs involves substantial nuance, and clinicians should individualize dosing based on the patient’s experience. 39 Approaches such as planned dosing holidays have proven effective at managing potentially severe TRAEs, and should be considered. 40
Approach to Common TRAEs
Hypertension
Hypertension is a common toxicity of MKIs and RET inhibitors, occurring in 68% of patients on lenvatinib and 43% of patients on selpercatinib. 9,20 Ensuring patients are normotensive before initiating treatment and close monitoring after initiation, with rapid adjustment of antihypertensive medications, is essential to avoid treatment discontinuation, dose reductions and serious adverse events such as cerebrovascular events (CVAs) and posterior reversible encephalopathy syndrome. Data from the SELECT trial suggest that treatment-related hypertension is associated with increased OS, so optimal management of blood pressure to prevent treatment discontinuation due to HTN may be particularly important for these patients. 27
Blood pressures (BPs) often rise within one month of starting treatment and sometimes increase as soon as 1–2 days after starting treatment, so active early management is essential. 41,42 Home blood pressure monitoring should begin prior to treatment initiation to ensure patients can regularly check their BPs at home and to confirm BPs are at goal before starting treatment. Patients should check and record home BPs twice daily and review values with their care team. After treatment initiation, patients should be told to immediately contact their care team if they have two sequential BP readings with a systolic blood pressure >160 mmHg or a diastolic blood pressure >90 mmHg. Home BP logs should be reviewed at regular clinic visits, and out of office BP measurements should be used to adjust antihypertensives. 43 If there are discrepancies between home BPs and office BPs, patients should be observed checking their BP to ensure they are using correct technique and functioning equipment.
Antihypertensives should be increased sequentially with the sequence guided by patient comorbidities. For patients with normal renal function, calcium channel blockers and ACE inhibitors or ARBs are usually the first two classes of antihypertensives used. In patients with kidney disease, start an ACE inhibitor/ARB first. If BPs remain elevated despite using three or more antihypertensives or patient comorbidities restrict the antihypertensive options, involving Cardiology and Nephrology for multidisciplinary management of hypertension is encouraged. Lenvatinib, sorafenib and RET inhibitors have half-lives under 36 hours, so treatment-associated hypertension can resolve within days of stopping the drug. To avoid hypotension during a drug holiday, antihypertensives may need to be adjusted.
Other cardiovascular TRAEs
QTc prolongation can be seen with all systemic therapies for advanced thyroid cancer, but it is most commonly seen with lenvatinib, vandetanib and RET inhibitors. 34,44 While QTc prolongation is asymptomatic, it should be carefully managed to avoid arrhythmias and sudden cardiac death. Prior to starting treatment with lenvatinib, vandetanib or RET inhibitors, any concurrent QTc prolonging medications should be stopped, if possible. A pre-treatment EKG should be done to measure the baseline QTc. The optimal frequency of EKG monitoring with these medications is not established. Our practice is to repeat EKGs 2, 4, and 8 weeks after initiating treatment (Fig. 2), and then with each restaging scan if no new abnormalities are detected. 45 EKGs should be repeated more frequently if the QTc is increasing. If the QTc rises to >500 ms and all concurrent QTc prolonging medications have been stopped, hold treatment until the QTc returns to the normal range and then restart with a dose reduction. 34
Bleeding and thrombotic events have been associated with all MKIs used to treat thyroid cancer and dabrafenib/trametinib. 9,46,47 Management of bleeding events depends on the severity of the bleeding. Mild bleeding events such as self-limited epistaxis do not require dose modifications while life-threatening bleeding should prompt a dose hold or treatment discontinuation. Venous thrombotic events occur in up to 5% of patients with some medications (Table 1). Arterial thrombotic events are less common, but elevated rates of acute coronary syndrome and CVAs are seen with MKIs and BRAF/MEK inhibition. 48 Other uncommon but serious cardiovascular events associated with treatments for thyroid cancer include cardiomyopathy, decreased left ventricular ejection fraction (LVEF), and congestive heart failure. 49 Decreased LVEF was reported in 9% of patients with melanoma who were treated with dabrafenib/trametinib. 25 Depending on the severity of these complications, they may require permanent treatment discontinuation. Of note, cardiovascular complications are seen more frequently later in treatment, so clinicians should closely monitor for evidence of cardiovascular TRAEs through the entirety of treatment. 28
Dermatologic and mucosal TRAEs
Dermatologic TRAEs are common with all thyroid cancer treatments apart from TRK inhibitors. TRAEs include pruritis, rashes, hand-foot syndrome (HFS) and cutaneous squamous cell carcinomas, which occur in 4–6% of patients on RAF inhibitors and some patients on MKIs. 50 Generally, dermatologic TRAEs should be managed with preventative and supportive care, and most patients are able to continue treatment uninterrupted with early, appropriate management.
Rashes occur in 10–30% of patients with most treatments and more than 50% of patients on sorafenib and vandetanib. 34 They can present as acneiform, diffuse erythema, erythematous papules (Grovers disease), dermatitis, photosensitivity, or hyperkeratosis. When starting treatment, patients should be recommended to use fragrance-free moisturizing creams, avoid direct sunlight during peak hours, wear clothing with (ultraviolet) UV protection and apply sunscreen of at least sun protection factor 30 prior to any sun exposure. 51 Prophylactic low potency topical steroids can also be used.
Specific management of rashes varies based on the location, type, and severity of the rash, but Figure 3 outlines a general approach to managing treatment-related rashes. For mild to moderate rashes (grade 1 or 2), treatment can be continued, and supportive care should include low to moderate potency topical steroids and moisturizing creams. For pruritis, oral antihistamines can be helpful. Topical or oral antibiotics can be effective for acneiform or pustular rashes, and creams containing salicylic acid can help with hyperkeratosis. Any rash that affects a patient’s ability to carry out their ADLs, should prompt referral to Dermatology. Treatments to consider for severe rashes include oral or topical analgesia, nonsteroidal anti-inflammatory drugs (NSAIDs), and low-dose oral steroids. If these measures are not sufficient, then dose holds and/or dose reductions may be needed. Panniculitis, which can be seen with dabrafenib/trametinib, usually improves with time, so patients should be managed supportively, as able, while continuing treatment.
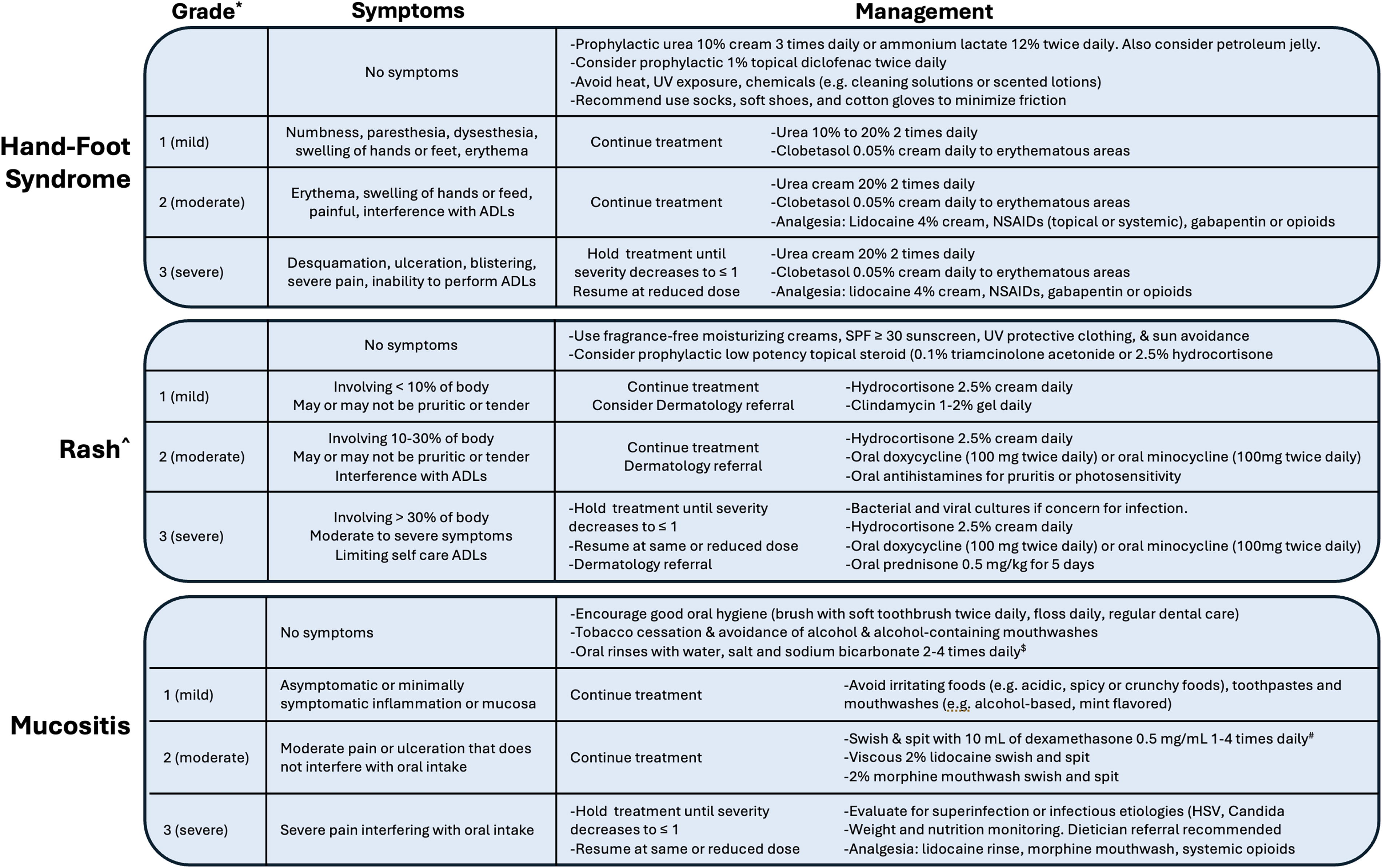
Suggested management algorithms for dermatologic and mucosal adverse events commonly seen during treatment for thyroid cancer. *Grades based on CTCAE version 5.0.^Grading and management can vary by specific type of rash (i.e., acneiform or maculopapular). For example, oral antibiotics have greater efficacy with acneiform rashes.$Patients can make oral rinses at home by mixing 1 pint water, 1 teaspoon salt (sodium chloride) and 1 teaspoon baking soda (sodium bicarbonate).#Patients using dexamethasone swish and spit should be monitored for oral candidiasis.ADLs, activities of daily living; CTCAE, common terminology criteria for adverse events; HSV, herpes simplex virus; NSAIDs, nonsteroidal anti-inflammatory drugs; SPF, sun protection factor; UV, ultraviolet.
Hand-foot syndrome (HFS), also known as palmar-plantar erythrodysesthesia, is seen in 24–45% of patients treated and MKIs and 22% of patients on dabrafenib/trametinib. 47,52 HFS can substantially decrease quality of life and impair daily activities. A recommended management approach is shown in Figure 3. 51,53 Randomized controlled trial data support using prophylactic low potency urea- or ammonium-based moisturizers to reduce HFS. 54,55 Patients should be counseled to avoid heat, UV exposure and chemicals (e.g., cleaning solutions or scented lotions) and encouraged to use socks, soft shoes, and cotton gloves to reduce excessive friction on hands and feet. Prophylactic topical diclofenac may also be considered based on randomized data showing it reduced HFS incidence in patients on capecitabine. 56 For mild HFS, apply a topical high potency steroid such as clobetasol 0.05% twice daily to the affected area and increase the concentration of urea cream to 20% or higher. If patients require analgesia, lidocaine cream can be used initially, and then NSAIDs (topical or systemic), gabapentin and opioids can be added as needed. When possible, continue treatment as HFS can improve over time with treatment continuation and supportive management. 57 However, severe pain or inability to perform ADLs should be treated with a dose hold followed by a dose reduction after symptoms improve.
Mucositis is seen with several MKIs such as lenvatinib, sorafenib and cabozantinib (Table 1). 9,12,24 Suggested management is shown in Figure 3. Smoking cessation, reduction of alcohol and good oral hygiene should be encouraged to reduce the risk of mucositis. 58 With mild to moderate symptoms, instruct patients to avoid irritating foods, toothpastes and mouthwashes. 53 Dexamethasone swish and spit can reduce the severity of mucositis associated with cancer therapies. 59 When studied in patients on everolimus, patients were instructed to rinse with dexamethasone solution 4 times daily. In our practice, we have seen efficacy with lower frequencies of once or twice daily, but lower dosing regimens have not been formally evaluated. All patients prescribed dexamethasone should be counseled about the risk of oral candidiasis and regularly monitored for signs or symptoms of thrush. Mild to moderate pain from mucositis can be managed with viscous 2% lidocaine rinses or 2% morphine solution oral rinses, and systemic opioids are recommended for severe oral pain. 45 Monitoring weight, nutrition and hydration is essential in patients experiencing mucositis. Early dietician involvement is encouraged, and patients unable to obtain hydration or nutrition may need hospitalization.
Fatigue and asthenia
Asthenia and fatigue are common with all treatments for thyroid cancer with rates or fatigue ranging from 16–35% with RET and TRK inhibitors to over 50% with lenvatinib and dabrafenib/trametinib (Table 1). 9,16 –18,20,47 Fatigue can begin days after starting treatment, so patient education prior to treatment initiation is important.
All patients with new fatigue should be evaluated for anemia, liver and renal dysfunction and metabolic derangement. Patients should also have a TSH checked if it hasn’t been done recently. Multiple TKIs can affect thyroid hormone metabolism, and a high proportion of athyreotic patients have increases in TSH while on treatment. 60 Additional evaluations should include screening for depression, which may affect more than 20% of patients on active treatment for cancer, 61 and evaluation for adrenal insufficiency with a cortisol stimulation test. The prevalence of adrenal insufficiency in patients treated with MKIs has not been established, but case series of patients on lenvatinib and vandetanib suggest is could be as high as 50%. 62,63
After potentially reversible causes of fatigue has been excluded, mild to moderate fatigue should be initially managed while continuing treatment. When possible, refer patients to specialists who can support lifestyle interventions shown to improve fatigue in patients with cancer including exercise, psychosocial counseling, nutritional support, sleep optimization, and mind-body interventions such as yoga and meditation. 64 Where specialist support is not available, patients should be directed to education resources such as those published by the American Cancer Society and the National Cancer Institute. 65,66 While stimulants are often used for treatment-associated fatigue, studies show stimulants do not improve in fatigue or quality of life relative to placebo. 64,67 Palliative Care referrals can be helpful when considering stimulants or other pharmacologic interventions. Dose reduction and dose holds should be reserved for severe asthenia and fatigue that affects a patient’s ability to perform their activities of daily living or fatigue that worsens despite lifestyle interventions.
Gastrointestinal TRAEs
Gastrointestinal effects, particularly diarrhea, nausea, anorexia and weight loss, are common with all thyroid treatment, particularly MKIs where these symptoms are seen in more than half of patients (Table 1). 68 Prior to treatment initiation, patients should be educated on foods that can be associated with gastrointestinal symptoms, though prophylactic dietary changes are not recommended. Patients should be encouraged to keep a food diary to assess whether any foods are associated with symptoms. 53,69
For new diarrhea, clinicians should evaluate the severity of the diarrhea and consider the risk of alternative etiologies such as infection, inflammatory conditions or immunotherapy-associated diarrhea in patients receiving concurrent or prior immunotherapy. After these possibilities are excluded, mild to moderate diarrhea can be managed with dietary changes, oral rehydration, and loperamide (2 mg every 2 hours as needed). Specific dietary recommendations include avoiding caffeine, alcohol, dairy and greasy foods and increasing dietary fiber. 68,70 Additional pharmacologic options to consider include diphenoxylate/atropine, codeine and tincture of opium. Diarrhea may not resolve completely, so the goal of management is to achieve a level of symptoms that minimally affects quality of life, usually ≤2 loose stools per day. If symptoms do not sufficiently improve after 1–2 weeks with maximum supportive care, treatment should be held for 1 week and then restarted at the same dose. 69 For recurrent, intractable diarrhea, dose reductions are indicated. With close monitoring and active management, treatment-related severe (≥7 loose bowel movements per day) diarrhea should be avoidable; however, if patients present with severe diarrhea, electrolytes and hydration status should be assessed and acutely managed.
All patients with weight loss ≥5% of baseline body weight should be referred to a dietician. Patients should be counseled on the importance of small, frequent meals and high-protein, high-calorie foods and nutritional supplements. If patients have weight loss of ≥10% of baseline body weight, treatment should be held for 1 week and then restarted. If intake and weight loss do not improve after 1 week off treatment, alternative etiologies should be explored. Recurrent weight loss that does not respond to any of these interventions may require a dose hold and dose reduction. 69
Guidelines for managing nausea and vomiting while on antineoplastic therapy are detailed elsewhere. 71 Nausea and vomiting while on MKIs and targeted therapies should be managed with maximum supportive care before considering dose reductions. In patients with persistent nausea, multiple classes of antiemetics should be trialed to try to find an effective regimen.
Gastrointestinal perforation is a rare but serious side effect of MKIs, and it can be challenging to identify. Clinicians should always consider this possibility when patients present with gastrointestinal issues with additional symptoms or if issues not resolve with standard management. 34,72 Gastrointestinal perforations without an obvious cause unrelated to the MKI require urgent surgical consultation and treatment discontinuation.
Renal and electrolyte abnormalities
Several thyroid cancer treatments have potentially significant nephrotoxicity including instances of acute renal failure. Weight, peripheral edema, and electrolytes should be closely monitored while on treatment, and suspected changes in renal function should be promptly evaluated. Renal function can be monitored with BUN and creatine measurement. However, several drugs used for thyroid cancer (selpercatinib, entrectinib, vandetanib, and cabozantinib) can inhibit MATE-1, a transporter in the proximal tubules of the kidney that assists with creatine excretion independent of GFR. 73 –76 In patients with creatinine increases while on these drugs, cystatin C can distinguish between MATE-1 inhibition and renal impairment.
Proteinuria is seen in 31% of patients receiving lenvatinib and at lower rates with other MKIs. 9,12,13,21 It can be an early or late toxicity, so proteinuria should be monitored during treatment initiation and continued through the duration of treatment. Patients can be monitored with qualitative assessments of proteinuria (e.g., urine dip stick or urinalysis), urine albumin:creatinine or urine protein:creatinine ratios. 77,78 Any qualitative urine result ≥1+ or elevated urine ratios should be assessed with a 24-hour urine collection whenever possible. An ACE inhibitor or ARB should be started in all patients with proteinuria. 79 For proteinuria ≤2.0 g/24 hours with no evidence of edema or elevated creatinine, treatment can be continued with close monitoring. If proteinuria exceeds 2.0 g/24 hours, lenvatinib should be held until proteinuria resolves to ≤2.0 g/24 hours and then restarted at a reduced dose. 53 Treatment should be permanently discontinued in any patients who develop nephrotic syndrome. All patients who develop proteinuria prompting consideration of a dose hold should be referred to Nephrology.
Edema, most commonly in the lower limbs or face, can be seen with most thyroid cancer therapies. 80 Treatment-associated edema is usually not responsive to diuretics while continuing therapy; however, diuretics can be trialed to assess for clinical benefit. Try to continue therapy when patients develop edema and manage symptoms with supportive measures such as compression wraps and low-dose steroids, both of which can be effective. For edema that causes significant pain or interferes with a patient’s functional status and does not respond to supportive measures, treatment should be held for 1 week and then restarted at a lower dose.
Potentially severe electrolyte abnormalities, particularly hypocalcemia with MKIs and hypophosphatemia with dabrafenib/trametinib and RET inhibitors, can be seen during thyroid cancer treatment. Rates of hypocalcemia while on MKIs are higher among patients with thyroid cancer compared to patients with other malignancies. This is thought to be due, at least in part, to postsurgical hypoparathyroidism in patients with thyroid cancer; however, MKI-associated hypocalcemia can be PTH-dependent or PTH-independent. 81 Mild to moderate hypocalcemia (corrected Ca ≥7.0) can be managed with oral calcium and vitamin D supplementation and then calcitriol while continuing treatment. However, patients who develop severe hypocalcemia despite these interventions (corrected calcium <7.0 mg/dL) require dose holds and inpatient admission for treatment with IV calcium gluconate. Other electrolytes are managed with close monitoring, oral or IV supplementation and dose holds in severe cases. Treatment can be restarted after severe electrolyte abnormalities, but patients should be closely monitored as recurrence rates are high. 81
Other Significant TRAEs
Pyrexia syndrome
Pyrexia syndrome involves fevers, chills, rigors and/or flu-like symptoms, and occurs in 50–70% of patients receiving dabrafenib/trametinib. 47,82 Though initially thought to be just due to dabrafenib, the rate of pyrexia is higher with combination therapy and it is now believed that trametinib also contributes to this syndrome. In patients treated with one year of dabrafenib/trametinib who experience pyrexia, the median number of episodes was 2 and 21% of patients had four or more episodes. The median time from treatment initiation to the first episode was 19 days with a range of 1 to 81 days. 83 Prior to treatment initiation, it is important to inform patients of the likelihood of experiencing pyrexia, discuss potential management, and provide instructions for how to promptly contact their care team.
Our approach to managing pyrexia syndrome, adapted from Atkinson and colleagues’ management algorithm, is shown in Figure 4. 33 For fevers ≥38.0 or other symptoms of pyrexia syndrome, treatment should be held and patients should be managed supportively with acetaminophen and NSAIDs. Both dabrafenib/trametinib should be held based on data from the COMBI-APlus trial showing lower rates of severe pyrexia, pyrexia-related hospitalizations and treatment discontinuation when both medications were held. 82 It is important to remember that other conditions including infections can present with fevers, so providers must keep a broad differential. 84 If patients have severe symptoms (symptoms requiring hospitalization or CTCAE v5.0 grade ≥2) or there is a concern for active infection, they should be immediately evaluated including an infectious workup. 85 Other situations that should prompt consideration of alternative etiologies include patients whose symptoms do not improve after treatment is held or persistent symptoms more than 5 days after treatment cessation.
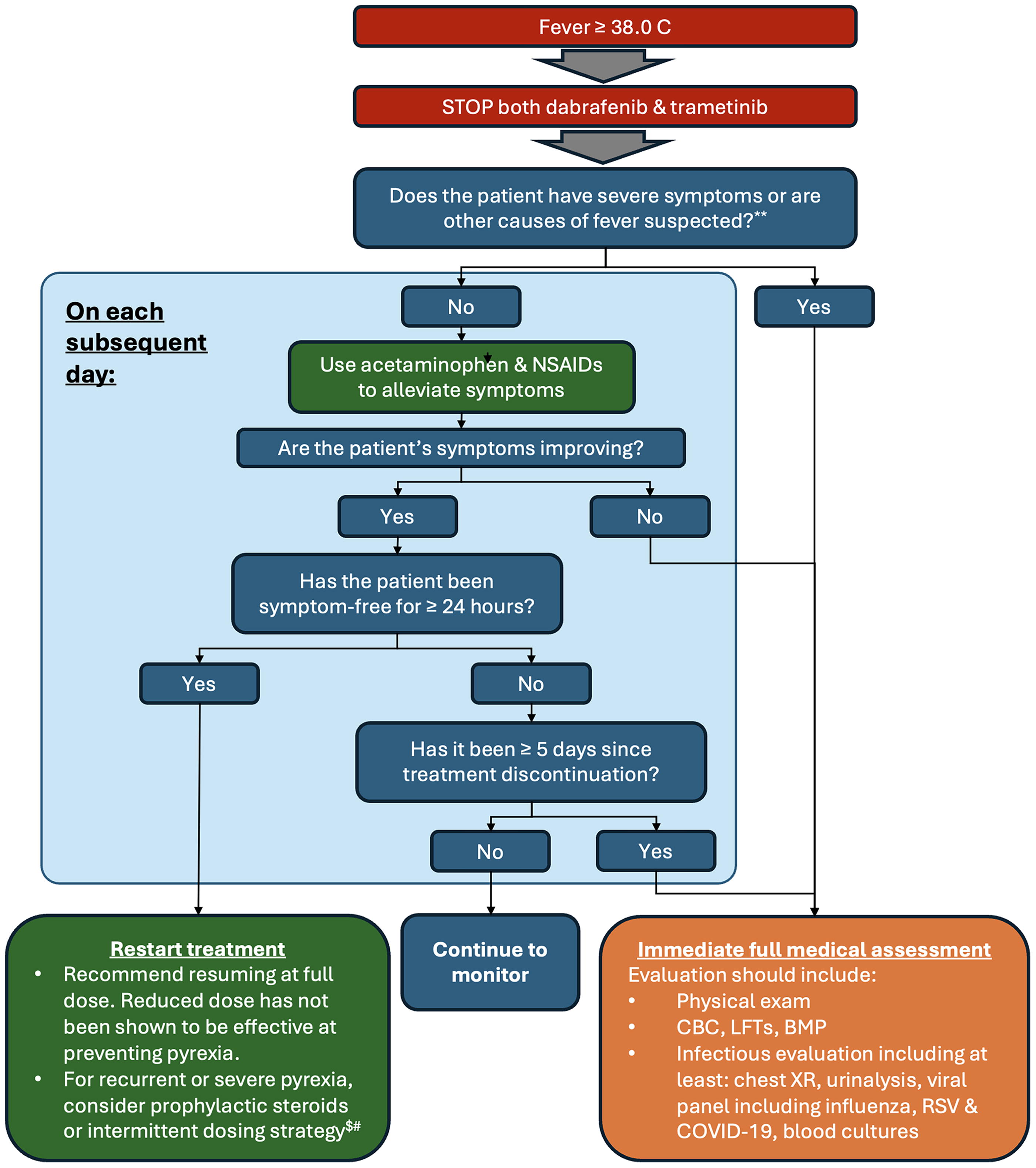
Flowchart for management of dabrafenib/trametinib-associated pyrexia syndrome.**Adapted with permission from Atkinson et al., Asia-Pacific Journal of Clinical Oncology 2016. 33 **Severe symptoms include any symptom requiring hospitalization or CTCAE v5.0 grade 2 or higher dehydration, renal impairment, hypotension, confusion or vomiting. 85 $For steroid dosing, we recommend a starting dose of 10–20 mg/day with a plan to slowly taper if patients remain afebrile for at least 4 weeks. If pyrexia syndrome continues at these doses, some patients may require higher doses.#Intermittent dosing strategies should be designed based on patient experience. For example, if a patient experiences pyrexia syndrome every 2–3 weeks, consider a treated for 12 days followed by a 2-day break.BMP, basic metabolic panel; CBC, comprehensive blood count; CTCAE, common terminology criteria for adverse events; LFTs, liver function tests; NSAIDs, nonsteroidal anti-inflammatory drugs; RSV, respiratory syncytial virus.
Dabrafenib/trametinib should be restarted after symptoms have been resolved for ≥24 hours. Both medications should be restarted at the full dose as dose reductions do not reduce rates of recurrence. The benefits of acetaminophen and NSAIDs for secondary prophylaxis are not clear, so clinicians should discuss the risks/benefits of prophylactic antipyretics with patients to determine whether to start them. 86 For severe or recurrent pyrexia, corticosteroids should be considered for secondary prophylaxis. These can be started at a dose of prednisone 10–20 mg daily and slowly tapered after patients have been afebrile for at least 4 weeks. If pyrexia recurs on steroid prophylaxis and all other potential etiologies have been excluded, higher doses of steroids can be trialed. Interrupted dosing should also be considered for recurrent pyrexia as data suggest dose interruptions may not reduce treatment efficacy. 25 Dosing schedules should be patient-specific based on the pattern of their symptoms. For example, if a patient develops pyrexia 2–3 weeks into treatment, a schedule of 12 days on treatment followed by a 2-day drug holiday may be effective.
Ocular TRAEs
Ocular TRAEs are a class effect of MEK inhibitors, and TRAEs including retinopathy, retina detachment, and retinal vein occlusion can be seen in patients on dabrafenib + trametinib. 87 The precise incidence is or ocular TRAEs with dabrafenib + trametinib is not known due to variation in reporting across trials but they likely occur in less than 15% of patients. 25,47 Rates of ocular toxicity are higher with other MEK inhibitors including binimetinib. 88,89 Ophthalmological screening is not required for patients on MEK inihibitors. 90 However, if visual symptoms develop on treatment with dabrafenib + trametinib, trametinib should be held and urgent Ophthalmology consultation arranged. As these TRAEs are due to MEK inhibition, dabrafenib can usually be continued through ocular TRAEs. For retinopathy and retinal detachment, trametinib should be held for up to 3 weeks, and the decision to discontinue or restart should be made with an Ophthalmologist based on the degree of improvement in symptoms during the dose hold. For retinal artery occlusion, trametinib should be permanently discontinued. Uveitis is associated with dabrafenib, and can be managed with dose holds and reductions though severe or persistent uveitis requires permanent discontinuation of dabrafenib. 91
Other significant but uncommon TRAEs
Cytopenias are uncommon with MKIs but can be seen with BRAF/MEK, RET and TRK inhibitors. Mild to moderate cytopenias can be managed with observation while continuing treatment. Brief dose holds followed by dose reductions may be required for grade 3 or greater cytopenias. Fistula formation is a rare but serious TRAEs with MKIs, particularly lenvatinib, and it often requires treatment discontinuation. 92,93 RET inhibitors are associated with chylous effusions, which can be initially confused with disease progression, and erectile dysfunction. 45,94,95
Conclusion
Novel therapies such as lenvatinib, dabrafenib/trametinib and selpercatinib have substantially improved survival for patients with thyroid cancer. However, these medications have several common TRAEs that can impair quality of life and reduce time on treatment if not effectively managed. Because of the indolent nature of most thyroid cancers, relatively low symptom burdens from the disease, and long durations of treatment, managing TRAEs is of particular importance in thyroid cancer. Many TRAEs can be detected early with proactive monitoring and effectively managed using evidence-based approaches. With more advanced TRAEs or those that do not respond to standard treatments, multidisciplinary collaboration is essential help identify strategies to manage TRAEs and optimize patients’ quality of life. With these approaches, clinicians should be able to help increase time on treatment, improve quality of life and maximize treatment efficacy for patients with thyroid cancer.
Footnotes
Authors’ Contributions
T.J.R. made substantial contributions through study design, data collection, analysis, and article writing. L.J.W. made substantial contributions through study conception, study design, analysis, and review. All the authors approved the final version of the article to be published and agree to be accountable for all aspects of the work.
Author Disclosure Statement
T.J.R. reports serving as a non-independent board director for Biocon Biologics, Ltd. He also reports equity holdings in Syngene International, Ltd., Biocon Ltd., and Bicara Therapeutics. L.J.W. reports serving as a consultant for Bayer Healthcare, Blueprint Medicines, Eli Lilly, Exelixis, EMD Serono, Illumina, Nested Therapeutics, Ellipses, Novartis, and Merck. She received research support from Eli Lilly, Ellipses and Novartis.
Funding Information
No funding was received for this article.