
Abstract
Background:
Over the past several decades, there have been indications of potential shifts in the diagnostic strategies and treatment of patients with Graves’ disease (GD) and thyroid eye disease (TED). The objective of this study was to evaluate current practices in managing GD when complicated by moderate-to-severe TED worldwide.
Methods:
We recently reported results from a global online survey of endocrinologists comparing the management of GD in different scenarios. The current analysis focuses on regional differences in the diagnosis and treatment of GD when complicated by TED.
Results:
A total of 1252 respondents from 85 countries completed the survey. Regarding the initial diagnostic and treatment measures, there were no differences among the various geographical regions. Regarding the treatment of moderate-to-severe TED, the use of sodium selenite was higher in Europe (66.5%) and Oceania (60%) compared to other regions (p < 0.001). North American respondents were more likely to recommend teprotumumab and less likely to use glucocorticoids (p < 0.001). When comparing the treatment options for GD in patients with TED, although prolonged use of antithyroid drugs (ATD) remained the first choice in all regions, respondents from Europe, North America, and Oceania were more likely to recommend thyroidectomy than those from other regions (p < 0.001). Ophthalmologists, rather than endocrinologists, would more often be responsible for prescribing advanced medical therapy for TED in North America, Oceania, and Africa, while endocrinologists would have primary responsibility in other regions of the globe.
Conclusions:
Although there are regional differences, respondents generally employ the recommended diagnostic tools, treatments, and a multidisciplinary approach suggested by current clinical practice guidelines. However, there were examples of deviations from current guidance from professional societies.
Introduction
Thyroid eye disease (TED), also known as Graves’ orbitopathy, Graves’ ophthalmopathy and thyroid-associated ophthalmopathy, is the most prevalent extrathyroidal manifestation of Graves’ disease (GD), being present clinically in up to 40% of patients. 1 Patients who are euthyroid or hypothyroid with positive anti TSH receptor (TSH-R) antibodies can also develop TED, but these instances are uncommon, representing fewer than 5% of TED cases. 2 TED presentations vary from mild disease with minimal impact on appearance, visual function, or quality of life, to sight-threatening manifestations requiring urgent intervention, including orbital decompression. 3 The use of diagnostic tools has increased in the last 30 years, with orbital CT scans and MRI becoming more widely available. Also, newer, more targeted therapies, particularly immunobiological agents such as teprotumumab, have the potential to improve ophthalmic outcomes and quality of life, but remain unavailable in many parts of the world because they have not been approved by the various regulatory agencies. Recent guidelines and consensus statements provide recommendations for the diagnosis and management of the full spectrum of TED presentations and emphasize the need for a multidisciplinary team approach. 1,3
To identify the shifting management approaches to TED, we performed a global survey of endocrinologists and related specialists to (i) assess international differences in diagnostic and therapeutic approaches to TED, (ii) compare differences in regional management of moderate-severe TED compared with an uncomplicated patient with GD, and (iii) evaluate the impact of respondent characteristics and demographics on treatment choices for TED.
Methods
Survey methodology and question design strategy
This is a cross-sectional online survey; the methodology and question design were described previously. 4 Briefly, a GD patient with TED (Table 1) was described, together with a series of questions regarding diagnostic methods, treatment recommendations, primary treatment for GD when complicated by TED, and respondent demographics. The target groups for the survey were clinically active international members of endocrine societies and thyroid societies. For a complete list of medical societies and the survey, see Supplementary Data. 5 The present study is a preplanned secondary analysis of the online survey results. This study aimed to compare regional differences in GD treatment in the presence of TED, against current clinical practice guidelines and a recent joint consensus statement from the American Thyroid Association and European Thyroid Association. 1 Accordance with guidance is reported as the percentage of respondents in each region whose response to a given question is concordant or discordant with this professional society guidance. Anonymous survey research is considered exempt from IRB approval at the authors’ institutions.
Case Summary of a Patient with Graves’ Disease and Concomitant Thyroid Eye Disease
Collection and summary of responses
The survey was written in English and was open from May 1 to August 31, 2023. Only one response from the same IP address was permitted by the survey service default settings. All responses were anonymous and stored electronically on the server.
The outreach to potential respondents was previously published; in summary, the societies members were contacted by email according to the practices of each individual society; the Endocrine Society permitted posting of the survey link twice on their community forum webpage, focusing on participants interested in thyroid disease.
Statistical analysis
The responses to each question were analyzed with summary statistics. Not every respondent answered every question. Therefore, the response data were analyzed as a percentage of the specific responses to each question divided by the total number of responses to that question. We explored the relationship between the categorical variables of age, sex, geographic region, and society membership with the selected options for the initial diagnostic evaluation, treatment, and referral patterns for GD and TED. Chi-square or Fisher exact tests were applied to compare differences in proportions by gender, age, and geographical region. The degree of association between categorical variables was assessed by the Cramer V test. The SAS System for Windows (Statistical Analysis System), version 9.4. SAS Institute Inc, 2002–2012, Cary, NC, USA, was used to analyze the survey responses.
Results
Respondent demographics and society membership
The evaluation of patients with TED
Of the 1429 respondents who began the survey, 1252 (87.6%) completed the entire survey. As previously reported, 4 1239 respondents provided society membership data. Among respondents, 48.5% (602/1239) were Endocrine Society members, 20.9% (260/1239) American Association of Clinical Endocrinology members, 20.5% (254/1239) American Thyroid Association members, 12.1% (151/1239) European Thyroid Association members, and 10.5% (131/1239) Brazilian Endocrine Society members. Fewer than 10% were members of other societies, including the Asia and Oceania Thyroid Association (9.6%, 119/1239), and the Latin American Thyroid Society (9.4%, 117/1239). Additional societies, representing <5% of all responses included the European Society of Endocrinology, and the Korea Thyroid Association). 4 Membership in more than one society was reported by 38.1% (473/1239) of respondents, and 15.7% (195/1239) respondents did not report membership in a professional society. The actual survey questions, the response rate per society, and the initial treatment for GD by geographical region are provided in the Supplementary Data. 5 Respondent demographics are summarized in Table 2.
General Characteristics of Survey Respondents
The survey respondents’ demographics were published previously. 4 To summarize, 58.1% (728/1252) of respondents were women, 40.6% were men (508/1252), and 1.3% (16/1252) did not respond to this question. Age groupings were ≤35 years (13.2% [165/1244]), 36 to 50 years (45.0% [560/1244]), 51 to 65 years (27.6% [344/1244]), and >65 years (14.1% [175/1244]). Responses were submitted from 85 different countries. The geographical regions by United Nations categories and general characteristics of the respondents are described in Table 2.
International differences in evaluation and treatment of TED
There were no differences among the various geographical regions regarding the initial evaluation. According to previously published data, 4 23.4% (306/1306) requested visual field testing; radiological examinations involving the eye were requested by 47.6% (622/1306) of respondents, including orbital CT for 24.6% (321/1306) and orbital MRI for 23.1% (300/1306). Also, 90.2% (1178/1306) referred this patient to an ophthalmologist with experience in TED management. Only 3.8% (50/1306) of the respondents did not request additional diagnostic studies or refer to an ophthalmologist. Initial treatment measures, including advice to stop smoking and the provision of lubricating eye drops, were selected by 87% (1136/1306) and 78.7% (1028/1306) of respondents, respectively. Sodium selenite would be recommended by 41.7% (545/1306), systemic glucocorticoids by 58.1% (759/1306), and teprotumumab by 16.1% (210/1306). 4
When the geographical region of respondents was analyzed, the referral rate to ophthalmologists with experience in TED management was >90% in all regions, except for respondents in Latin America, where the referral rate was 83.6% (270/323) (p < 0.001). Ophthalmologists, rather than endocrinologists, would more often be responsible for prescribing advanced medical therapy for TED in North America (75%), Oceania (68%), and Africa (58%), while endocrinologists would have primary responsibility in the other regions of the globe (Europe (63%), Latin America (63%), Asia (62%) and the Middle East (52%). Table 3 summarizes key survey findings by region.
Use of Various Therapies for TED and Geographical Respondents
Respondents from each geographical location: Africa n= 29 (2.3%), Asia n = 307 (24.6%), Europe n = 170 (13.6%), Latin America n = 323 (25.9%), North America n = 263 (21.1%), Oceania n = 85 (6.8%), the Middle East n = 71 (5.7%).
TED, thyroid eye disease.
The use of sodium selenite was higher in Europe (66.5%) and Oceania (60%) compared to other regions (p < 0.001). There were also significant differences regarding the use of glucocorticoids. Asian respondents had the highest rates (80%-243/306), and North American respondents had the lowest rates (23%-61/263). North American respondents were more likely to recommend teprotumumab and less likely to use glucocorticoids (p < 001). Of note, during the survey period, teprotumumab had only received approval for use in the United States.
Differences in approach to GD with TED versus an uncomplicated GD case
Compared to the treatment of uncomplicated GD, for primary treatment of hyperthyroidism in patients with concurrent TED, there was a decrease in the use of ATD (from 91.5% to 67.5%) and proportionate increases in the use of thyroidectomy (p < 0.001), as previously described. 4 The percentage of responders changing their choice for primary treatment from ATD to thyroidectomy in the setting of active, moderate-to-severe TED was 20–40%, with Oceania being the region with the highest conversion rates from ATD to thyroidectomy (p < 0.001). Also, an increase in the use of radioiodine plus glucocorticoids prophylaxis (RAI + GC) was observed. The highest rates were in Asia and Latin America: increasing from 5–7.5% in the index case without TED to 10–15% use of RAI + GC in the presence of moderate-to-severe TED (p < 0.001). Finally, 1% of the respondents selected RAI without glucocorticoid prophylaxis. Figure 1 compares the management of hyperthyroidism in the presence or absence of TED, categorized by region. When comparing the treatment options for GD in patients with TED, although prolonged ATD remained the first choice in all regions, respondents from Europe, North America, and Oceania were more likely to recommend thyroidectomy than the other regions (p < 0.001) (Fig. 1). Respondents who see 6 to 15 newly diagnosed patients with GD per month were more likely to use ATD in patients with TED, compared to respondents with fewer than five new cases per month, who were more likely to use RAI with corticosteroid prophylaxis or thyroidectomy (p < 0.001). Respondents not associated with the Endocrine Society or thyroid societies (ATA, ETA, LATS, or AOTA) selected RAI + GC more frequently (p < 0.01) than did members of these organizations.
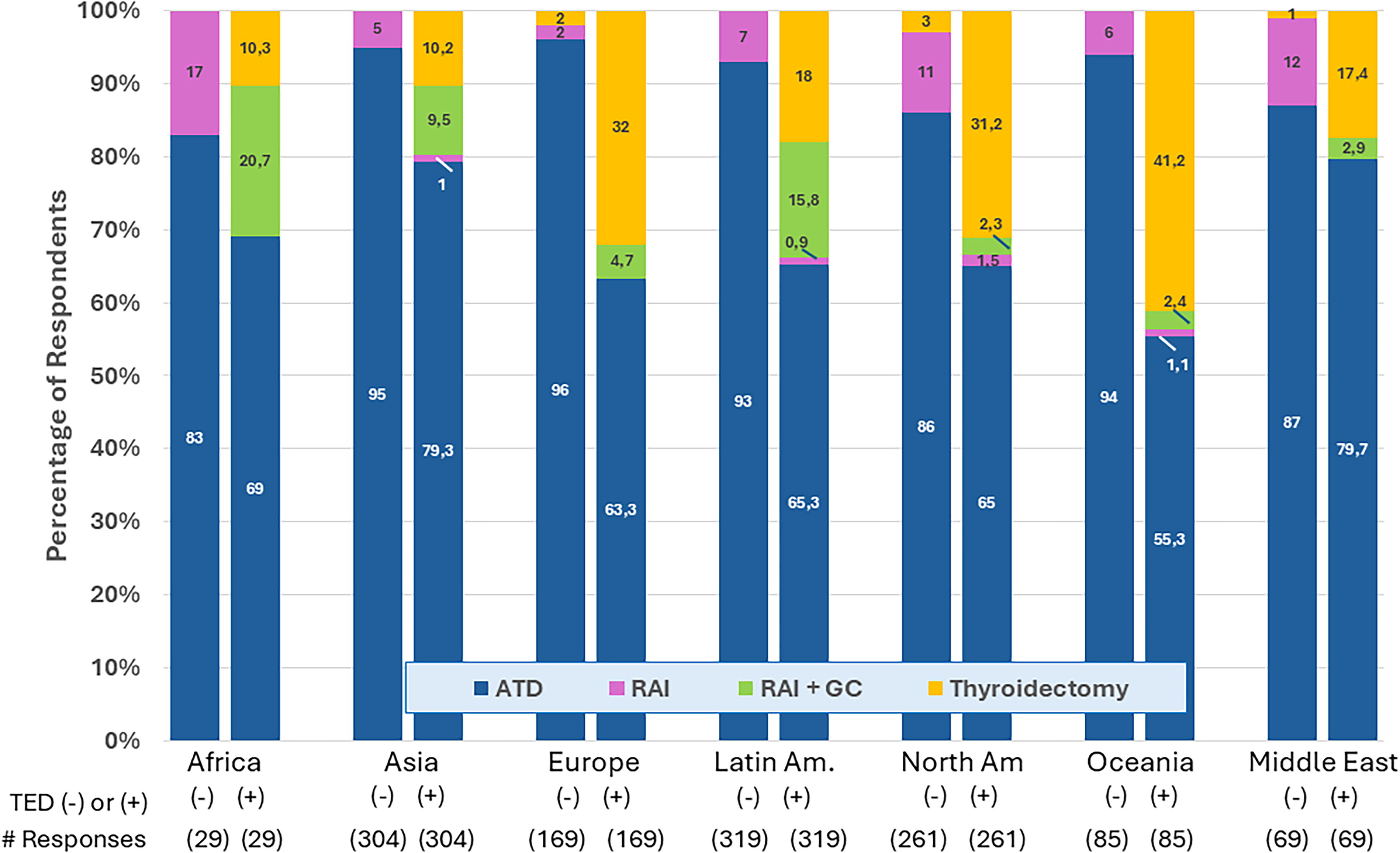
The effect of the presence of TED on the selection of primary therapy for hyperthyroidism due to Graves’ disease, by regional differences are shown, demonstrating the influence of the presence of thyroid eye disease on selection of therapy, by United Nations regions. TED, thyroid eye disease.
The impact of individual physician characteristics on management
Respondents who saw more than ten new GD patients per month were more likely to request visual field tests and diagnostic imaging (orbital CT or orbital MRI) (p < 0.005). Also, this same group of respondents prescribed more sodium selenite and glucocorticoids (p < 0.005 and p < 0.01, respectively) (Table S2 Supplementary Data). When stratified by age, respondents aged 66–80 compared to those 65 years or less were less likely to refer patients to an ophthalmologist, request visual or radiological exams, or prescribe sodium selenite or glucocorticoids (Table S3 Supplementary Data). Female respondents were more apt than their male counterparts to refer patients to ophthalmologists with experience in TED and request diagnostic testing (visual field testing, radiological exams) (p < 0.05). There was no interaction between age and sex.
Table 4 compares key survey findings to ATA-ETA Consensus Statement recommendations. 1,3 There are two sets of responses that are at odds with these recommendations: first, the use of RAI + GC, especially in Asia and Latin America in patients with moderate-to-severe TED, and second, the use of selenium by a majority of respondents from Europe and Oceania.
Comparison of Key Survey Findings to American Thyroid Association-European Thyroid Association Consensus Statement on the Management of TED
Reference for the American Thyroid Association-European Thyroid Association Consensus Statement on the Management of TED. 1
Discussion
The current study is a secondary analysis of a survey on the management of GD with more than 1400 respondents from 85 countries. 4 The analysis focuses on GD patients with TED, and includes members of 15 professional societies worldwide, with representation of endocrinologists and allied specialists from Latin America, Asia, Oceania, the Middle East, Africa, North America, and Europe. Most respondents would adhere to the recommended initial treatment measures for TED. In addition, most respondents would choose ATDs as first line of treatment of GD in the presence of TED. The survey revealed that the specialty most likely to supervise (or coordinate) advanced medical therapy for TED has changed dramatically over the past decade, and that regional differences exist. Specifically, an endocrinologist will likely be responsible for advanced medical management of TED in Europe, Asia, and Latin America, while an ophthalmologist will more often assume this role in North America and Oceania. This is a notable change from our 2011 survey of members belonging to three U.S.-based professional societies, which included 41% international members with primary practices outside of the U.S., at which time (pre-teprotumumab) 60.9% of respondents indicated that endocrinologists would be primarily responsible for TED care, 37.9% indicated a primary role for ophthalmologists, and <1% indicated primary care physicians coordinate TED care at their center. 6 This practice pattern change may relate to new regional differences in specialized training for TED management among ophthalmologists and endocrinologists. It may also reflect a marketing decision from the pharmaceutical industry, specifically targeting ophthalmologists due to their larger numbers of providers. 7 Recent clinical practice guidelines and consensus statements 1,3 include initial management, such as advice to quit smoking and using lubricating eye drops and more than 80% of survey respondents adhere to these recommendations. Also, most respondents indicated that they would order currently recommended diagnostic testing, such as visual field testing and radiological examinations, with no differences among geographic regions.
One remarkable survey result relates to the recommendation to use selenium, which was much more common among respondents from Europe and Oceania (60–65%) than from other regions. North and Latin American respondents were the least likely to recommend the use of selenium (30–35%). Since selenium deficiency has been shown to be a risk factor for the development of Hashimoto’s thyroiditis, supplementation has been proposed to be of value in patients with autoimmune thyroid disease, 8 including thyroid eye disease. 9 In a recent meta-analysis four randomized placebo-controlled trials evaluating the efficacy of selenium in TED, selenium was more effective at 6 and 12 months than placebo at lowering the Clinical Activity Score, but there was no difference in the degree of proptosis, soft tissue involvement, or ocular motility. 10 The four studies cited in the meta-analysis were conducted in Europe (the Netherlands, Italy, Switzerland, Greece, and Germany), Mexico, Thailand, and China. Each of these countries are considered to be mildly or moderately selenium deficient. 11,12 On the other hand, the United States, Canada, and many other countries around the world are selenium sufficient, and it is uncertain whether the potentially beneficial effects of selenium would be found in studies from these areas of the world. Although European respondents had higher rates of use of selenium, the European Group on Graves’ Orbitopathy (EUGOGO) guidelines do not advise a 6-month course in patients like the one presented in our survey, but rather advocate its use for mild GO. 3 A previous survey with 227 participants from North America and Europe also demonstrated higher rates of selenium recommendation for TED patients by European respondents (73% vs. 32%). 13 The use of systemic glucocorticoids also varied among regions. For example, based on these data, the same patient had twice the chance of receiving glucocorticoids in Asia (79%) than in Oceania (36%).
At the time of the survey, teprotumumab was only available in the United States and 42% of North American respondents opted for it. This could reflect a change in treatment in patients with TED, since North American responders chose teprotumumab more than twice as frequently as glucocorticoids. These results are similar to those of a previous study of ATA and ETA members. 13 At the time of this writing, teprotumumab is available in the USA, some countries in Latin America, and a single Middle Eastern country.
When comparing the answers of survey respondents regarding management of a Graves’ patient with TED to one without TED, there was an increase in the use of thyroidectomy as primary therapy. The shift in favor of thyroidectomy from ATD therapy might be explained by the fact that TRAb levels fall after thyroidectomy. 14,15 However, since TRAb levels also decline with ATD use, 14 there are probably other reasons for this shift in the choice of therapy that remain unclear. For example, some respondents may have been under the impression that thyroidectomy has a beneficial effect on TED compared to ATD therapy, but this is not evidence-based. Another reason for the increase in thyroidectomy could be the diffuse goiter presented in the TED case, which was approximately two to three times the normal size. The presence of a large goiter is a risk factor for failing to achieve remission with ATD therapy. 16
Noncompliance with current professional society guidance regarding the use of radioiodine with or without glucocorticoids in patients with hyperthyroidism due to GD and moderate-severe TED was noted in our study. Specifically, the switch from ATDs in uncomplicated GD to the use of RAI + GC in the presence of moderate-to-severe TED was selected by 8.6% of the respondents. Current professional ATA and ETA guidance advises against the use of RAI + GC in moderate-to-severe TED 1,17 since randomized controlled trials showing efficacy of this approach specifically excluded patients with this degree of disease severity. 18 This apparently inappropriate selection of RAI + GC, while decreased in frequency from our previous survey, 6 in which 16.9% of respondents made this selection, may be due to several contributing factors, including less experience treating TED patients. In fact, respondents who selected this modality of treatment usually see fewer new patients with Graves’ disease per month compared to respondents who selected ATD. In addition, respondents who selected RAI + GC were less like to be associated with the Endocrine Society or global thyroid societies (ATA, ETA, LATS or AOTA). Also, there may have been a lack of familiarity with recent guidance and/or difficulty recognizing the TED case presented as having active moderate-to-severe TED. According to the ATA/ETA consensus statement and EUGOGO guidelines, oral prednisone/prednisolone prophylaxis should be given if RAI therapy is selected in patients with mild TED or those at risk of de novo development of TED. 19,20
Regarding the initial general management of TED, smoking cessation and lubricant eye drops were not selected by 13% and 21% of respondents, respectively. Additionally, 1% of the respondents would choose RAI therapy without GC for the patient presented, even in the presence of moderate-to-severe TED. It is unclear from a demographic perspective that why some respondents failed to select common measures of TED care, such as lubricating eye drops or smoking cessation. However, it may be that these aspects of care are provided through primary care or ophthalmology in these respondents’ practice locations. Furthermore, these respondents see fewer patients per month (p < 0.001) and were less likely to be affiliated with professional societies (p < 0.001).
The survey has some limitations as responses to questions about the management of patients reflect the “intention” of the respondent, while the actual behavior of the respondent in “the real world” remains unknown. Research wherein intention and actual behavior have both been assessed (also referred to as the “say-do gap”) is largely in the domain of the social sciences 21 and market research, 22 and there is a paucity of such studies in the medical literature. Also, it is important to note that these findings cannot be applied to Graves’ disease patients with different clinical characteristics from the patient we described in the survey.
Finally, it would be of interest to conduct a similar survey among ophthalmologists and oculoplastic surgeons to analyze and compare the results to those presented herein, to note potential differences in care between medical and surgical specialties.
Conclusion
The survey results suggest that, for the most part, endocrinologists are familiar with and follow current professional society guidance by employing the recommended diagnostic tools, treatments, and utilization of a multidisciplinary management approach. However, there were instances in which there were significant deviations from current recommendations. It is essential to consider regional differences when evaluating how professional societies will guide continuing medical education efforts to enhance adherence to current consensus statements and clinical practice guidelines.
Footnotes
Acknowledgment
We thank Haixia Guan, MD, PhD Department of Endocrinology, Guangdong Provincial People’s Hospital (Guangdong Academy of Medical Sciences), Southern Medical University), Guangzhou, Guangdong, China for assistance in dissemination of the survey in China.
Authors’ Contributions
D.V., D.S.C., and H.B.B.: Contributed equally to conceptualization and methodology. D.V.: Contributed to writing the original draft, and D.S.C. and H.B.B.: Reviewed and edited the final article.
Author Disclosure Statement
The views expressed in this article are those of the authors and do not reflect the official policy of the National Institutes of Health or the United States Government. One or more of the authors are employees of the U.S. Government. This work was prepared as part of our official duties. Title 17 U.S.C. 105 provides that the “Copyright protection under this title is not available for any work of the United States Government.” Title 17 U.S.C. 101 defines a U.S. Government work as a work prepared by an employee of the U.S. Government as part of that person’s official duties. We certify that all individuals who qualify as authors have been listed; each has participated in the conception and design of this work, the analysis of data (when applicable), the writing of the document, and/or the approval of the submission of this version; that the document represents valid work; that if we used information derived from another source, we obtained all necessary approvals to use it and made appropriate acknowledgements in the document, and that each takes public responsibility for it.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Data
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.