
Abstract
Background:
Rearrangements of the ALK gene are rare in medullary thyroid carcinoma (MTC), with limited data on the efficacy of ALK inhibitors in this context. Novel fusions, such as SPECC1L::ALK, have not been extensively studied.
Methods:
We present a case of a 33-year-old woman with metastatic MTC, in whom molecular profiling using next-generation sequencing (Archer FusionPlex®) identified a SPECC1L::ALK gene fusion. Treatment with the ALK inhibitor alectinib was initiated at 600 mg twice daily.
Results:
The patient demonstrated a dramatic partial to near-complete response after 6 days of treatment, as shown by positron emission tomography-computed tomography. At 6 weeks, a complete response was confirmed. Treatment was generally well tolerated, aside from grade 3 myalgia with elevated creatine phosphokinase, managed with temporary cessation and dose adjustment. As of the latest follow-up (8 months), the patient remains on alectinib with sustained complete response.
Conclusions:
This is the first report of a SPECC1L::ALK fusion in MTC. The dramatic response to alectinib highlights the importance of molecular profiling and suggests that ALK inhibitors may benefit patients with rare ALK fusions in thyroid cancers.
Introduction
Rearrangements involving the ALK gene have been identified in various solid tumors, including thyroid carcinomas. In papillary thyroid carcinomas (PTC), the prevalence is estimated at 0.8%, according to The Cancer Genome Atlas (TCGA) data. 1 In medullary thyroid carcinoma (MTC), the prevalence of ALK rearrangements is reported to be around 2%. 2 However, the clinical efficacy of ALK inhibitors in patients with tumors harboring novel fusion partners remains largely unexplored. 3 The most common fusion partner in thyroid carcinomas appears to be STRN. Currently, no specific treatment guidelines exist for thyroid cancers with ALK rearrangements. As a result, therapeutic approaches are modeled after those used for ALK-rearranged lung carcinomas, which account for 3–7% of cases. We present here a remarkable case of a patient with metastatic MTC harboring a SPECC1L::ALK fusion who exhibited an exceptional response to the ALK inhibitor alectinib.
Patient
A 33-year-old female was referred for evaluation of cervical adenopathy. The patient reported a recent unintentional weight loss of 5 kg over 1 month, along with a progressive, debilitating dry cough. Her medical history included an episode of acute psychosis, surgical resection of a borderline mucinous ovarian tumor, and active smoking with a cumulative 8-pack-year exposure. The family history was significant for congenital cardiomyopathy in her father and sister.
A chest computed tomography (CT) scan revealed numerous bilateral pulmonary nodules. A positron emission tomography-computed tomography (FDG PET-CT) scan identified multiple hypermetabolic bilateral mediastinal and hilar lymphadenopathy, extending along the bronchial tree, a right thyroid mass, and multiple sites of osseous metabolic activity (Fig. 1A–E). Brain magnetic resonance imaging revealed no evidence of metastases.
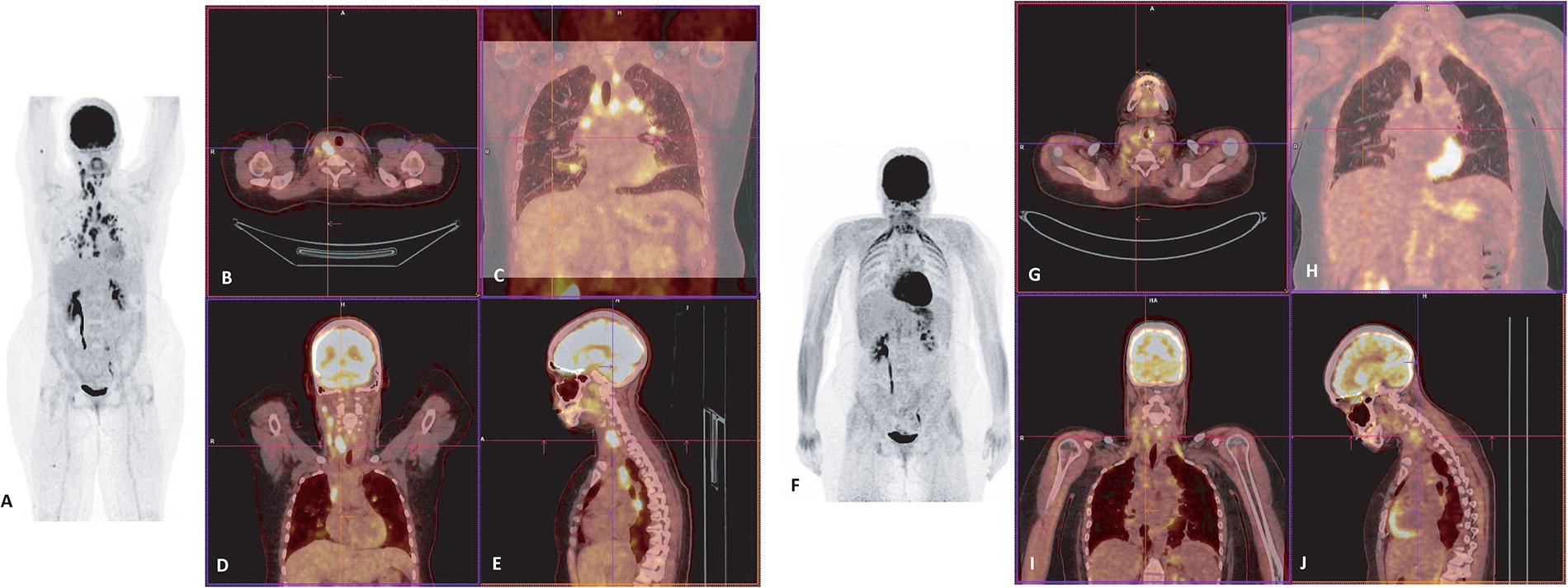
18F-FDG PET images with maximum grayscale projection before Alectinib therapy
Laboratory findings included an elevated serum calcitonin level of 209 pg/mL (normal <10 pg/mL), elevated carcinoembryonic antigen (CEA) at 17.8 pg/mL (normal <5 pg/mL), and elevated neuron-specific enolase at 50 pg/mL (normal <25 pg/mL). Thyroid ultrasonography showed a mass measuring 35 × 21 × 18 mm in the right lobe, associated with multiple ipsilateral cervical lymph nodes.
Histological analysis of biopsy specimens from the thyroid, cervical lymph node, and mediastinal lymph node (obtained via endobronchial ultrasound-guided biopsy) is presented in Figure 2 and demonstrates consistent tumor proliferation across all sites. The tumor was composed of medium-sized cells with eosinophilic cytoplasm and irregular nuclei, sometimes featuring nucleoli, arranged in lobules and clusters within a fibro-edematous and inflammatory stroma. Numerous mitotic figures were observed (12 mitoses per 1.7 mm2), along with areas of necrosis. Stromal amyloid deposition was not observed. Immunohistochemical studies showed diffuse positivity of tumor cells for chromogranin, synaptophysin, and TTF-1, with partial positivity for calcitonin (∼60–70% of tumor cells). PAX8 positivity was noted in a small number of nuclei. ALK immunohistochemistry was uniformly positive across all tumor cells, with retained Rb expression and wild-type p53. The Ki-67 proliferation index ranged from 35% to 60%, depending on the biopsy site. These findings led to the diagnosis of a high-grade MTC, according to the International Medullary Thyroid Carcinoma Grading System (IMTCGS). No gene mutation (including the RET gene) was detected by next-generation sequencing (NGS) assays covering 52 related cancer genes. But fusion transcript analysis (Archer FusionPlex® Lung, ArcherDx®) identified a novel SPECC1L::ALK gene fusion transcript (S12::A20, breakpoint: chr22:24759312, chr2:29446394; GRCh37/hg19 reference sequence). This chimeric transcript retains a long coiled-coil domain belonging to SPECCL1 and the tyrosine kinase domain of ALK, which could result in constitutive kinase activity and oncogenic transformation.
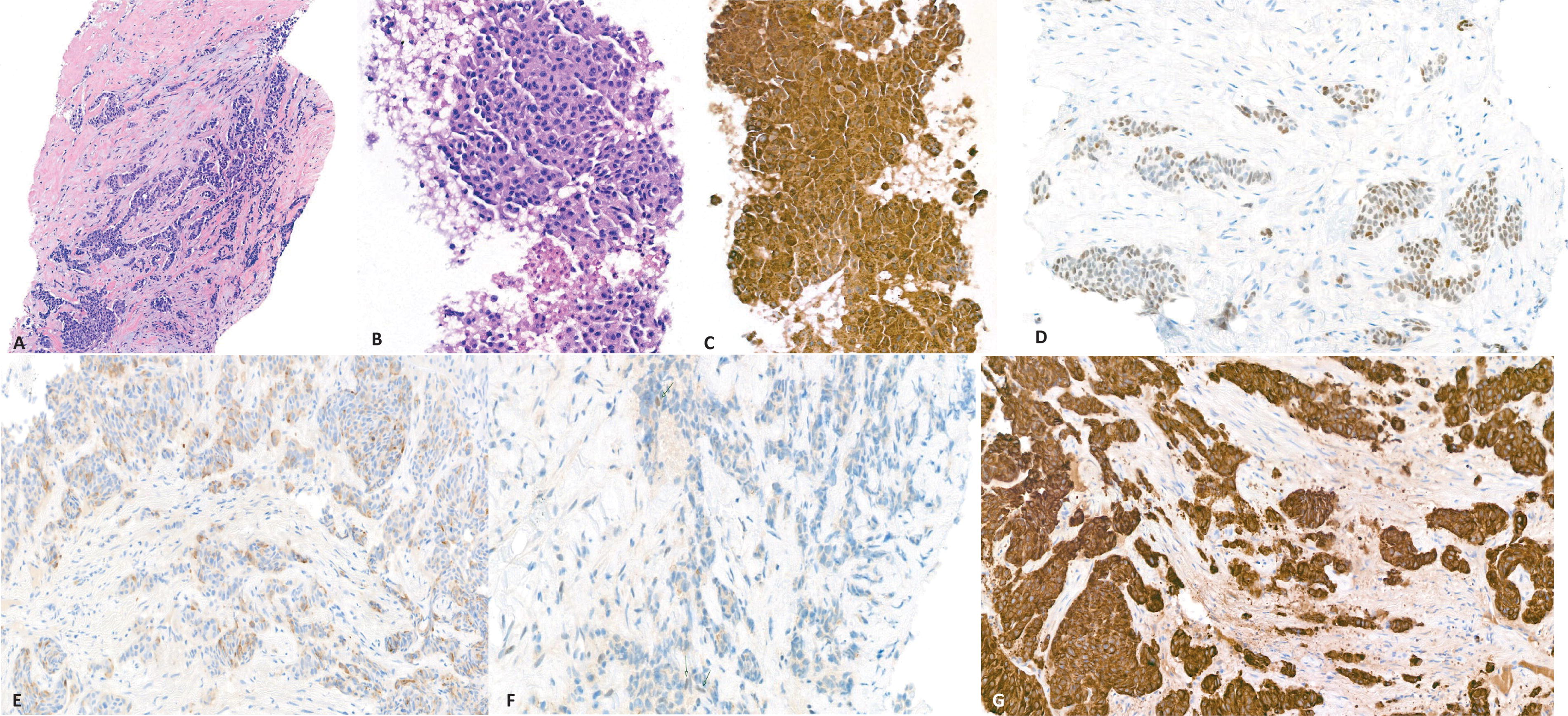
Biopsy specimens from the thyroid
Following a multidisciplinary discussion and obtaining informed consent, the patient was initiated on alectinib at a dose of 600 mg twice daily. A FDG PET-CT performed 6 days after starting treatment (as baseline for comparison with subsequent assessments) revealed a deep morphological and metabolic partial response in all lesions (Fig. 1F–J). A follow-up FDG PET-CT 6 weeks later confirmed a complete morphological and metabolic response. Laboratory assays also confirmed a decrease in serum calcitonin to <3 pg/mL and a reduction in CEA to 5.8 pg/mL (normal <5 pg/mL).
The patient tolerated the treatment well, though she developed myalgia with grade 3 elevations in creatine phosphokinase levels (>10 times the upper limit of normal). These adverse effects were managed with temporary cessation of treatment and dose adjustment. At the time of writing, the patient has remained on alectinib for 8 months. The follow-up duration remains limited, and longer-term monitoring is necessary to confirm the durability of the response and the long-term benefit of alectinib in this patient.
Discussion
The somatic genetic landscape of MTC remains incompletely understood, though it is most commonly associated with mutations in the RET gene. 4 Recent consensus guidelines from the American Head and Neck Society and the International Thyroid Oncology Group (ANHS-ITOG) recommend comprehensive somatic profiling in advanced MTC, particularly in the absence of germline RET mutations. 5 RET is the most commonly mutated gene in MTC, but somatic RAS mutations are frequent in RET-wildtype sporadic tumors, although they are not currently considered actionable targets for therapy. Moreover, there is no clear consensus regarding the routine inclusion of RAS testing in advanced MTC, as reflected by the lack of agreement among experts in recent ANHS-ITOG guidelines. 5 In rare cases, such as the one described here, other oncogenic drivers such as ALK fusions may be present. These guidelines emphasize the utility of NGS panels that include fusion detection, ideally using RNA-based assays. Similarly, the National Comprehensive Cancer Network (NCCN) Guidelines now recommend molecular testing for actionable alterations such as RET, ALK, NTRK, and BRAF, as well as biomarkers such as Microsatellite Instability (MSI) and Tumor Mutational Burden (TMB) in metastatic MTC. 6 This supports a broader, systematic approach to molecular testing that can guide both treatment decisions and genetic counseling for patients and families.
The introduction of ALK tyrosine kinase inhibitors (TKIs) has revolutionized the treatment of patients with metastatic ALK-rearranged non-small cell lung cancer (NSCLC). The PROFILE-1014 trial demonstrated that crizotinib significantly improves survival compared with chemotherapy, despite patient crossover. 7 Second- and third-generation ALK inhibitors, such as alectinib, have shown efficacy in overcoming resistance to crizotinib and in controlling brain metastases.
The most common ALK fusion partner is echinoderm microtubule-associated protein-like 4 (EML4), 8 but numerous other fusion partners have been described, often without sufficient clinical data. 9 In NSCLC, ALK rearrangements act as oncogenic drivers. Dickson et al. were the first to describe a novel SPECC1L::ALK fusion in 2018, identified in a case of epithelioid fibrous histiocytoma. 10 Since then, additional cases of SPECC1L::ALK fusions have been identified, including in lung cancer, where different exons and breakpoints of SPECC1L are fused with the ALK tyrosine kinase domain (exons 20–29). Several case reports have described responses to ALK inhibitors in NSCLC harboring SPECC1L::ALK fusions, with varying fusion breakpoints.
The somatic genetic landscape of MTC remains incompletely understood, though it is most commonly associated with mutations in the RET gene. 4 Ji et al. performed a screening of 98 cases of MTC, identifying two ALK-positive cases by FISH. 2 Targeted sequencing revealed a GFPT1::ALK (G13::A23) fusion in one case and an EML4::ALK fusion in the other, with the latter showing a dramatic response to crizotinib in the PROFILE-1013 phase 1b trial. Hillier et al. described a case of a 10-year-old boy diagnosed with MTC harboring a CCDC6::ALK fusion, who exhibited a striking response to crizotinib followed by alectinib for improved tolerability. 11
Responses to ALK inhibitors have been documented in other subtypes of thyroid cancers. Aydermirli et al. reported a case of metastatic PTC with an EML4::ALK fusion, where the patient initially experienced stable disease for 6 months, followed by a partial response to lorlatinib, including intracranial activity. 12 Similarly, Zhu et al. described a case of PTC with an STRN::ALK fusion, in which treatment with alectinib resulted in a partial systemic and cerebral response, ongoing for 8 months at the time of publication. 13 In a recent study, Buriolla et al. reported the first European case of an advanced PTC with STRN::ALK fusion successfully treated with alectinib, resulting in a complete radiological response and clinical benefit after 17 months of therapy. 14 De Salins et al. also reported a complete response to crizotinib in a 76-year-old woman with metastatic oncocytic thyroid carcinoma. 15
In the present case, there was initial diagnostic uncertainty regarding whether the primary tumor originated in the lungs or thyroid. Heterogeneous and typically faint calcitonin immunohistochemical positivity has been reported in a few extra-thyroidal tumors, including pulmonary carcinoid tumors and laryngeal neuroendocrine tumors, both of which may also express TTF1. 16,17 This overlapping expression can represent a significant diagnostic pitfall. However, the clinical and biological presentation, characterized by a thyroid mass with satellite lymphadenopathy and elevated serum tumor markers, supported the diagnosis of MTC. In this context, the Ki-67 proliferation index observed in our case is unusually high and would correspond to a neuroendocrine tumor (NET) G3 according to the current WHO G1–G3 grading system for gastroenteropancreatic NETs. 18 While MTC typically displays low to moderate proliferative activity, rare cases of high-grade MTC with markedly elevated Ki-67 indices have been described, often correlating with aggressive clinical behavior and extensive metastatic disease, 19 as seen in our patient. Notably, the Ki-67 index increased from 35% in the thyroid tumor to 60% in the mediastinal lymph node metastasis, suggesting tumor progression and biological heterogeneity.
The presence of a rare SPECC1L::ALK fusion, confirmed by immunohistochemical overexpression of ALK, was consistent with the diagnosis, although this fusion has rarely been observed in MTC. 2 The choice of alectinib over another ALK inhibitor was made based on a compromise between efficacy compared with crizotinib and tolerance compared with other ALK inhibitors. While the response observed supports the clinical relevance of the SPECC1L::ALK fusion, in the absence of functional validation or comparison with non-selective TKIs, it remains uncertain whether the benefit can be attributed solely to ALK inhibition. Furthermore, although the structure of the fusion suggests preserved kinase activity, no functional studies were performed to confirm its oncogenic potential, which remains a limitation of this report. The short follow-up duration limits our ability to assess the long-term efficacy and durability of the response to alectinib in this case.
The application of molecular profiling has transformed the management of rare tumors by uncovering unique genomic alterations that drive oncogenesis, such as the SPECC1L::ALK fusion identified in this case. The ability to detect such fusions, which are not traditionally associated with certain tumor types like MTC, illustrates the power of NGS to reveal actionable mutations in even the most unexpected contexts.
In this case, the discovery of the SPECC1L::ALK fusion allowed for the successful use of alectinib, a drug initially developed for ALK-positive lung cancers, highlighting the relevance of molecular diagnostics in guiding treatment choices. Without comprehensive molecular profiling, this rare fusion would likely have gone undetected, and the patient might have been subjected to less effective treatment options.
While the efficacy of ALK inhibitors is well established in ALK-rearranged lung cancers (3–7% of cases), this case demonstrates the broader potential of these therapies in other tumor types when guided by molecular alterations. The identification of fusions such as SPECC1L::ALK in rare tumors not only offers therapeutic options but also challenges the traditional organ-specific approach to cancer treatment, pushing toward a genomically-driven, tissue-agnostic model of care.
Yet, while NGS opens up the possibility of treating tumors based on their molecular profile, access to these therapies remains limited. Many drugs are approved only for specific cancers, making it difficult for patients with rarer tumors to benefit from them outside of clinical trials or compassionate use programs. Adding to the challenge is the low frequency of actionable mutations in rare tumors, which requires testing large cohorts of patients—a resource-intensive process. Tissue-agnostic clinical trials have been proposed, though recruitment remains a significant challenge. 20
The successful use of ALK inhibitors in this patient suggests that even in rare tumors, molecular profiling should be a standard component of diagnostic evaluation. As more tissue-agnostic approvals are granted by regulatory bodies, the utility of NGS will continue to expand, offering a personalized therapeutic approach that can improve outcomes for patients with rare and challenging cancers. Increasing evidence suggests that ALK rearrangements, though extremely rare (<0.2%), are found in a variety of non-NSCLC tumors, with response rates ranging from 50% to 85% and prolonged response durations. 21 These findings highlight the imperative need for further research into tissue-agnostic therapeutic strategies targeting ALK fusions, particularly in rare tumor types such as MTC, where clinical evidence remains scarce.
Conclusion
The use of ALK inhibitors has significantly improved outcomes for patients with ALK-rearranged malignancies, particularly in NSCLC. The rarity of ALK fusions in MTC presents diagnostic and therapeutic challenges. In this report, we document the first known case of a SPECC1L::ALK fusion in MTC, with a near-complete response to alectinib within 6 days of treatment initiation. This remarkable outcome underscores the importance of molecular profiling in rare tumors, particularly in younger patients, and suggests that ALK inhibitors could offer substantial clinical benefit across a broader range of ALK-rearranged cancers. Future studies and case reports are needed to further elucidate the clinical significance of SPECC1L::ALK fusions and the potential role of ALK-targeted therapies in these rare tumors.
Footnotes
Authors’ Contributions
H.B.: Conceptualization and writing—original draft. A.F.: Writing—original draft, investigation, and visualization. F.M.-B.: Resources, writing—original draft, and writing—review and editing. O.S.: Investigation, visualization, and writing—review and editing. P.D.: Resources and writing—review and editing. D.R.: Investigation and writing—review and editing. V.R.: Investigation and writing–review and editing. A.-C.V.: Investigation and writing—review and editing. L.B.: Resources, supervision, and writing—review and editing.
All authors reviewed and approved the final version of the article and agree to be accountable for all aspects of the work in ensuring the accuracy and integrity of the content.
Author Disclosure Statement
The authors declare no conflicts of interest in relation to the publication of this article.
Funding Information
The authors declare that no funding was received for the preparation or publication of this article.