
Abstract
Background:
Although accumulated experience with lenvatinib in patients with differentiated thyroid cancer (DTC) and progressive radioactive iodine (RAI)-refractory disease has been used to improve management strategies for this disease, findings regarding the actual clinical picture and long-term observation data are insufficient.
Methods:
We conducted a retrospective cohort study of patients with DTC who received lenvatinib treatment from 2011 to 2022 at the National Cancer Center Hospital East, Japan. The patients were treated under the following treatment and management policies (1) starting dose at 24 mg/day, (2) schedule modification according to individual adverse events status (planned drug holidays), (3) dose escalation of lenvatinib, and (4) local therapy at disease progression, if applicable. This is a retrospective cohort study, although some patients were enrolled in a prospective clinical trial (NCT01321554 and UMIN000022243).
Results:
Of 91 patients, 59 (64.8%) had papillary carcinoma and 22 (24.2%) had follicular carcinoma. Best overall response in all patients was 60.4% (partial response in 55 and complete response in 0). With a median observation period of 2.9 years (range, 0.1–12.4; interquartile range, 1.7–4.6) under supportive management, including the planned drug holidays (n = 72, 79.1%), dose escalation of lenvatinib at systemic disease progression (n = 21, 23.1%), and local therapy for oligoprogressive disease (n = 11, 12.1%), median progression-free survival and overall survival were 2.4 years (95% confidence interval [CI] 1.9–3.3) and 5.1 years (95% CI 3.3–6.7), respectively. At the time of data cutoff, 19.8% had discontinued lenvatinib treatment due to adverse events, although no adverse event was grade 5.
Conclusions:
In patients with RAI-refractory DTC treated with lenvatinib, careful treatment optimization and management of adverse events contribute to a favorable, durable prognosis.
Introduction
Differentiated thyroid cancer (DTC) accounts for 90% of all thyroid cancers. The treatment of locally recurrent, advanced, and/or metastatic disease not amenable to radioactive iodine (RAI) treatment is systemic therapy consisting of multi-kinase inhibitors (MKIs) and targeted therapy driven by treatable genomic alterations. Worldwide approval of these drugs is now relatively longstanding—10 years for MKIs and several years for targeted therapy—and many patients with RAI-refractory DTC have now benefited from them.
Lenvatinib is listed as the preferred category 1 drug in the National Comprehensive Cancer Network (NCCN) guidelines and European Society for Medical Oncology guidelines for patients with locally recurrent or metastatic progressive RAI-refractory DTC. 1,2 This recommendation is based on the results of the phase 3, randomized, double-blind, placebo-controlled SELECT trial, 3 in which the lenvatinib group demonstrated statistically significantly longer progression-free survival (PFS) than the placebo group (median PFS, 18.3 months vs. 3.6 months; hazard ratio [HR], 0.21; 99% confidence interval [CI], 0.14–0.31; log-rank p-value <0.001) and a higher overall response rate (ORR) (64.8% vs. 1.5%; odds ratio, 28.87; p-value <0.001). Accordingly, lenvatinib is now recognized as a key drug for RAI-refractory DTC.
Disease treatment and management with lenvatinib have been refined by several post hoc analyses of the SELECT trial and a number of prospective and retrospective studies. 4 –6 We have also provided several reports on treatment strategies and management. 7 –12 Our management policy includes an appropriate starting dose (24 mg/day), planned drug holidays to avoid severe adverse effects, and dose escalation to re-establish the efficacy of lenvatinib. We believe these approaches help improve the prognosis of patients with DTC by maximizing anti-tumor efficacy with safety.
Several other retrospective studies have reported the results of lenvatinib in long-term clinical use. However, these studies are limited by heterogeneous treatment, inadequate management of adverse events, and short observation periods. 13 –20 The lack of robust long-term results of lenvatinib often hinders treatment decision-making for both oncologists and patients.
Here, we aimed to clarify long-term clinical outcomes for lenvatinib in patients with DTC treated with currently available optimized management.
Materials and Methods
Patients
This single-center retrospective cohort study was approved by the Institutional Review Board of the National Cancer Center Hospital East, Japan (2016-243). Patients with thyroid cancer who were introduced to treatment with lenvatinib from September 2011 to November 2022 were reviewed. The inclusion criteria were as follows: (1) locally recurrent or metastatic, progressive, RAI-refractory disease; and (2) histologically proven papillary thyroid cancer (PTC), follicular thyroid cancer (FTC), or poorly differentiated thyroid cancer (PDTC). Patients with brain metastasis were required to undergo pre-treatment with external radiotherapy. Our study allowed the inclusion of patients who were previously enrolled in clinical trials (NCT01321554 and UMIN000022243). Written informed consent for lenvatinib therapy was obtained from each patient, including an explanation of the potential modification of the treatment schedule and drug dose in consideration of adverse events. In accordance with national legislation and the institutional ethics board, written informed consent for study participation was not required. However, detailed information regarding the study’s purpose, methods, and anticipated outcomes was made publicly available on the ethics review board’s website. In addition, patients were given the opportunity to opt out of the use of their data in the study in accordance with institutional policy.
Treatment
The initial dose of lenvatinib was 24 mg/day for all patients. Dose reductions and interruptions were performed in accordance with adverse events in each patient. Our clinical practice includes a planned drug holiday strategy, summarized as an interruption within the period of previous adverse events, to maintain dose intensity and avoid severe or intolerable toxicities. 7,10,12 At the time of disease progression on lenvatinib treatment, various treatment choices are considered to maximize the survival benefit from lenvatinib, if available and reasonable. Dose escalation was endorsed after disease progression to regain anti-tumor efficacy, 11 and palliative local therapy, including surgery and radiation, was also permitted for oligoprogressive disease. Other supportive treatments, such as extra visits, medication for adverse events, and self-care education by multi-disciplinary staff, were provided for all patients as usual clinical practice. Details of our treatment strategy and management are provided elsewhere. 9
Evaluation and statistical analysis
Clinical tumor response to treatment was evaluated radiographically according to Response Evaluation Criteria in Solid Tumors ver. 1.1 using computed tomography (CT), which was evaluated every 3 to 6 months. ORR was defined as the proportion of patients with a complete response (CR) or partial response (PR) to lenvatinib therapy. Disease control rate (DCR) was similarly defined as the proportion of patients with a CR, PR, or stable disease (SD). Clinical benefit rate (CBR) was defined as the proportion of patients who achieved a CR, PR, or durable SD persisting for at least 23 weeks. Overall survival (OS), PFS, and duration of treatment (DOT) were calculated using the Kaplan-Meier method. OS was calculated from the introduction of lenvatinib until death from any cause. PFS was calculated from the introduction of lenvatinib until first disease progression or death from any cause. DOT was calculated from the introduction to discontinuation of lenvatinib treatment for any reason, including continuous progression of disease, treatment toxicity, and death from any cause. Patients who were lost to follow-up were censored at the date of last follow-up. Adverse events were evaluated by Common Terminology Criteria for Adverse Events version 4.0. All statistical analyses were performed with EZR (version.1.51; Saitama Medical Center, Jichi Medical University, Saitama, Japan). The cutoff date was November 7, 2024.
Results
Patient and tumor characteristics
Ninety-one patients were identified. A participant flow diagram is shown in Figure 1. Patient and tumor characteristics at the introduction of lenvatinib are shown in Table 1. Median age was 70 years (range, 42–84), and all patients had an Eastern Cooperative Oncology Group performance status of 0 or 1. By histological subtype, PTC, FTC, and PDTC accounted for 59 (64.8%), 22 (24.2%), and 10 (11.0%) cases, respectively. Regarding metastases, lung metastases occurred in 75.8%, lymph node metastases in 62.6%, and bone metastases in 35.1%, with some overlap among individuals. Most patients (93.4%) had no prior systemic therapy, but a few patients were previously treated with MKI (3.3%), BRAF targeted therapy (1.1%), immune checkpoint inhibitors (1.1%), and cytotoxic chemotherapy (1.1%). Genomic testing after lenvatinib treatment was performed for 26 patients (21 patients with PTC, 2 with FTC, and 2 with PDTC). Genomic alteration was identified in 23 of 26 patients: 19 patients (20.1%) had BRAF-mutated disease (BRAFV600E mutation), 3 patients (3.3%) had RAS family-mutated disease (HRAS A182G, KRAS G12A, and NRAS Q61R), and 1 patient (1.1%) had RET-fusion (RET-CCDC3 fusion)-positive disease.
Participant flow diagram.
Patient and Tumor Characteristics at Initiation of Lenvatinib
Some cases with duplication.
BRAF plus MEK inhibitor, combination treatment with a v-raf murine sarcoma viral oncogene homolog B1 inhibitor and mitogen-activated protein kinase kinase enzyme inhibitor; ECOG PS, Eastern Cooperative Oncology Group performance status; RAI, radioactive iodine.
Treatment status and disease management
The details of the treatment status and disease management approach are shown in Table 2. At the cutoff date, 17 (18.7%) patients had continued lenvatinib treatment, 46 (50.5%) had discontinued lenvatinib due to disease progression, 18 (19.8%) had discontinued lenvatinib due to adverse events, and 10 (11.0%) patients were lost to follow-up, including those with relocation. The details of treatment management were as follows. During treatment with lenvatinib, the treatment schedule for 72 (79.1%) patients was conducted under the planned drug holiday strategy in accordance with the status of adverse events. At disease progression, dose escalation of lenvatinib was conducted in 21 (23.1%) patients, and palliative local therapy, including surgery and radiotherapy, was performed in 6 (6.6%) and 5 (5.5%) patients, respectively. After discontinuation of lenvatinib, 14 (15.4%) patients received other systemic treatments, including BRAF plus MEK inhibitor and RET inhibitor (Table 2).
Treatment Status
aSome cases with duplication.
RET inhibitor, rearranged during transfection.
Anti-tumor efficacy and prognosis
Table 3 shows anti-tumor efficacy. Best overall response was PR in 55 (60.4%) patients; SD in 32 (35.2%), including 23 (25.3%) with durable SD; and PD in 4 (4.4%). No patient had CR. Accordingly, ORR, DCR, and CBR were 60.4%, 95.6%, and 90.1%, respectively.
Anti-Tumor Efficacy
All clinical tumor responses were evaluated by Response Evaluation Criteria in Solid Tumors (RECIST) ver. 1.1.
CR + PR + SD persisting for at least 23 weeks.
With a median observation period of 2.9 years (range, 0.1–12.4; interquartile range, 1.7–4.6), 65 PFS events, 64 DOT events, and 44 OS events were recognized. Kaplan-Meier curves for PFS, DOT, and OS are shown in Figure 2. Median PFS and 2-year PFS were 2.4 years (95% CI 1.9–3.3) and 57.2% (95% CI 46.0–66.8), respectively. Median DOT was 2.9 years (95% CI 2.0–3.3) and 2-year DOT was 59.9% (95% CI 49.1–69.3), resulting in a median OS of 5.1 years (95% CI 3.3–6.7) and 2-year OS of 79.4% (95% CI 69.4–86.5).
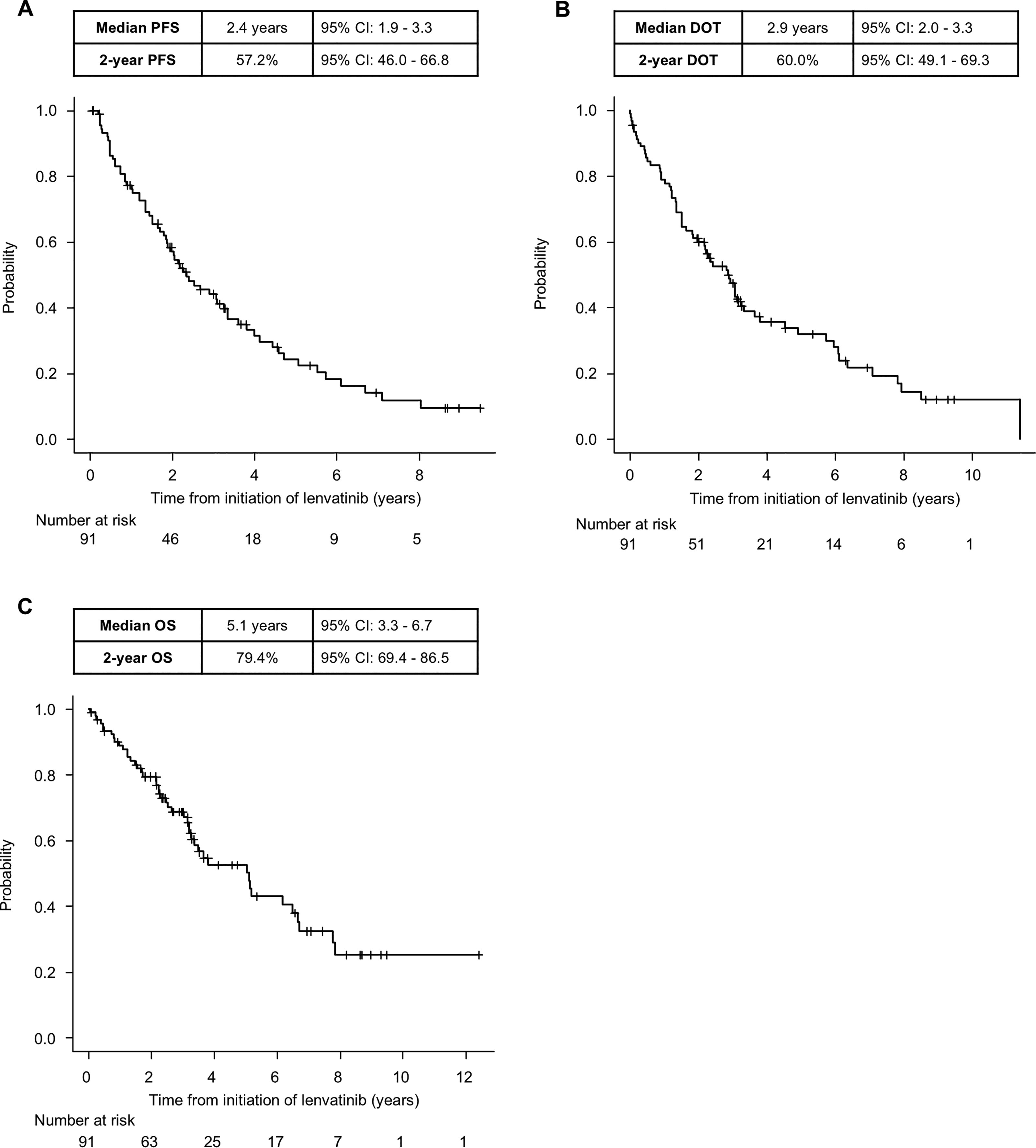
Kaplan-Meier curves of
Among the 10 patients who received targeted therapy after lenvatinib treatment, median PFS was 9.1 months (95% CI: 1.1–not applicable), and 8 patients achieved a PR. Median observation period was 9.2 months (range: 1.9–16.9; interquartile range: 4.4–9.3).
Safety
Table 4 shows all adverse events observed in the total population. The most common adverse events, excluding abnormal laboratory results, were hypertension (93.4%), palmar-plantar erythrodysesthesia syndrome (PPES) (61.5%), and anorexia (52.8%). There were no grade 5 adverse events. Table 5 summarizes adverse events leading to termination of lenvatinib treatment, including non-suspected treatment-related adverse events. A total of 18 patients discontinued lenvatinib due to adverse events, of whom 16 patients (88.9%) experienced grade 3 events and 2 patients (11.1%) experienced grade 2 events. The overall prognosis of these patients was generally poor. In particular, three patients with grade 3 esophageal perforation exhibited notably limited survival durations following the discontinuation of lenvatinib (2, 3, and 12 months, respectively). In contrast, two cases of intracranial ischemia were classified as grade 2, as the lesions were detected radiologically and managed conservatively with anticoagulation therapy and without the need for invasive interventions.
Summary of Adverse Events
All events were graded according to Common Toxicity Criteria for Adverse Events Version 4.0.
ALT, alanine aminotransferase; AST, aspartate aminotransferase.
Adverse Events Leading to Termination of Lenvatinib Treatment
All events were graded according to Common Toxicity Criteria for Adverse Events Version 4.0.
Discussion
In this study in patients with RAI-refractory DTC treated with lenvatinib, we demonstrated a median PFS of 2.4 years, a median DOT of 2.9 years, and a median OS of 5.1 years. The median observation period of 2.9 years (range, 0.1–12.4; interquartile range, 1.7–4.6) is the longest reported to date. At data cutoff, the incidence of discontinuation of lenvatinib due to any adverse event was 19.8%, although no grade 4 or 5 adverse events were reported. Of note, our study highlights the clinical significance and validity of specific management strategies, including planned drug holidays, dose escalation of lenvatinib at the time of systemic disease progression, and local therapy for oligoprogressive disease. These approaches were considered to contribute to the favorable prognosis observed.
Since its first approval in Japan in 2015, lenvatinib has played a pivotal role in the management of DTC. Several retrospective studies have reported real-world outcomes of lenvatinib for patients with DTC. 13 –19,21 However, early real-world reports, which would be expected to provide long-term follow-up prognostic data, might underestimate the efficacy of lenvatinib because they limited patients who were ineligible for clinical trials due to poorer characteristics, including performance status, pre-treatment history, or comorbidities. 14,20 Furthermore, the identification and evaluation of prognostic events in patients with DTC treated with MKI requires an extended observation period. Many articles in the literature, even late reports, had limited follow-up durations, potentially underestimating the full clinical activity of lenvatinib. Rendl et al. reported a 2-year PFS of 71% (95% CI 56–87) and 2-year OS of 74% (95% CI 60–88) with a median follow-up of 2.8 years, which was the longest, in 43 patients treated with lenvatinib. 17 Even in their study, however, 44% (19 of 43 patients) lacked an objective assessment of anti-tumor efficacy; rather, tumor assessment was performed mainly by F-18 fluorodeoxyglucose positron emission tomography/CT, which is not commonly used for thyroid cancer. Furthermore, the release of the long-term results of the SELECT trial has been insufficient, limiting evaluation of the actual clinical efficacy of this agent. From this viewpoint, our present results—obtained by long-term observation under widely accepted evaluation methods—represent a reliable benchmark, which reflects the actual clinical value of lenvatinib.
In addition, genomic medicine in thyroid cancer continues to show progress, and several molecular targeted agents have shown clinical utility (e.g., targeting BRAF, 22 RET, 23,24 NTRK 25,26 ). Despite this, the NCCN guidelines continue to rank lenvatinib as a “category 1” systemic therapy for RAI-refractory DTC, likely due to its reliable anti-tumor efficacy. 1 This recommendation, which does not mention the effect of genomic mutation, may rely on the results of the exploratory biomarker analyses in the SELECT trial, in which patients with BRAF mutation treated with lenvatinib also showed a greater benefit in PFS than those treated with placebo. Although the present and other supplementary studies may together support the selection of lenvatinib as first line treatment in this patient population, a further study examining the prioritization of treatment sequence (lenvatinib or BRAF-directed molecular targeted therapy) will provide clinically significant guidance. Moreover, a significant number of patients treated with lenvatinib do not have a potent therapeutic target. 27 The lack of an appropriate target particularly affects patients with FTC, giving them little opportunity to receive targeted therapy; 28 this situation also highlights the importance of lenvatinib.
We attribute the encouraging prognostic data in our study to several clinical factors. First, we started lenvatinib treatment at the dose of 24 mg/day. This dose was primarily selected in accordance with the results of a randomized study, which compared the standard dose and a reduced dose (18 mg/day), and found that the reduced starting dose sacrificed prognostic outcomes without ameliorating adverse events. 9 In this study, the ORR in the reduced starting dose group did not demonstrate non-inferiority to that in the standard group, namely 40.3% (95% CI 29.3–51.2) for 18 mg/day versus 57.3% (95% CI 46.1–68.5) for 24 mg/day, suggesting that a reduced starting dose adversely affected anti-tumor efficacy. Second, we adopted a planned drug holiday strategy in which lenvatinib treatment was intentionally interrupted according to the status of adverse events. 10,12 Our prospective observation and retrospective studies showed that this strategy potentially contributes to a better prognosis with a more favorable safety profile. 10,12 Of the 91 patients in this study, 10 were enrolled in the COLLECT study, a multicenter, prospective, observational study of lenvatinib. The COLLECT study delegated treatment management to the individual institutions, and management may have differed accordingly between them. However, the current study was conducted in a single center, likely allowing for a more standardized management approach. Our planned drug holiday strategy can be summarized as interrupting lenvatinib administration on the anticipated day of severe or intolerable adverse events based on each patient’s prior clinical course. Such proactive toxicity management has the potential to support sustained treatment continuation and optimize the therapeutic efficacy of lenvatinib. At the same time, clinicians should be cautious not to overlook low-grade adverse events, as we have found that even mild toxicities may rapidly worsen and lead to unexpected treatment interruptions. Therefore, a more preemptive strategy—specifically, the implementation of a fixed, intentional schedule of planned drug holidays—may represent a practical approach to completely preventing the emergence of undesirable or intolerable adverse events, and this concept also warrants prospective validation in future studies. Third, we considered the dose escalation of lenvatinib at disease progression to maximize clinical benefit in reference to a report that first advocated this strategy in renal cancer patients treated with axitinib. 11,29 The escalated dose of lenvatinib is carefully determined based on previous adverse events status and the need to schedule dosing under the planned drug holiday strategy so as not to exceed the threshold associated with a high rate of intolerable adverse events. As a result of this approach, we rarely observed treatment discontinuation due to adverse events during dose escalation (7%; one case of pulmonary abscess among 15 patients). 11 We speculate that these individual management factors acted in complement to produce a numerically preferable result.
Our study had several limitations. First, in contrast to current treatment strategies in this field, we were unable to assess whether genomic (e.g., BRAF) status, which can be a prognostic and predictive factor in thyroid cancer, 30,31 affected efficacy results due to the limited opportunity to analyze them. In relation to this, we have yet to conclude whether the current results with lenvatinib will be retained following genomic alteration-targeted therapy. Second, because of the retrospective nature of the study, we might have overlooked adverse events, particularly low-grade events. Further, we need to assess the characteristics of adverse events under the specific management introduced in the current study. In our previous study, the planned drug holiday strategy appeared to reduce the frequency of unplanned drug interruptions due to several adverse events when compared with conventional daily administration (fatigue/malaise: 52.3% vs. 4.0%, p-value <0.001; diarrhea: 38.0% vs. 8.0%, p-value = 0.028; thrombocytopenia: 19.0% vs. 0%, p-value = 0.037). 10 In contrast, PPES was one of the leading adverse events associated with temporary treatment interruptions in both groups, albeit that frequency was slightly lower in the planned drug holidays group (28.0%) than in the daily administration group (33.3%). These findings suggest that planned drug holidays may be particularly beneficial for managing certain adverse events and preserving treatment adherence, whereas other adverse events—such as PPES—may require further ingenuity, such as both planned drug holidays and additional dose adjustment depending on severity. Regarding long-term specific adverse events, our study demonstrated that patients treated with a planned drug holiday strategy—who generally received lenvatinib for longer durations—had a higher incidence of grade 3/4 proteinuria (60%) than those on conventional continuous daily dosing (23.8%). Furthermore, renal dysfunction was more frequently observed in patients with coexisting diabetes mellitus, suggesting a possible interaction between comorbidities and prolonged lenvatinib exposure. Notably, the incidence of grade ≥3 proteinuria in both the planned drug holidays group (60%) and the current cohort (39.6%) was substantially higher than that reported in the SELECT trial (10%), supporting the association between this toxicity and extended treatment duration. Collectively, these findings suggest that certain adverse events—particularly proteinuria—may be associated with long-term lenvatinib exposure, especially in patients with specific comorbid conditions. A long-term prospective study is warranted to assess these adverse event characteristics accurately and to enhance the clinical value of the ingenuities introduced in the current study. Third, the results were obtained from a Japanese patient population, who are reportedly at high risk for adverse events 32 ; accordingly, it remains unclear whether our detailed management without excess and omission matching can be applied to generalized patients worldwide. Additionally, 85% of patients in the current study did not receive further systemic treatment after lenvatinib. One primary possible reason is that cabozantinib, which has shown efficacy in prolonging PFS in randomized controlled trials following lenvatinib or sorafenib, 33 has not been approved for use in Japan. Given this limitation in available treatment options and overcoming them, we have adopted lenvatinib dose-escalation therapy as an alternative strategy when clinically appropriate.
Conclusions
On long-term observation, lenvatinib demonstrated favorable and durable efficacy for patients with RAI-refractory DTC when managed appropriately. Our findings suggest that optimized treatment strategies—including personalized dosing schedules, planned drug holidays, dose escalation at progression, and targeted local therapy for oligoprogressive disease—alongside careful management of treatment-related adverse events are critical factors in achieving these positive outcomes. This approach allows patients to maintain treatment while minimizing toxicity, potentially extending the clinical benefit of lenvatinib therapy in this challenging disease setting.
Footnotes
Acknowledgments
The authors would like to thank all patients and their families for this study. Furthermore, the authors also thank Chihiro Matsuyama, Yuma Shibutani, and Shinya Suzuki (Department of Pharmacy, National Cancer Center Hospital East, Japan) for their clinical and research assistance. The authors thank Guy Harris, D.O. of Dmed (![]() ), for editing drafts of this article. However, the ultimate responsibility for opinions, conclusions, and data interpretation lies with the authors.
), for editing drafts of this article. However, the ultimate responsibility for opinions, conclusions, and data interpretation lies with the authors.
Authors’ Contributions
Conceptualization: R.O., T.E., and M.T. Methodology: All authors. Software: R.O. Formal analysis: R.O. Investigation: R.O. Writing—original draft: R.O. and T.E. Writing—review and editing: All authors. Project administration: T.E. Supervision: M.T.
Author Disclosure Statement
M.T. reports grants and personal fees from Ono Pharmaceutical and Bayer, and personal fees from MSD, BMS, Merck Biopharma, Pfizer, Rakuten Medical, Lilly, Boehringer Ingelheim, Eisai, Chugai Pharmaceutical, Daiichi-Sankyo, Janssen Pharmaceutical, Genmab, Astra Zeneca, Abbvie and Astellas outside the submitted work. T.E. reports personal fees from Ono Pharmaceutical, Bayer, MSD, and Merck Biopharma outside the submitted work. S.O. reports personal fees from Ono Pharmaceutical, MSD, BMS, and Merck Biopharma. Others declare no conflicts of interest.
Funding Information
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.