
Abstract
Background:
Newborn screening for congenital hypothyroidism (CH) has been implemented in high-income countries since the 1970s to prevent intellectual disability. A delayed thyrotropin (TSH) rise with a normal TSH on the first dry blood spot (DBS) sample, followed by an abnormal TSH on the subsequent DBS, is sometimes observed in preterm newborns. The incidence of permanent CH and the screening process in preterm newborns remain controversial. Our aim was to evaluate the incidence of transient and permanent CH and delayed TSH rise in preterm newborns. The utility of a multiple screening samples is discussed.
Methods:
We conducted a retrospective study on preterm newborns (<37 weeks of gestation) screened at the Newborn Screening Center of Université Libre de Bruxelles between January 2014 and December 2023. A literature review was performed to identify cases of permanent CH with delayed TSH rise in cohorts of preterm newborns.
Results:
Of the 3578 preterm newborns included in the study, 10 were diagnosed with CH (0.3%). The majority of CH cases were transient (6 out of 10 transient, one deceased and one under ongoing L-thyroxine, too young for weaning attempt). Six cases were detected at the first DBS, four at subsequent DBS. Only two cases were confirmed as permanent CH, yielding an incidence of 1 in 1789 for permanent CH in preterms (0.05%). One of the two had a delayed TSH rise. Genetic testing helped in establishing the diagnosis of permanent CH with gland in situ.
Conclusions:
Permanent CH appears to be rarer than transient CH among preterm newborns (1/1789 vs. 1/596). Transient CH may be suspected in case of iodine exposure or thyroid ultrasound showing an in situ gland with negative genetic testing and absent maternal blocking antibodies. In such cases, early L-thyroxine weaning may help avoid overtreatment. A delayed TSH rise leading to a false negative first DBS is not uncommon in preterm newborns with permanent CH. This justifies a second DBS in preterms. Given the retrospective nature of this study, these findings should be interpreted with caution, and further prospective research is warranted to confirm these observations.
Introduction
Newborn screening for primary congenital hypothyroidism (CH) has been implemented in high-income countries since the 1970s and has been shown to prevent intellectual disability. 1
While clear recommendations have recently been issued for CH screening in term newborns, 2 there is no clear consensus about the screening in preterm newborns: is a second (and a third) dried blood spot (DBS) necessary, what is the best timing of the second DBS, should the TSH cutoff be different for the second DBS. 3 –6
Indeed, immaturity of the thyrotrope axis has been reported in preterm newborns, characterized by a lower TSH peak on the first day of life. 7 Similar to term newborns, TSH peaks around 90 minutes after birth and then decreases until day 3; however, in some cases, especially in extremely preterms, it rises again after the 7th day of life. 8 Neonatal morbidity and certain medications can affect thyroid function in preterm newborns: dopamine and glucocorticoids suppress TSH secretion, while iodine and amiodarone can cause acquired hypothyroidism. 9 False negative screening results can occur in newborns requiring blood transfusion. 10 The degree of prematurity might also influence the TSH levels: neonates born with a gestational age (GA) between 30 and 35 weeks, have TSH values from 24 hours of life that are similar to those of term newborns. 11
Cases of CH with delayed TSH rise were first described in 2000 12 and have since been reported by several screening programs, especially in preterms and very low birth weight newborns. 12 –14 Delayed TSH rise in preterm newborns usually occurs at 2–6 weeks of life. It remains unclear whether these cases represent preterm newborns with transient or with permanent CH. 15 Nonetheless, many programs now perform repeated DBS testing to identify such cases. 5,6,16,17
Since the goal of CH screening is intellectual disability prevention, it is controversial whether treatment of newborns with mildly elevated TSH, on the first or the second DBS, is necessary. Some studies suggest that GA rather than TSH levels influences neurodevelopmental outcomes in preterm babies, 18 while others report that even a modest TSH elevation is associated with poorer neurodevelopmental outcomes. 19,20
In literature, the number of permanent versus transient CH and the number of delayed TSH rise among permanent CH cases is rarely clear. 4,14,21,22
This study aims to evaluate the incidence of transient and permanent CH in preterm newborns and the incidence of delayed TSH rise in this population over a 10-year period. In addition, we carried out a literature review centered on the identification of premature newborns with permanent CH with a delayed TSH rise (normal first DBS). The usefulness of multiple sampling in CH screening is discussed, based on our single-center experience and our literature review.
Material and Methods
The study was approved by the NBS program unit of the Fédération Wallonie Bruxelles and the local ethics committee (CEH No. 34/24). The research was conducted in accordance with the Declaration of Helsinki, as revised in 2013. The local ethics committee issued a statement confirming that informed patient/participant consent was not required due to the retrospective nature of the research project.
We included preterm newborns (<37 weeks of GA) screened by the Newborn Screening Center of Université Libre de Bruxelles between January 2014 and December 2023.
In Belgium, serial screening for preterms started in 2014 and was adopted by most neonatal centers in 2016, with a first screening between days 2 and 5, a second screening on day 14 and a third on day 30 or at discharge.
Neonates with only one DBS collected between 2 and 5 days of life and with TSH within the normal range were excluded. After anonymization, the following data were retrieved from the Université libre de Bruxelles’ Center database: number of preterm newborns screened, GA, twin status, sex, birth weight, whole blood TSH value, and age at DBS collection.
TSH was measured on DBS samples by time-resolved fluorimetry immune-assays (AutoDelfia until December 2018 and GSP Perkin Elmer since January 2019). The whole blood TSH cutoff value to request a second DBS sample was 15 mU/L until December 2018. Since January 2019 the 99.5th percentile, calculated from the healthy newborn population, which varied between 8.25 and 12.50 mU/L) has been used. This 99.5th centile is evaluated using the results obtained during the last 12 months and is adjusted every 3 months. A whole blood TSH cutoff value of 30 mU/L was used for urgent referral. The same cutoff applies regardless of the screening time point.
In preterms with positive screening results, serum TSH, free T4, and thyroglobulin levels were measured. Thyroid ultrasound and sodium pertechnetate scintigraphy were performed when feasible. Levothyroxine treatment was started when serum TSH was >20 mU/L.
Data concerning patients under levothyroxine treatment were retrieved from the medical records.
CH was considered to be permanent in patients with athyreosis or an ectopic thyroid and in patients with an in situ gland if TSH levels rose 6 weeks after treatment cessation or if a pathogenic variant was detected in the thyroid gene panel. Genomic DNA was extracted from peripheral blood leukocytes, and informed consent for genetic testing was obtained from the legal guardians. Sequencing of 4876 genes was performed using the SeqCap EZ Choice XL (NimbleGen) on a HiSeq1500 instrument (Illumina) at BRIGHT core (Brussels, Belgium). Variant filtering was performed with Highlander software. Pathogenicity was assessed using the Franklin tool (www.franklin.genoox.com).
Descriptive statistics were used to report frequencies, rates, and confidence intervals (CIs). No formal statistical comparisons or hypothesis testing were performed. Histograms were generated using R software (version 2022.12.0 + 353). There were no significant missing data in the variables analyzed.
We reviewed published cases of preterm newborns with permanent CH and a delayed TSH rise (normal first DBS with an abnormal subsequent DBS). Pubmed search terms included: “congenital hypothyroidism,” “screening,” “late rise TSH” and “preterm newborn.”
Results
A total of 3578 preterm newborns (1649 females) were included, with a median GA of 32.8 (Q1–Q3: 32.7–32.9) weeks (Fig. 1), a mean birth weight of 1917 (CI: 1902–1931) g and a mean birth weight SDS of −0.2 SD (CI: −0.22 to −0.17). A birth weight SDS <-2.0 SDS was observed in 5.8%.
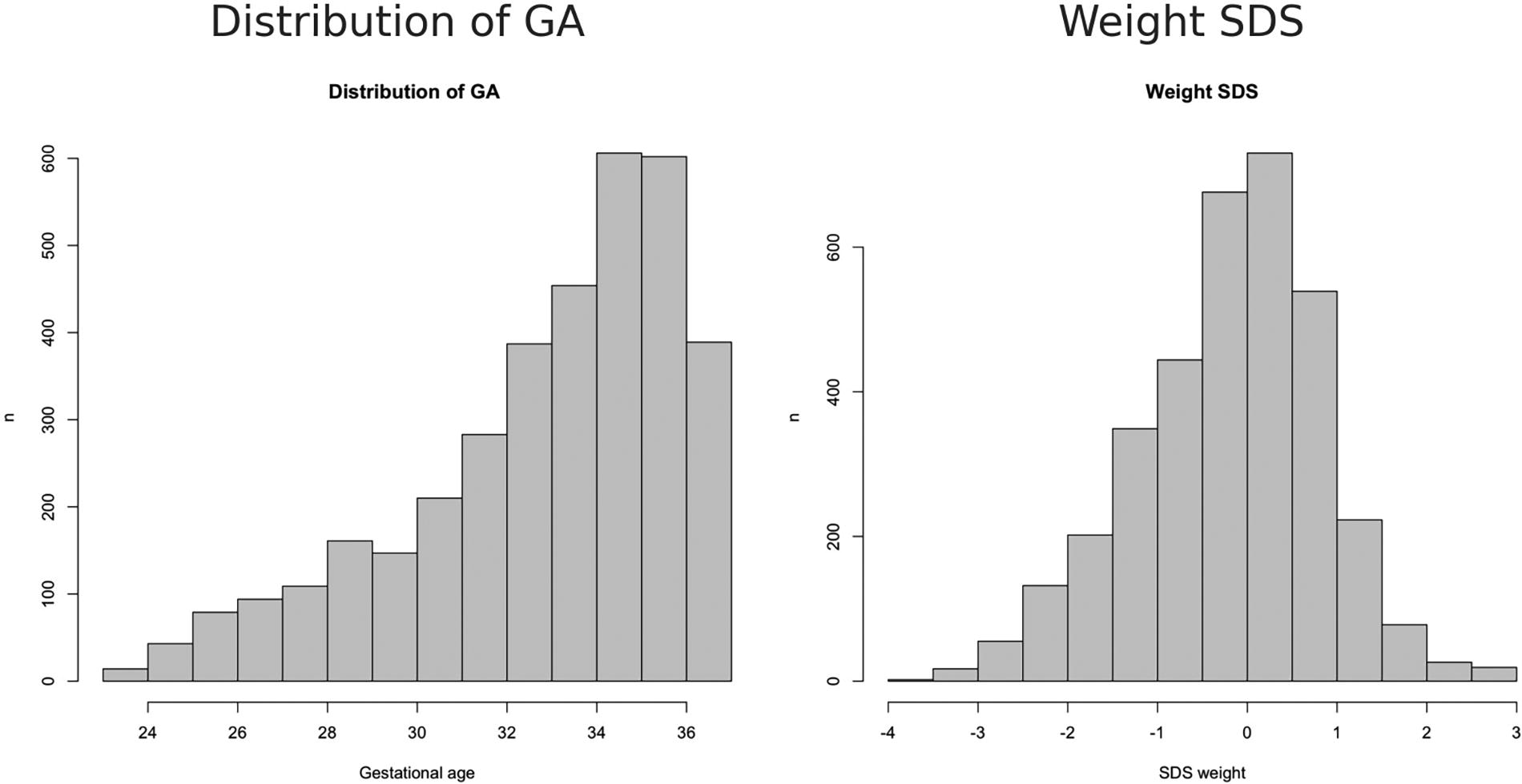
Distribution of gestational age and weight SDS in our cohort. GA, gestational age.
Ten out of the 3578 (0.3%) preterm babies were diagnosed with CH: six at the first screening, two at the second, and two at the third screening (Fig. 2). Their characteristics are detailed in Table 1.
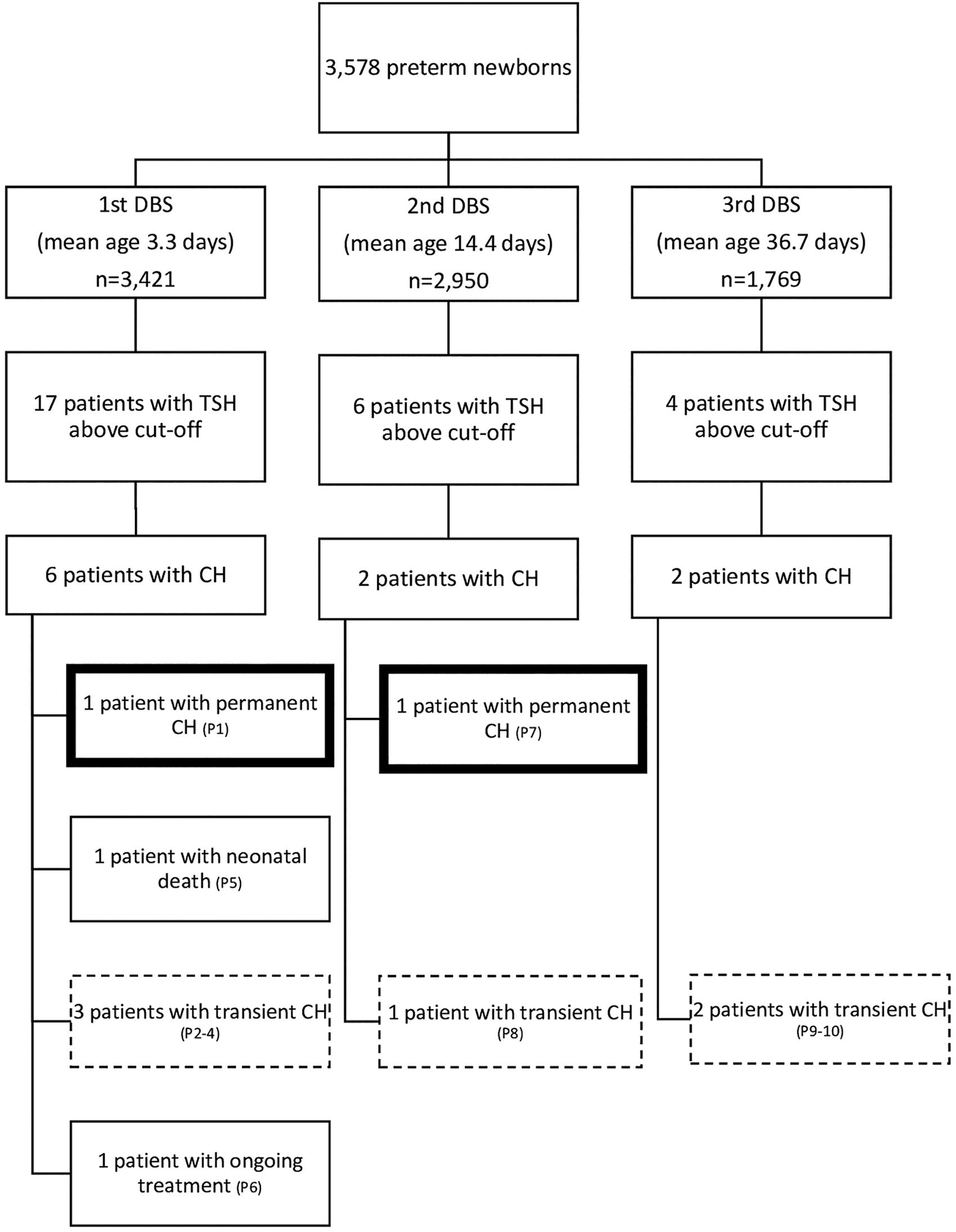
Flowchart of TSH screening results of preterm infants. TSH, thyrotropin.
Characteristics of the 10 Patients Diagnosed with Primary Congenital Hypothyroidism Among 3578 Preterm Infants Born between January 2014 and December 2023
In bold and italic, values that are not in the reference range.
Twins.
Patients diagnosed on second.
Patients diagnosed on third screening.
Iodine overload.
Neonatal death.
Treatment ongoing at 9 months at last follow-up (3.5 µg/kg/day of L-thyroxine).
Microdeletional syndrome + heterozygous PAX8 variant (3.8 µg/kg/day of L-thyroxine).
d, days; DBS, dry blood spot; GA, gestational age; GIS, gland in situ; P, patient; Tx, treatment; TSH, thyrotropin; W, weeks.
Among the six patients diagnosed with CH at first screening, two were twins (Patients 2 and 3). Only one patient (Patient 1) was confirmed to have permanent CH at the 1st screening, due to an ectopic thyroid gland, resulting in a frequency of permanent CH of 1 in 3578 (0.03%) in our preterm cohort. Patient 5 had a very high TSH level at first screening but unfortunately died during the neonatal period. One patient (Patient 6) is still receiving L-thyroxine due to his young age, with no weaning attempted yet. The remaining three patients had transient CH, with treatment durations ranging from 4 to 20 months.
Among the two patients diagnosed with CH at the 2nd screening (after a normal 1st screening result), Patient 7 had transient CH; Patient 8 was found to have permanent CH secondary to a class IV variant in the PAX8 gene, specifically the c.737delC (p.Pro246Glnfs*33variant). This frameshift variant causes a disruption in the function of the PAX8 protein, which is critical for thyroid development. This variant in PAX 8 gene has not been reported in the general population. Additionally, the patient has a 15q13.2q13.3 microdeletion syndrome, a genetic disorder that can cause a range of developmental and neurological issues. 23 She was delivered via emergency cesarean section due to abruptio placentae, following a twin pregnancy obtained through in vitro fertilization, during which the second fetus had died in utero. She has delayed motor and speech development.
The two neonates diagnosed with CH at 3rd screening (at 26 and 30 days of age, both with normal first screenings and no second screening due to their poor clinical condition at that time), were found to have transient CH.
None of the patients were receiving dopamine infusion at the time of first screening. The mothers of the two patients diagnosed at third screening (patient 9 and 10), but also those of patients 6 and 8 received corticosteroid treatment 2 days before cesarean section for pulmonary maturation. None of the mothers received L-thyroxine, and all had normal thyroid function. Maternal blocking antibodies were absent in patients 6–10 (not measured in the other mothers).
Among the six patients diagnosed with transient CH (1:596), two (33.3%) were small for GA and diagnosed at the 3rd screening (patients 9 and 10). Patient 9 underwent iodine-based skin disinfection on the 1st and 3rd days of life for esophageal and duodenal atresia. Although genetic testing was negative, the clinical presentation was suggestive of VACTERL (Vertebral defects, Anal atresia, Cardiac defects, Tracheo-Esophageal fistula, Renal anomalies, and Limb abnormalities) syndrome. Patient 10 was extremely preterm and dysmature and had a heterozygous GLIS3 class 3 variant. She had no associated dysmorphic features and had a normal development. Patient 4 also underwent an iodine-based skin disinfection for laparoschisis. Patients 2 and 3 were monochorionic–diamniotic twins; they had high thyroglobulin (>1000 µg/L) levels but no evidence of iodine overload. Patient 7 required prolonged resuscitation and was under therapeutic hypothermia at the time of the 1st screening.
After detailed clinical characterization and follow-up, we concluded that the frequency of permanent CH in this cohort of preterm newborns is 1/1789.
Table 2 summarizes the published studies reporting the frequency of permanent CH with delayed TSH rise (normal first screening) in cohorts of premature newborns.
Summary of Studies from the Literature Review in Which the Frequency of Permanent CH with Delayed Rise TSH Was Documented
Between January 2014 and December 2018 the cutoff was 15 mU/L. Since January 2019 the cutoff is the 99.5th centile, adjusted every 3 months on the basis of the results obtained during the last 12 months.
TSH cutoff: ≥ 50 mu/L: confirmed CH; TSH 25–50 mU/L: control TSH and treatment start; TSH 5-25 mU/L: control TSH and free T4 at 2, 4, and 8 weeks.
William and Down syndrome.
6 late rise permanent CH reported but no 1st DBS performed in 4; all had normal scan and TSH after 6–10 weeks of discontinuation was between (10.5, 10.59, 11.2, and 15.1 mU/L).
CH, congenital hypothyroidism; DBS, dry blood spot; P, permanent; T, transient; TSH, thyrotropin; W, week.
Discussion
Our retrospective study confirms that transient CH is more common than permanent CH in preterm newborns, with a respective frequency of 1 in 596 versus 1 in 1789.
The incidence of CH among preterm newborns in different studies is variable due to different TSH cutoffs, screening strategies, and diagnostic criteria. 6,24 –27 Some authors do not distinguish between transient and permanent CH. 4,14,21,22,33,34 Others include preterm newborns with hypothyroxinemia of prematurity who do not exhibit TSH elevation 35,36 We focused our literature review on the studies that allow to distinguish permanent from transient CH and early from late TSH rise. We found a frequency of permanent CH in preterms (1 in 1789) that is similar to one reported in other large published cohorts by Tuli et al. in 2023 (1 in 1483) 24 and Srinivasan in 2012 (1 in 1839). 32
In our cohort, one neonate with permanent CH was diagnosed on the first DBS while one was missed on the first DBS (delayed TSH rise) yielding a frequency 1:3578 of permanent CH with delayed TSH rise. In the literature, the frequency of permanent CH with delayed TSH rise in preterms ranges from 0 to 1:255. 24 –26,29,30,32
Both our study and literature review show that permanent CH is not always detected at first screening in preterm newborns. This supports the recommendation to retest preterm newborns. 2,37,38
The cause of the delayed TSH rise in some preterm newborns is often unknown and probably variable or multifactorial. In our cohort, the patient with a delayed TSH rise had both a microdeletion syndrome and a likely pathogenic variant in the PAX8 gene. It is interesting to note that PAX8 variants are known to cause CH due to thyroid dysgenesis, sometimes of late onset. 39 –41 In the cohort published by Campos-Martorell et al., the two preterm newborns with delayed TSH rise had Down and Williams syndrome respectively, which highlights the importance of the genetic work-up in patients with CH and in situ gland. 26
Another reason for a late TSH rise is acute iodine exposure which was documented in two newborns with transient CH in our cohort. The mild iodine deficiency of the adult Belgian population 42,43 might predispose to the marked Wolff−Chaikoff effect responsible for the profound hypothyroidism observed after iodine exposure in our setting. 44
On this basis, we suggest that, in preterm newborns with elevated TSH and normal thyroid morphology (gland in situ), a history of iodine exposure 45,46 and medications such as dopamine 47 or glucocorticoid 9 exposure should be sought along with maternal TSH-receptor-blocking antibodies. If negative, a genetic analysis (SNP array and panel of genes implicated in thyroid dysgenesis/dyshormonogenesis) could contribute to guide management.
Whether lower TSH cutoffs should be used for preterm newborns remains a matter of debate because of the risk of overdiagnosis and overtreatment. 48 Using a TSH cutoff of 7 rather than 15 mU/L, Olivieri et al. found an overrepresentation of preterm newborns: 12.4% compared with a national rate of preterm birth of 6% in Italy. 49 In contrast, in our unpublished cohort of patients with CH diagnosed between 2014 and 2023 (n = 88) (using the same TSH cutoff for term and preterm newborns), we found an underrepresentation of preterm newborns (3% of newborns with permanent CH were born preterm, while 46% of newborns with transient CH were preterms. The national rate for preterm births in Belgium is 8%). This underrepresentation of preterm newborns in cohorts of CH is expected, given the association between permanent CH and prolonged gestation (≥42 weeks of gestation). 50,51
Similarly, controversy persists regarding the management of preterm newborns with mild TSH elevation. Yoon et al. found no difference at 2 years in growth, cerebral palsy incidence, or neurodevelopment between 25 treated and 22 untreated extremely low birth weight infants (TSH >40 mU/L, normalizing within ∼30 days). 29 Woo et al. observed no difference in growth or neurodevelopment at 18 months between nine preterm infants with delayed TSH rise (two treated, seven untreated) and controls, although 2/9 had a smaller head circumference versus none in controls. 15 Nicksick et al. found no association between higher TSH centiles and adverse outcomes in 78 preterm newborns (mean GA 28.8 weeks). 52 Chung et al. reported that transient thyroid dysfunction resolving within 3 months was common in 177 preterms (<34 weeks) and not linked to poor outcomes, whereas persistent hyperthyrotropinemia (>3 months) may lead to adverse effects. 20 Conversely, Williams et al. showed that TSH ≥6 mU/L at birth was associated with significantly lower Bayley III scores at 2 years. 19 Additionally, higher but normal-range TSH levels at screening may predict neuromotor impairment in preterms without brain lesions. 53 Finally, Hung et al. concluded that GA, rather than transient TSH elevation, influences neurodevelopmental outcomes. 18
It is also important to note that, in term-born babies, overtreatment with levothyroxine may have harmful consequences. 54,55 Furthermore, some babies with mildly elevated TSH, including those born preterm, may carry a mono-allelic pathogenic variant in TSHR gene, which is not associated with developmental delay. 56,57
Avoiding the overdiagnosis of permanent CH in preterm newborns is a major challenge. 58 In this regard, it is worth mentioning that one-third of children labeled as having CH (one in 2360) by an NBS program in the United States discontinue thyroid hormone treatment by 3 years and remain euthyroid. However, the proportion of preterms in this study was not reported. 59
In our cohort, levothyroxine treatment was successfully discontinued before 3 years of age in patients with transient CH. Some studies indicate that discontinuation of levothyroxine therapy is possible at 2 years or even earlier for most preterm newborns with CH. 60,61 Kim et al. showed that discontinuing replacement treatment around the time of discharge from the neonatal intensive care unit appears to be safe and feasible in preterm newborns with delayed TSH rise. 62
This study has several limitations. Its retrospective and single-center design limits the generalizability of findings. The relatively small number of confirmed CH cases, especially permanent CH, limits statistical power. Moreover, for some patients still receiving L-thyroxine, definitive classification (transient vs. permanent CH) could not yet be established. Not all patients underwent genetic testing, which could have improved diagnostic accuracy. Finally, variability in the timing of the second DBS sample may have influenced the detection of delayed TSH rise.
Based on our observations and our literature review, we propose a management strategy for preterm newborns with elevated TSH levels on DBS screening (Fig. 3). Key steps include a detailed history of iodine exposure, assessment of maternal thyroid autoimmunity, thyroid ultrasound, and a genetic work-up, when feasible. These steps are essential for accurately determining the type of CH and for guiding early treatment discontinuation decisions.

Decision tree for management of preterm infants with TSH above cutoff on dried blood spot (DBS).
Conclusions
Permanent CH is rarer than transient CH among preterms and is not always identified on the first DBS screening. While the need for a second screening in preterms is debated, our study supports its continued use. Our article underlines the need for a more precise characterization of the preterms with suspected CH, including those with a delayed TSH rise (normal first DBS, abnormal 2nd DBS), such as clinical data about the neonatal period (including iodine or medication exposure), maternal TSH-receptor-blocking antibodies and a genetic work-up, especially for preterm babies with an in situ thyroid gland. This will allow to distinguish transient from permanent forms of CH and guide treatment decisions. In suspected transient forms, early levothyroxine weaning using a standardized protocol could be considered, with careful follow-up. Future research should focus on distinguishing between permanent and transient CH, as well as between early and late TSH rise, to improve diagnostic and treatment strategies. Finally, studies on the neurodevelopmental outcomes of children with transient CH are needed to determine whether treatment is truly beneficial for these patients.
Footnotes
Acknowledgments
The authors thank Ms. Tatiana Pereira from the neonatal screening program of the Fédération Wallonie−Bruxelles for allowing them to anonymously collect the data for the NBS program. The authors thank the health care workers of the following maternity hospitals: CHU Brugmann/HUDERF, CHIREC Delta, Hôpital Erasme, CHU Saint-Pierre, Hôpital Etterbeek-Ixelles, EpiCURA Ath, CHIREC Braine l’Alleud, CHU Marie-Curie (Vésale), CHU Ambroise Paré, CHR Haute Senne Soignies, CHU Tivoli, CHR Val de Sambre, from which the NBS data were collected.
Authors’ Contributions
All authors meet the ICMJE criteria for authorship, have approved the final version of the article, and agree to be accountable for all aspects of the work. E.B.: Conceptualization, methodology, formal analysis, writing—original draft, visualization, and investigation. V.V.: Investigation. L.M.: Methodology, formal analysis, and investigation. G.V.V.: Conceptualization, supervision, and writing—review and editing. M.A.: Investigation. C.H.: Methodology, supervision, and writing—review and editing. C.B.: Conceptualization, methodology, supervision, and writing—review and editing.
Author Disclosure Statement
The authors have nothing to disclose.
Funding Information
E.B. was supported by a grant from “The Belgian Kids Fund for Pediatric Research.”