
Abstract
Background:
A rare group of patients with differentiated thyroid cancers (DTCs) will have gross residual disease or recurrence following the standard primary therapies of surgical resection and radioactive iodine. In these patients with advanced DTC no longer amenable to further surgery, systemic, or radioactive iodine therapies, external beam radiation therapy (RT) is considered. Whether to add concurrent chemotherapy (CRT) to radiation for patients with advanced DTC remains unclear. We review the long-term follow-up of the largest single-institution experience on the use of RT alone versus CRT in advanced DTC.
Methods:
From 1989 to 2023, 327 patients with recurrent, gross residual, or unresected DTC were treated with RT alone or CRT. Patients with incomplete resection and/or unfavorable histology were preferentially treated with CRT. For this retrospective cohort study, locoregional control (LRC), distant metastasis-free survival (DMFS), and overall survival (OS) were evaluated using the Kaplan–Meier method.
Results:
CRT patients (n = 153) were 46% female and 61.6 ± 11.7 years old versus RT alone (n = 174) were 48% female and 66.8 ± 12.6 years old. Overall median follow-up was 109.7 months [confidence interval 100.3–123.5 months]. There were no differences in 4- and 10-year LRC, DMFS, or OS rates between groups (4-year LRC 89.0% RT alone vs. 86.6% CRT, p = 0.76; 4-year DMFS: 64.2% RT alone vs. 54.5% CRT, p = 0.08; 4-year OS: 58.5% RT alone vs. 56.9% CRT, p = 0.28). Worse grade 3+ acute dermatitis was reported with CRT (29% CRT vs. 10% RT alone, p < 0.0001). Eight patients developed a tracheoesophageal fistula (TEF), six of whom received CRT followed by tyrosine kinase inhibitor (TKI) therapy. TEF developed at a median of 7.3 months (range = 0.5–17.0 months) after TKI initiation. There were no differences in other acute toxicities, any late toxicities, rates of tracheostomy tube, percutaneous endoscopic gastrostomy (PEG) tube within 60 days of RT, or PEG tube persistence past one year.
Conclusion:
CRT did not demonstrate any benefit over RT alone in this retrospective study, although patients treated with CRT had worse disease. Late toxicities were similar, aside from greater TEF development after TKI therapy in CRT patients. Further research is necessary to elucidate who may benefit from CRT.
Introduction
Thyroid cancer is the 13th most common cancer in the US with a typically excellent prognosis. 1 This is in part due to effective local therapy, early diagnosis of smaller lesions, and the indolent nature of the differentiated thyroid cancers (DTCs), which make up 94% of all thyroid cancers. 1,2
The mainstay primary therapy for DTC is complete surgical resection with or without adjuvant radioactive iodine therapy (RAI). However, when tumor invades critical structures of the neck, complete surgical resection can be difficult, influencing the risk of recurrence. 3,4 While most patients (80%) are classified as low-risk, intermediate-risk patients have 21–36% risk of recurrence, and high-risk patients have as high as 68% risk of recurrence following initial surgery. 4 Most recurrences occur locoregionally. 5 Given the proximity of critical neck structures, locoregional disease control is important in reducing morbidity and maintaining quality of life.
In patients who have unresected recurrence or gross residual disease (GRD) refractory to RAI, the National Comprehensive Cancer Network recommends consideration of external beam radiation therapy (RT). 6 Previous retrospective studies from our group demonstrated improved locoregional progression-free survival (LPFS) and overall survival (OS) using radiosensitizing doxorubicin concurrent chemoradiotherapy (CRT) compared to RT alone in patients at high risk for local recurrence with tolerable toxicity. 7 –10 Beckham et al. observed a 4-year LPFS of 85.8% in the CRT group compared to 68.8% in the RT alone group, with no differences in late toxicity or percutaneous endoscopic gastrostomy (PEG) tube requirement. As a result of these findings, our institution implemented a practice change in 2010 that resulted in more patients receiving CRT than RT alone.
While intensity-modulated radiation therapy (IMRT) has become the standard RT technique in head and neck cancer, proton beam radiation therapy (PBRT) for DTC is not well studied. Recent reports have demonstrated the potential of PBRT, particularly for large thyroid tumors where IMRT is not feasible, with minimal toxicity. 11,12 Similarly, although tyrosine kinase inhibitors (TKIs) have been more widely studied recently, research on their use for DTC after RT is lacking. 5,13,14 We present what we believe to be the largest series of patients with the longest duration of follow-up, incorporating over 30 years of data and reflecting our practice change in 2010, to evaluate the long-term outcomes of definitive-intent CRT or RT alone in the treatment of locoregionally advanced or recurrent non-medullary, non-anaplastic thyroid carcinomas.
Materials and Methods
The Memorial Sloan Kettering Cancer Center’s institutional review board approved this multisite, single-institution retrospective cohort study, approval ID: RRP 16-1648. Patient confidentiality was maintained during data transfer as required by the Health Insurance Portability and Accountability Act. Between April 1989 and October 2023, there were 327 consecutive patients with pathologically confirmed gross residual or unresected DTC treated with definitive-intent RT. Unresected disease includes patients with upfront unresected or unresected recurrent disease. The M (distant metastasis [DM]) stage was determined at RT start. Other covariates include sex and age at RT start, prior recurrence, RAI, primary surgery status (unresected, hemi- or partial thyroidectomy, or total thyroidectomy), gross tumor volume (GTV), and the outcome of surgery (number of surgeries, extrathyroidal extension, lymph node dissection, and margin status of most recent surgery, i.e., negative, microscopic positive, GRD, or unresected). High-risk pathology was defined as presence of at least one of poorly differentiated histology, oncocytic carcinoma histology, or tall cell variant of papillary carcinoma. RT was utilized in this setting for patients who the head and neck disease management team felt were at high risk of recurrence without surgical salvage options. The primary outcomes were locoregional control (LRC), DM-free survival (DMFS), and OS, and secondary outcomes were toxicity and role of prognostic variables.
Radiotherapy Technique
Our radiation technique has been described previously. 8,10 Briefly, we treated various clinical target volumes as follows: (1) low-risk areas including elective lymph node volumes to 50–54 Gy, (2) high-risk areas including the operative or tumor bed, operative thyroid gland volume, tracheoesophageal grooves, and central nodal compartment to 60 Gy, (3) close or microscopically positive margins to 66 Gy, and (4) areas of gross disease to 70 Gy. Since 2016, we have omitted the lateral neck from elective target volumes except when involved with gross disease. All target volumes were expanded by 3–5 mm to a planning target volume to account for intra-fraction patient motion and inter-fraction setup error. All patients were immobilized in the treatment position using a three- or five-point Aquaplast mask.
Toxicity and response assessment
Toxicities were recorded retrospectively with chart review. Patients were assessed jointly by radiation and/or medical oncology weekly during radiation and at approximate intervals of 4, 8, and 12 weeks after RT, then every 3–4 months for 2 years, followed by every 6–12 months thereafter. Acute toxicity events (dermatitis, nausea, vomiting, mucositis, xerostomia, dysphagia, voice changes, dysgeusia, and fatigue) were recorded based on the worst-grade toxicity sustained by patients up to 90 days after RT start using the contemporaneous National Cancer Institute’s Common Terminology Criteria for Adverse Events. 15 Late toxicity events (xerostomia, dysphagia, voice changes, dysgeusia, fatigue, laryngeal edema, and fibrosis) were recorded based on the worst-grade toxicity sustained >90 days after completion of treatment based on the Radiation Therapy Oncology Group late radiation morbidity scoring system. 16 Use of vascular endothelial growth factor-TKIs, development of tracheoesophageal fistula (TEF), and PEG and tracheostomy tube incidence and timing (before, during/within 60 days, or >60 days after RT start) were also recorded.
Statistical analysis
LRC, DMFS, and OS were calculated from the start of radiotherapy. LRC was defined as either local (i.e., thyroid bed) or nodal (i.e., central compartment, cervical, and/or superior mediastinal) disease progression within the RT treatment field (i.e., new or enlarging disease seen on imaging). Biopsy confirmation was not required. Stable disease without progression was not classified as progression. If systemic therapy or RAI was initiated after RT for suspicion of progressive disease, these patients were classified as having locoregional progression.
Duration of outcomes was calculated from RT start to the date of locoregional recurrence, DM, death, or last clinical follow-up and estimated with the Kaplan–Meier method. Log-rank tests were used to compare survival curves. The reverse Kaplan–Meier method estimated median follow-up. Cox hazard ratios were used for univariable (UVA) and multivariable (MVA) analyses. Any variable with p < 0.200 on UVA was included in MVA, and hazard ratios were generated using backward stepwise regression with a cutoff of p < 0.10. Concurrent chemotherapy (CRT) was always included in MVA. If high-risk histology or any of its components had p < 0.200 on UVA, only the significant individual variables were included. Separate analyses were conducted for patients with GTV (Supplementary Fig. S5, Supplementary Table S3). Comparisons between cohorts were performed using chi-square tests, Wilcoxon rank-sum tests, logistic regression, or Fisher’s exact test where appropriate. Statistical significance was set a priori at p = 0.05. Analyses were conducted using SAS 9.4. 17
Results
Patient and tumor characteristics
A total of 327 patients received RT between April 1989 and October 2023 (Fig. 1). The median age of RT start was 64.4 ± 12.4 years (range = 22.8–92.0 years) with median follow-up of 9.1 years (0.23–18.7 years) for all patients (Table 1). The most common histology was papillary (164/327, 50%), including tall cell variant (94/327, 29%), followed by poorly differentiated (125/327, 38%), and oncocytic carcinoma (35/327, 11%). Overall, 233 patients (71%) had high-risk pathology. There were 27 patients (8%) with upfront unresected tumors and 64 patients (20%) with unresected recurrent tumors. GRD was identified in 135 patients (41%). Before RT, 205 patients (63%) had locoregional recurrence, and 116 patients (35%) had DM (lung (90/116, 78%), bone or spine (35/116, 30%), liver (7/116, 6%), and brain (6/116, 5%).

Participant flow diagram. RT, radiation therapy; MTC, Medullary thyroid carcinoma.
Demographic and Clinical Data
Well or moderately differentiated papillary thyroid carcinoma or differentiation not listed.
Comprises “high-risk histology.”
TKI: vascular endothelial growth factor-tyrosine kinase inhibitors.
CRT, concurrent chemotherapy; RT, radiotherapy; SD, standard deviation; TKI, tyrosine kinase inhibitor.
Treatment characteristics
The median RT dose was 6600 cGy (range = 900 cGy–7660 cGy) in a median 33 fractions (range = 4–40 fractions) delivered Monday through Friday. There were 275 patients (84%) treated with IMRT (Supplementary Fig. S4), 10 patients (3%) treated with PBRT (Supplementary Data S1), and 42 patients (13%) treated with 2D or 3D RT. CRT was administered to 153 patients (47%), of which 6 received PBRT. Before 2010, 28/116 patients (24%) received CRT; on logistic regression, M1 disease and age <60 years predicted receipt of CRT. After 2010, 125/211 patients (59%) received CRT, with GRD, unresected disease, and poorly differentiated histology predictive of CRT (Supplementary Table S1).
Chemotherapy
Most patients (143/153, 93%) who were treated using CRT received once weekly doxorubicin 10 mg/m2 starting in the first week of CRT. Two patients received doxorubicin 20 mg/m2, and two patients received 30 mg/m2. Six patients received paclitaxel, of which one also received carboplatin.
Tyrosine kinase inhibitor
There were 67 patients (20.5%) who received TKI, of which 8 received TKI pre-RT. CRT patients were more likely to receive TKI (23/174, 29% CRT vs. 44/153, 13% RT alone, p = 0.0005, Table 1). Most patients first trialed sorafenib (27/67, 40.3%) or lenvatinib (21/67, 31.3%). The most frequently used TKIs were lenvatinib, sorafenib, and pazopanib (Supplementary Table S4). The median treatment duration, which includes treatment breaks or treatment with another TKI or immunotherapy, was 11.7 months (range = 0.5–149.7 months).
Toxicity
Toxicities are summarized in Table 2. Acute grade 3 dermatitis was reported in 19% of patients, more frequently in those receiving CRT (29% CRT vs. 10% RT alone, p < 0.0001). There were no differences between groups in other acute toxicities, any late toxicities, incidence of PEG, or tracheostomy tube prior to or within 60 days of RT. Receipt of PEG tube >60 days after completing RT was greater in the CRT group (4% RT alone vs. 12% CRT, p = 0.005). There was no difference in PEG tube dependence one-year post-treatment (4% in both, p = 0.96) for patients who received PEG prior to or during/within 60 days of RT. Overall, 31 patients (6%) required tracheostomy tube after RT start, which was not statistically different between groups.
Toxicities
PEG, percutaneous endoscopic gastrostomy; Trach, tracheostomy.
Eight patients (2.1%) developed a TEF at a median of 34.7 months after RT start (range = 17.9–84.5 months). All TEF patients received CRT, and six of them received TKI therapy after CRT at a median of 20.2 months (range = 13.7–43.9 months) after RT for progressive or metastatic disease. TEF developed at a median of 7.3 months (range = 0.5–17.0 months) after TKI initiation. The other two patients received dabrafenib and selpercatinib. For all eight patients, median survival after TEF formation was 6.6 months (range = 0.1–22.6 months).
Locoregional control
The 4-year and 10-year LRC were 88.0% and 74.3%, respectively (Supplementary Fig. S1a). There were 46 patients (14.1%) with locoregional failures at a median of 20.8 months (range = 1.2–121.0 months), which includes 26 patients (15.0%) treated with RT alone and 20 patients (13.0%) treated with CRT. There was no difference in the 4-year LRC between RT alone and CRT (89.0% RT alone vs. 86.6% CRT, p = 0.76) (Fig. 2a). Unresected tumor was associated with decreased 4-year LRC (81.8% unresected vs. 90.2% resected, p = 0.002) (Supplementary Fig. S1b). There was no difference in LRC according to the extent of residual disease (R2 vs. R1, p = 0.71), metastasis stage (M0 vs. M1, p = 0.15), or pathology (high-risk vs. low-risk, p = 0.11).
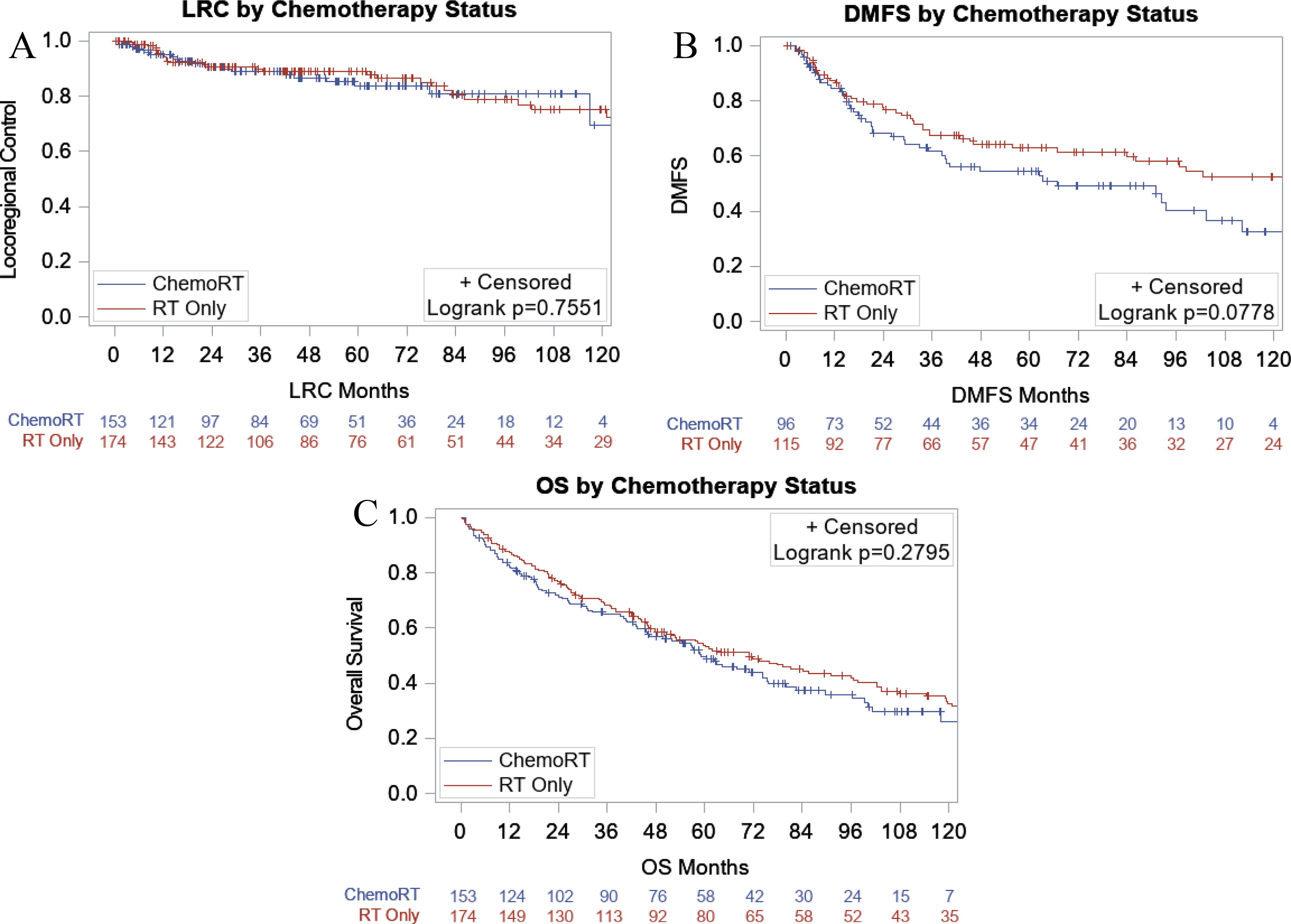
Locoregional control, distant metastasis-free survival, and overall survival by chemotherapy status. Kaplan–Meier estimates of LRC (
Distant metastasis-free survival
Of 211 patients without metastases at RT start, 92 patients (44%) subsequently developed metastases after a median 19.8 months (range = 2.2–162.7 months). The 4-year and 10-year DMFS were 60.0% and 44.9%, respectively (Supplementary Fig. S2a). There was no difference in 4-year DMFS between RT alone and CRT (64.2% RT alone vs. 54.5% CRT, p = 0.08) (Fig. 2b). High-risk pathology was associated with worse 4-year DMFS (55.6% high-risk vs. 71.9% low-risk, p = 0.003) (Supplementary Fig. S2b). There was no difference between groups by resection status (p = 0.41). The most common sites of metastatic failure were lung (85/211, 40%), bone including spine (48/211, 23%), brain (23/211, 11%), and liver (13/21, 6%).
Overall survival
The 4-year and 10-year OS were 57.7% and 29.9% for all patients (Supplementary Fig. S3a). There were 209 deaths (64%) at a median of 35.0 months (range = 0.5–269.3 months). There was no difference in 4-year OS between RT alone and CRT (58.5% RT alone vs. 56.9% CRT, p = 0.28) (Fig. 2c). The presence of metastases at RT start was associated with decreased 4-year OS (40.8% M1 vs. 67.2% M0, p < 0.0001) (Supplementary Fig. S3b). There were no differences in OS in unresected versus resected (p = 0.40) or high- versus low-risk pathology (p = 0.24).
UVA and MVA analysis (Supplementary Table S2)
Unresected tumor was associated with worse LRC on UVA and MVA (HR 2.60, [CI 1.44–4.67], p = 0.002). On UVA, high-risk and poorly differentiated histology were associated with worse DMFS, while tall cell histology was associated with improved DMFS. On MVA, poorly differentiated histology was associated with worse DMFS (HR 2.69, [CI 1.91–3.79], p < 0.0001). On UVA, M1 status and poorly differentiated histology were associated with worse OS, while tall cell histology was associated with improved OS. On MVA, M1 status (HR 2.56, [CI 1.03–3.44], p < 0.0001), poorly differentiated histology (HR 1.78, [CI 1.33–2.39], p = 0.0001), oncocytic carcinoma histology (HR 1.77, [CI 1.13–2.77], p = 0.012), and gross residual or unresected disease (HR 1.45, [CI 1.05–2.00], p = 0.023) were associated with worse OS. The subset analysis for patients with GTV is reported in Supplementary Data S2, Supplementary Table S3, and Supplementary Figure S5.
Discussion
The present study provides long-term results of patients with advanced DTC treated with RT and demonstrates that patients with worse prognostic factors, such as unresected or poorly differentiated histology, treated with CRT have similar survival to those with more favorable prognosis treated with RT alone.
Previous studies have demonstrated the efficacy of adjuvant RT for DTC. 18,19 This effect is even greater in patients at increased risk for recurrence. 20 However, these studies do not delineate the role of concurrent CRT. Given the rarity of this clinical entity, our findings build on prior work from our group. Beckham et al. found that CRT improved LPFS and OS compared with RT alone. 7 Prior to that, Romesser et al. reported non-significant differences in survival outcomes between patients treated with CRT and RT alone. 8 The present study includes the long-term results of these two studies as well as a more recent cohort. We note sustained, long-term survival in terms of LRC, DMFS, and OS with no differences between the CRT and RT alone cohorts. We observed, in our study, a greater proportion of patients with unresected disease treated with CRT (39% vs. 18%) and a non-significantly greater proportion of patients with poorly differentiated histology treated with CRT (44% vs. 33%). We note a decreased 4-year LRC in the unresected cohort (81.8% unresected vs. 90.2% resected, p = 0.002); this LRC rate is still commendable, and when treated with CRT, the survival outcomes were not statistically different compared to the cohort with more favorable prognosis treated with RT alone. Despite no clear survival benefit of CRT, the observation that patients with more advanced tumors who may not be eligible for surgery have similar outcomes when treated with CRT represents an important data point that can be used during shared decision making.
With a large portion of the cohort (69%) having gross residual or unresected disease, we were interested in determining whether survival outcomes were influenced by tumor volume at RT start. Similarly to Beckham et al., we observe no difference in LRC or DMFS for patients with the highest quartile of GTV compared to the lower three quartiles. This suggests that even patients with bulky residual tumors can attain sustained LRC with RT comparable to those with microscopic residual disease. However, in contrast to Beckham et al., we observe that the highest quartile GTV was associated with worse OS, which was substantiated on MVA, possibly explained by the presence of metastatic disease prior to RT. Further analysis suggests that oncocytic carcinoma histology, in combination with any volume of gross disease, is associated with worse LRC, DMFS, and OS. Attempted resection for these patients may be beneficial.
RT appears to have been well tolerated among patients in the present study. Dermatitis was the most common acute toxicity with incidence rates comparable to that found by Beckham et al. 7 In contrast to that study, which found no significant difference, we observe significantly greater acute dermatitis in the CRT group (30% vs. 9% RT alone). Other acute toxicities were infrequent. Late toxicities did not differ between groups, with voice changes being the most common (25%). Rates of PEG tube placement, 7% in each of the acute and late phase, are similar to other studies: Goodsell et al. reported a rate of 12% in patients with non-anaplastic thyroid cancer treated with RT. 21 Importantly, the rate of PEG tube persistence for >1 year was low in both RT alone and CRT. PEG placement can significantly impact patients’ quality of life and has been associated with mortality, underscoring the importance of early and aggressive swallow rehabilitation in patients who develop this complication. 21
The development of TEF in our cohort was low (2.4%). The risk factors for TEF formation during TKI therapy historically included prior esophageal procedure, radical neck surgery, tumor involving the trachea or esophagus, and/or a history of RT. 22 Blevins et al. documents a case series of three patients who developed fistula following TKI therapy after RT for thyroid cancer. 22 Our observed rates are comparable to that listed on the product warning label for fistula formation with cabozantinib (4%) and lenvatinib (2%) and may suggest that TKIs themselves pose a risk of TEF regardless of RT. 23,24 However, our data may also suggest that there should be increased concern for TEF in the setting of CRT followed by TKI, given that all patients who developed TEF received CRT. Further research is warranted to better understand the benefits versus risks and complications of TKIs, especially when considering initiating RT versus TKI therapy, or in patients who have progressed following RT. This is especially relevant in today’s clinical environment since targeted immunotherapy is considered in many cases of progressive DTC or anaplastic thyroid cancer. 22,25,26
There are several limitations to this study. Patients treated with CRT were significantly younger than those treated with RT alone, potentially introducing a selection bias. As a single-institution retrospective analysis spanning three decades, prospective comparison of patients treated with RT to those treated with other, more modern, modalities (TKIs, chemotherapy alone, or observation) cannot be made. The RT technique has changed over the years, and we included patients who started RT but did not complete treatment due to death or patient factors. We also included patients who received chemotherapy with a regimen other than doxorubicin 10 mg/m2. While this allows for a greater understanding of future interventions for patients with advanced DTC, it adds some heterogeneity to the cohort. Finally, while toxicity grading was reported using a standardized form, evaluation varies between practitioners, and the data collection tool has evolved over the years. These limitations underscore the need for prospective studies in this group of patients, which may need to span multicenter or multinational settings due to the rarity of this clinical entity.
Conclusion
CRT for patients with unfavorable surgery status or histology was associated with similar survival outcomes compared to those treated with RT alone. Additionally, local control rates with CRT were high even among patients with unresectable disease. Late toxicities were comparable, aside from greater TEF development after TKI therapy in CRT patients. Taken together, these findings may help inform shared decision making regarding CRT or RT alone in patients with advanced DTC. Further research is warranted in delineating the role of systemic agents such as TKI in patients who progress after RT.
Footnotes
Acknowledgment
Abstract was presented at the American Society for Radiation Oncology Annual Meeting in Washington, DC, October 2, 2024.
Authors’ Contributions
J.C.: Conceptualization, methodology, data collection, formal analysis, writing—original draft, writing—review and editing, approval of final version to be published, and accountable for all aspects of the work. E.S.: Conceptualization, methodology, formal analysis, writing—review and editing, approval of final version to be published, and accountable for all aspects of the work. E.C.D.: Methodology, data collection, formal analysis, writing—review and editing, approval of final version to be published, and accountable for all aspects of the work. T.T.: Methodology, data collection, formal analysis, writing—review and editing, approval of final version to be published, and accountable for all aspects of the work. K.Z.: Methodology, formal analysis, writing—review and editing, approval of final version to be published, and accountable for all aspects of the work. J.J.K.: Methodology, formal analysis, writing—review and editing, approval of final version to be published, and accountable for all aspects of the work. Y.Y.: Methodology, formal analysis, writing—review and editing, approval of final version to be published, and accountable for all aspects of the work. L.C.: Methodology, formal analysis, writing—review and editing, approval of final version to be published, and accountable for all aspects of the work. A.S.: Methodology, formal analysis, writing—review and editing, approval of final version to be published, and accountable for all aspects of the work. S.M.: Methodology, formal analysis, writing—review and editing, approval of final version to be published, and accountable for all aspects of the work. N.R.: Methodology, formal analysis, writing—review and editing, approval of final version to be published, and accountable for all aspects of the work. A.H.: Methodology, formal analysis, writing—review and editing, approval of final version to be published, and accountable for all aspects of the work. M.T.: Methodology, formal analysis, writing—review and editing, approval of final version to be published, and accountable for all aspects of the work. J.F.: Methodology, formal analysis, writing—review and editing, approval of final version to be published, and accountable for all aspects of the work. M.S.: Methodology, formal analysis, writing—review and editing, approval of final version to be published, and accountable for all aspects of the work. J.C.: Methodology, formal analysis, writing—review and editing, approval of final version to be published, and accountable for all aspects of the work. A.S.: Methodology, formal analysis, writing—review and editing, approval of final version to be published, and accountable for all aspects of the work. R.W.: Methodology, formal analysis, writing—review and editing, approval of final version to be published, and accountable for all aspects of the work. R.G.: Methodology, formal analysis, writing—review and editing, approval of final version to be published, and accountable for all aspects of the work. N.K.: Methodology, formal analysis, writing—review and editing, approval of final version to be published, and accountable for all aspects of the work. N.Y.L.: Conceptualization, supervision, methodology, formal analysis, writing—review and editing, approval of final version to be published, and accountable for all aspects of the work.
Author Disclosure Statement
J.C., E.S., E.C.D., T.T., K.Z., J.J.K., Y.Y., L.C., A.S., S.M., N.R., A.L.H., M.T., J.F., M.S., J.C., A.S., R.W., R.G., and N.K. have no conflicts of interest to disclose. N.Y.L. is on the advisory board (consultant) for Merck, Merck Serono, Nanobiotix, Galera, LEO SAB, and GSK and receives stock options from LEO SAB.
Funding Information
This article is funded by the Cancer Center Support Grant from the National Cancer Institute (P30 CA008748). J.C., E.S., T.T., K.Z., J.J.K., Y.Y., L.C., A.S., S.M.M., N.R., A.L.H., R.M.T., J.F., M.S., J.C., A.S., R.J.W., R.G., N.K., and N.Y.L. declare that they have no funding information to disclose. E.C.D. is funded in part through the Prostate Cancer Foundation Young Investigator Award.
Supplementary Material
Supplementary Data
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.