
Abstract

We report three patients from our clinical endocrinology practice who were diagnosed with amiodarone-induced thyrotoxicosis (AIT) shortly after starting semaglutide, a glucagon-like peptide 1 (GLP-1) analogue. Prior to semaglutide treatment, all three patients had normal thyroid function tests.
For this description of cases, ethics board review was not required, as per Swiss law (as confirmed by our hospital research promoter’s office). All patients provided written informed consent for reporting of their case.
The first patient was a 71-year-old male with metabolic syndrome who presented with thyrotoxicosis in May 2022. He had heart failure with reduced ejection fraction (HFrEF); due to atrial fibrillation, he was treated with amiodarone for 32 months (until November 2021). In March 2022, he was started on semaglutide at 0.25 and then 0.5 mg/week, resulting in a weight loss of 20 kg in the first 2 months. Thyroid function tests then showed suppressed TSH with elevated free T4 of 33.4 pmol/L (normal range [NR] 10.9–22.2) and free T3 of 9 pmol/L (NR: 3.1–6.8).
The second patient was a 40-year-old male with HFrEF due to idiopathic dilated cardiomyopathy. He presented with thyrotoxicosis in January 2025, having been on amiodarone treatment for over 3 years. Due to class I obesity (BMI 30.2 kg/m2), the patient started semaglutide treatment in September 2024 in preparation for cardiac transplantation; the semaglutide dose was increased progressively to 2.4 mg/week. At the 16-week follow-up, thyroid function tests revealed suppressed TSH with elevated free T4 of 33.3 pmol/L (NR: 11.2–24.1) and free T3 of 8.5 pmol/L (NR: 3.1–6.8).
The third patient was a 56-year-old female with class I obesity and HFrEF with multiple episodes of ventricular tachycardia, who was treated with amiodarone since August 2024. During a hospitalization for ablation of ventricular tachycardia in December 2024, her cardiologist started her on semaglutide 0.25 mg/week for cardiovascular protection. In February 2025, thyroid function tests showed suppressed TSH with elevated free T4 of 56 pmol/L (NR: 12–22) and free T3 of 8.36 pmol/L (NR: 3.95–6.8).
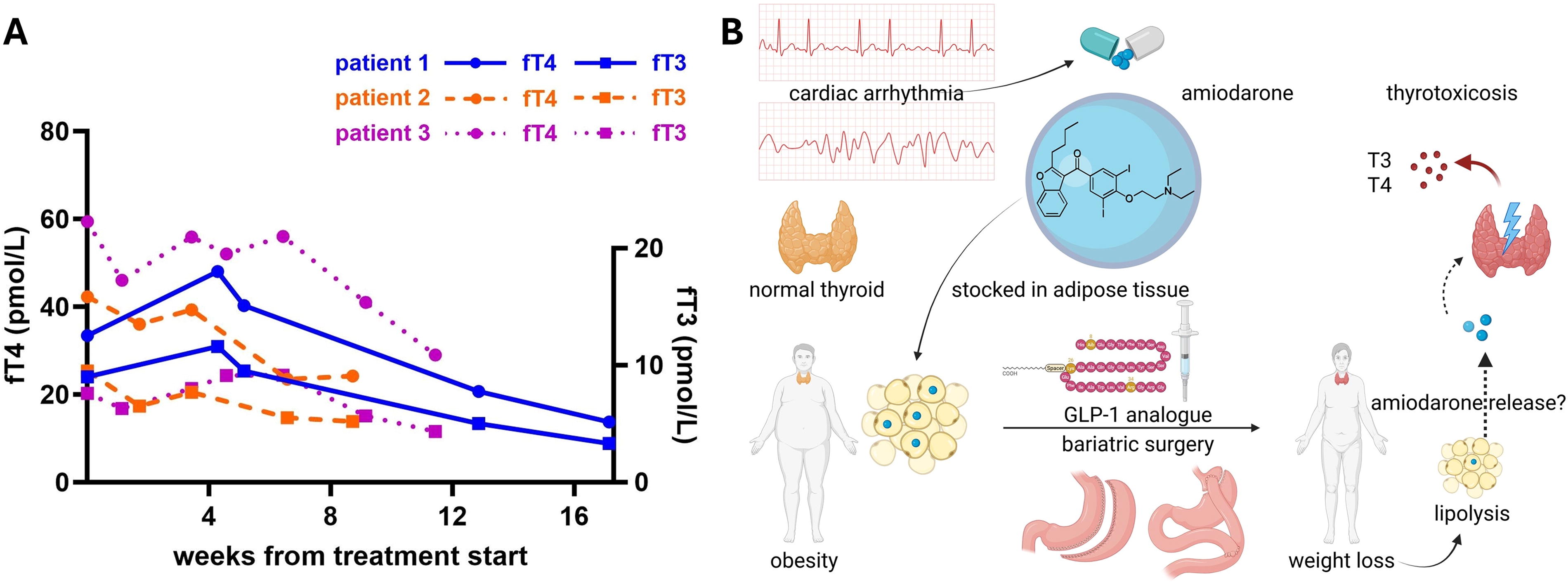
Except for the weight loss and some gastrointestinal symptoms attributed to semaglutide, the patients reported no other symptoms of thyrotoxicosis. In all cases, thyroid ultrasound showed mild hypoechogenicity and heterogeneity of the parenchyma without hypervascularization, suggesting type 2 AIT. However, the first patient was treated only with antithyroid drugs (ATD) (carbimazole) given his uncontrolled diabetes. The second patient was treated with prednisone, and the third patient was started on combined treatment with prednisone and ATD. The thyroid function tests rapidly improved in all three patients (Fig. 1A).
Two different groups have each described a respective case of AIT after weight loss induced by bariatric surgery, 1,2 but to our knowledge, no studies have directly examined the relationship between semaglutide-induced weight loss and AIT.
Our proposed hypothesis is that because amiodarone is stored in adipose tissue, a substantial and rapid weight loss, like the one associated with bariatric surgery or with GLP-1 analogue treatment, could induce a large release of amiodarone from adipose tissue, increasing exposure of the thyroid to amiodarone’s toxic effects (Fig. 1B). This could manifest as AIT, which in turn could potentially exacerbate the weight loss.
While several studies have demonstrated the extensive accumulation of amiodarone and its metabolite in adipose tissue, 3,4 there is no specific study on the pharmacokinetics of amiodarone after weight loss. There are, however, studies on other lipophilic substances, with some raising concern about the release of stored environmental lipophilic toxins. 5 As for amiodarone, there is indirect evidence that its lipophilic properties could impact its clinical efficacy. For example, one study showed an inverse relationship between BMI and amiodarone’s efficacy in reverting atrial fibrillation. 6
While a chance occurrence of AIT in patients undergoing significant weight loss cannot be excluded, the pharmacokinetic properties of amiodarone could account for the timing of AIT development after substantial and/or rapid weight loss. Formal research studies are needed to explore any potential association between weight loss and AIT development.
Pending such evidence, the cases reported in the literature and herein underscore the importance of monitoring thyroid function tests in amiodarone-treated patients undergoing weight loss treatment with bariatric surgery or GLP-1 analogues. Based on our clinical observations, we suggest screening for thyroid dysfunction more frequently (every 6–12 weeks) in amiodarone-treated patients during periods of rapid weight loss, such as after bariatric surgery or treatment with GLP-1 analogues. Recent real-life data show that exposure to thyrotoxicosis is linked to higher cardiovascular events and mortality in AIT patients, 7 hence timely diagnosis and optimal treatment are critically important. Moreover, both amiodarone and potential concurrent cardioprotective medications like beta-blockers may mask symptoms of thyrotoxicosis. This may also explain the pauci-symptomatic presentation observed in our patients and in many AIT patients, and it reinforces the importance of biochemical screening for thyroid dysfunction.
Footnotes
Authors’ Contributions
I.G.: Conceptualization, data analysis, writing—original draft. G.P.S.: Supervision, validation, writing—review and editing.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.