
Abstract
Background:
Thyroid cancer survivors may experience significant health-related quality-of-life (HRQoL) detriments. Currently available HRQoL survey tools, used in isolation, can be insensitive to change over time and may incompletely assess thyroid cancer-specific symptoms and fear of cancer recurrence. This study aimed to measure the trajectory of HRQoL changes in thyroid cancer survivors using repeated measures, comparing commonly used surveys, over the first 12–18 months following diagnosis.
Methods:
A prospective longitudinal cohort study recruited all patients with newly diagnosed thyroid cancer (excluding low-risk papillary thyroid microcarcinoma and anaplastic thyroid cancer) from a mixed metropolitan and regional health district (public and private). Patients were invited to complete Short Form-12 (SF-12), EORTC-QLQ-C30, Thyroid Cancer Quality of Life (ThyCaQoL) Survey, City of Hope–Thyroid Version, and Assessment of Survivor Concerns surveys postoperatively, and at 3, 6, and 12 months. Responses were assessed for changes over time, and multivariable analysis was used to identify variables associated with outcomes at follow-up.
Results:
Between January 2021 and June 2023, 111 patients completed surveys at a minimum of one time point (response rate 59%). Most were female (72%), mean age 55 years, 56% metropolitan, 56% privately insured, 55% American Thyroid Association low-risk differentiated thyroid cancer. Treatment included surgery (total thyroidectomy 49%, two-stage thyroidectomy 24%, lobectomy 25%, active surveillance 2%); 58% received radioactive iodine ablation. At the completion of the study, 82% were euthyroid and 92% disease-free. At all time points, SF-12 physical and mental component scores (PCS and MCS), remained below normative population values (>12 months; mean PCS = 39.4, mean MCS = 46.7, normative = 50). MCS showed more consistent improvement over the first year following thyroid cancer diagnosis (global p = 0.03). ThyCaQoL surveys identified improvement in voice and scar symptoms (p < 0.01 each), but distress regarding neuromuscular (p < 0.01), sensory symptoms (p = 0.01), and weight gain (p = 0.04) worsened over the course of the study. Fear of cancer recurrence was common and persisted over time.
Conclusion:
A year after diagnosis, thyroid cancer survivors have persisting HRQoL deficits with some symptoms worsening over time. As part of follow-up care, clinicians should specifically inquire about persistent symptoms that could affect HRQoL. Supportive care interventions for those with persistent HRQoL deficits are required.
Introduction
Thyroid cancer diagnoses have increased markedly 1,2 with overdiagnosis being common. 3,4 A diagnosis of “cancer,” even with good prognosis, brings the potential for psychosocial harm. 5,6 Individuals must process their cancer diagnosis and consider treatment options simultaneously. 7 –10 In thyroid cancer management, recent guideline-driven de-escalation of the extent of surgery and more selective radioactive iodine use requires a greater understanding of not just disease outcomes but also patient reported outcomes (including physical, psychological, and social functioning) to facilitate individualized treatment decisions. 11,12
While the literature investigating health-related quality of life (HRQoL) in thyroid cancer survivors is expanding, many studies have been performed in the context of survivorship groups, cancer registries, academic centers, or clinical trials evaluating different surgical techniques. 13 –15 A variety of generic and thyroid cancer-specific surveys are used, but often in isolation and at single time points. 13,16 Few studies compare the trajectory of HRQoL over time with reference to population values. 13,16 –18 Furthermore, fear of cancer recurrence (common in thyroid cancer survivors and often disproportionate to clinical prognosis) is not evaluated by most generic or thyroid cancer-specific surveys. 19 –21 HRQoL impacts of cancer diagnoses and fear of cancer recurrence may differ between different populations, ethnicities, and demographic groups. 22 –24 In Australia, there are disparities in thyroid cancer stage at diagnosis dependent on geography and access to health care, 25 as well as a lack of quantitative patient outcomes research in thyroid cancer survivors. 26 –28
This study aimed to comprehensively assess the HRQoL of thyroid cancer survivors within a population prospectively recruited from an Australian mixed metropolitan–regional health care network. The wider prospective longitudinal cohort study included assessments of recruitment methods, acceptability and comprehensiveness of surveys, 29 a detailed qualitative interview study with thyroid cancer survivors, 30 and measures of financial toxicity. This study measures the trajectory of HRQoL changes over the first year of the thyroid cancer survivorship journey, as measured by validated surveys encompassing generic, thyroid cancer-specific, and fear of cancer recurrence measures. These data aim to compare HRQoL outcomes to normative data and provide comprehensive, quantitative HRQoL assessment across domains and surveys.
Methods
Participants and setting
All patients with a new diagnosis of thyroid cancer (excluding anaplastic cancer and papillary thyroid microcarcinoma without adverse features) within Hunter New England Local Health District (HNELHD), New South Wales, Australia, were eligible for recruitment. HNELHD has an area of 131,785 km2 with an estimated population of 962,000, spanning metropolitan, regional, and rural areas. 31 Patients were excluded if aged <18 years, or lacked adequate language, cognitive, or computing skills to complete surveys. Following a pilot phase, recruitment methods were enhanced (patient eligibility screened by a senior clinician, and recruitment by either the clinical team or an oncology-trained research assistant), and the study commenced in January 2021. 29 Demographics, clinical characteristics, and treatment details were collected from the electronic medical record for all eligible patients. Responders self-reported their education status, smoking history, and use of thyroid hormone replacement. All data were collected and stored in a Research Electronic Data Capture (REDCap®) database. 32
Surveys
After providing informed consent, participants were sent a survey link via email. Initial attempts to recruit patients at the time of diagnosis were abandoned after only a few months, as participants reported difficulty responding to some survey items prior to surgery (especially scar), and this discouraged survey completion. Patients were recruited at the postoperative consultation (2–3 weeks following surgery) or via the 4-weekly multidisciplinary team meeting (where all new thyroid cancer diagnoses are presented postoperatively). Subsequent survey invitations were generated after a response to any survey item (scheduled at 3, 6, and 12 months). A lack of response at any time point resulted in no survey invitation being generated for the next time point.
HRQoL measures were selected after a review of the literature and included the generic Short Form-12 (SF-12), 33,34 a 12-item survey resulting in a physical component score (PCS) and mental component score (MCS); European Organisation of Research and Treatment of Cancer (EORTC-QLQ-C30), 35,36 a 30-item survey used widely in cancer survivorship studies of any tissue subtype; City of Hope Quality of Life–Thyroid Version (COH-TV), 37 a 41-item thyroid cancer-specific survey including physical, psychological, social, and spiritual domains; Thyroid Cancer Quality of Life (ThyCaQoL) Survey, 38 a 24-item thyroid cancer-specific survey including physical and psychological domains, designed to be administered alongside EORTC-QLQ-C30; Assessment of Survivor Concerns (ASC) Scale, 39 a five-item survey focused on fear of cancer recurrence; and Patient Health Questionnaire 4 (PHQ4), 40,41 an ultra-brief screening survey containing two items assessing each of anxiety and depression. Surveys were selected based on frequency of prior use and sensitivity to detect change, as well as to facilitate comparison with population normative data (SF-12), mixed oncology normative data (EORTC-QLQ-C30), and issues specific to thyroid cancer survivors. Precision analysis of global health status (EORTC-QLQ-C30) after 40 responses, and in comparison with available reference values, 42 suggested a minimum sample size of 80 participants to achieve a confidence interval.
The study protocol was prospectively approved by the Hunter New England (2019/ETH13770) and University of Newcastle (H-2021-0097) Human Research Ethics Committees.
Data analysis
Demographic, clinical characteristics, and survey responses at each time point were summarized using descriptive statistics. Due to variation in timing of participant recruitment and responses, time points for analysis were constructed based on the length of time after surgery (or day of recruitment for those choosing active surveillance). Where any participant had two responses within one time window, only the earliest response was included. Crude statistical comparisons were performed using Wilcoxon rank-sum tests, Pearson’s Chi-squared, and Fisher’s exact tests as appropriate.
Survey items were scored according to their relevant scoring manuals, reverse-scoring items as required, and followed recommended approaches to manage missing data. 34,36,38,39,43,44 For SF-12, PCS and MCS were constructed using the correlated method with scores normalized to the Australian population. 45 –48 p-Values representing tests of differences in survey scores over time were computed using linear mixed models, including a fixed effect for time after surgery (categorical variable with four categories) and a random intercept to account for repeated measures on participants. Two p-values for the effect of time are presented: the global p-value (corresponding to the overall effect of time allowing for the four nominal values) and a pairwise p-value comparing <3- and >12-month scores.
Multivariable models were fit to assess the association of patient demographic and clinical variables with patient responses to selected surveys. Outcomes for inclusion in multivariable models were selected based on a pairwise p-value <0.1. A multivariable model was also fit a priori for the total ASC score. A linear mixed model was used, including a random effect for participant to account for repeated measures, and prespecified patient variables (extent of surgery, American Thyroid Association [ATA] risk, age, sex, education, geography, insurance status, and need for thyroid hormone replacement) as fixed effects. Model assumptions were checked using plots of residuals and random effects. Robust standard errors were used to provide estimates robust to mild departures from model assumptions. Statistical significance was declared at 0.05. Multicollinearity was investigated to ensure levels were acceptable. 49 All analyses were performed using R Statistical Software (v4.1.2; R Core Team 2021). 50 –52
Results
Between January 2021 and June 2023, 111 (59%) patients completed at least one survey at one time point. Of the 76 nonresponders, 49 were unable to be contacted, 9 declined, 13 had no computer or email, 3 had insufficient English skills, and 2 had inadequate cognitive ability to answer surveys (Fig. 1). Participant characteristics are presented in Table 1. Most were female (72%), with mean age of 55 years. Responders reported smoking status (1 [1%] current, 41 [37%] previous, 68 [62%] never), educational status (15 [14%] did not complete high school, 67 [60%] completed high school or equivalent vocational qualifications, 29 [26%] university qualifications), and need for thyroid hormone replacement (n = 63 [57%]). Almost all patients underwent thyroid surgery (98%; 25% lobectomy only). Most patients had ATA low-risk disease (55%), and 58% received radioactive iodine. There was no significant difference in demographic, clinical, or treatment characteristics between survey responders and nonresponders. Comparison of responders >12 months and those lost to follow-up (after responding to at least one survey) revealed a higher loss to follow-up in metropolitan patients (p = 0.03), but no other significant differences.

Participant flow diagram. aOne participant did not complete surveys at the initial timepoint but had answered a single item and did complete subsequent surveys. bWhere any participant had more than two survey responses within one time window, only the earlies response was included.
Demographics of Participants, Stratified by Survey Response Status
Bold values indicate statistically significant p-values (defined as <0.05).
Wilcoxon rank sum test; Pearson’s Chi-squared test; Fisher’s exact test.
Modified Monash Medical Model 35 : an Australian population and socio-economic index. MM1 metropolitan centers include 70% of the Australian population. MM2-7 are regional with MM7 most remote. (Reference Versace).
BMI data available for only 56%.
Excludes two patients who did not have well differentiated thyroid cancer.
Low-dose is 1.1 GBq and high dose 3–4 GBq.
Lenvatinib is the only tyrosine kinase inhibitor available for thyroid cancer treatment in Australia and is restricted to those with RAI-refractory metastatic disease.
Missing values not presented in table.
ATA, American Thyroid Association; BMI, body mass index; RAI, radioactive iodine; SD, standard deviation; TSH, thyrotropin.
Short Form-12
SF-12 physical and mental component summary scales (PCS and MCS) and trends over time are presented in Figure 2. Despite improvement from <3 to >12 months in both PCS and MCS, mean scores for thyroid cancer survivors remained lower than population-normalized scores at all time points (<3, >3–6, >6–12, >12 months), with higher scores indicating higher HRQoL. The population-normalized score (mean [SD]) was 50 (10). PCS scores were: 35.9 (8.7), 38.4 (9.9), 38.6 (8.7), and 39.4 (8.4) at respective time points, global p = 0.12, pairwise p = 0.02; MCS scores were: 41.6 (9.2), 45.1 (11.5), 45.2 (10.5), and 46.7 (9.0) at respective time points, global p = 0.03, pairwise p < 0.01. MCS scores at 12 months returned closer to normalized scores (mean 46.7), and showed more consistent improvement (global p-value = 0.03). PCS scores remained lower at the end of the study (mean 39.4) and the global p-value did not reach statistical significance (p = 0.12). Regression modeling of factors associated with SF-12 revealed higher PCS in males (p = 0.01), and higher PCS (p = 0.01) and MCS (p < 0.01) with increasing time after surgery, but showed no relationship with extent of surgery, ATA risk, age, education, geography, health insurance status, or need for thyroid hormone replacement (Supplementary Table S1).
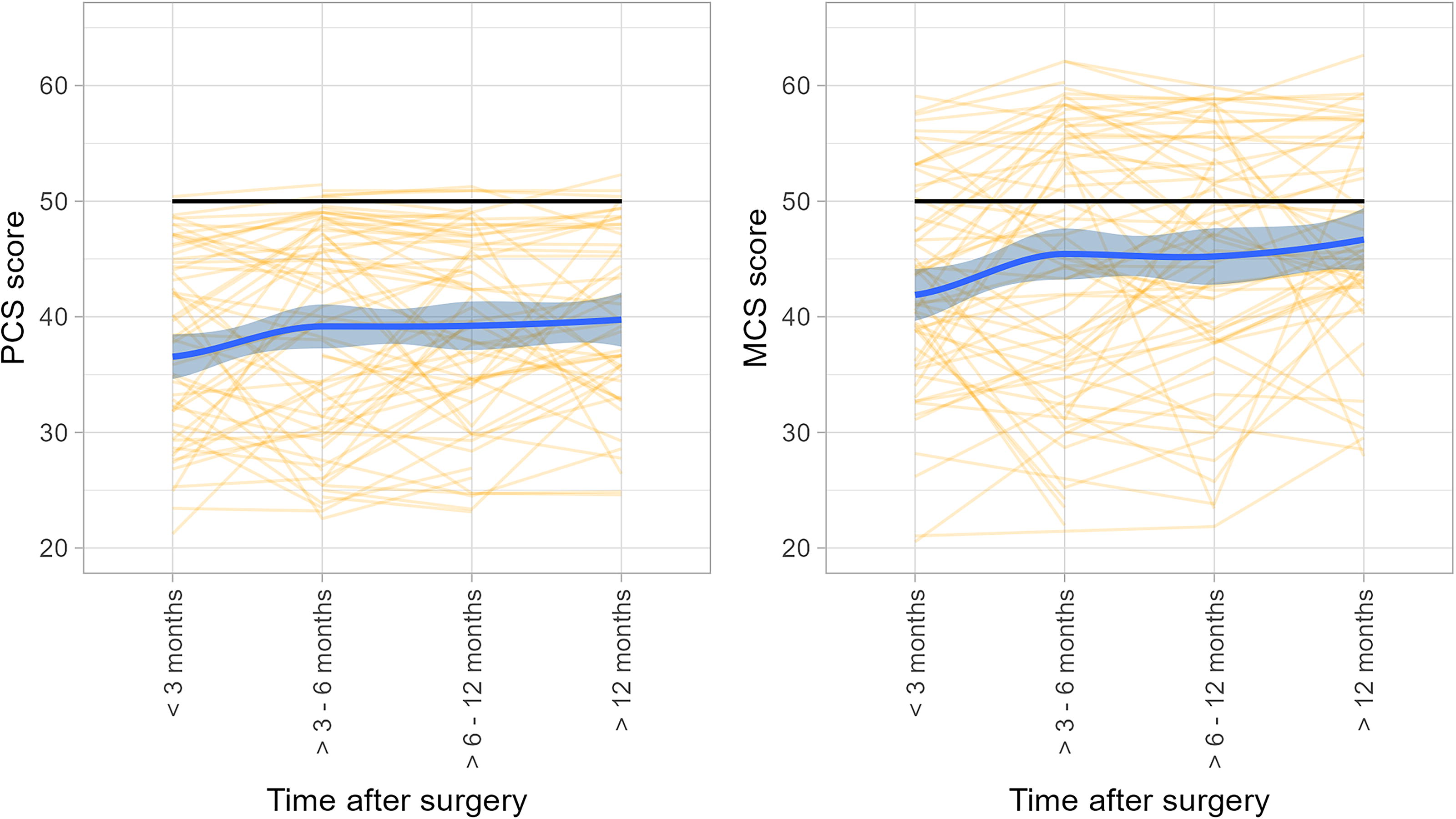
Trend over time in SF-12 physical component score (PCS) and mental component score (MCS). SF-12, Short Form-12.
EORTC-QLQ-C30
EORTC-QLQ-C30 scores and symptom scales over time are presented in Supplementary Table S2. There was no evidence of change over time for any scale (all global and pairwise p-values >0.05). Table 2 compares mean EORTC-QLQ-C30 scores and scales from >12-month time point to normative Australian values, 52 with clinical interpretation of effect sizes according to Cocks et al. 53 Compared with population data, thyroid cancer survivors reported lower scores (poorer HRQoL) for cognitive functioning (mean difference 10.8, medium effect size) and role functioning (mean difference 7.7, small effect size), and higher scores (more symptoms) related to fatigue, dyspnoea, insomnia, diarrhoea, and financial difficulties (mean differences 8.8, 4.6, 5.7, 6.5, and 4.7, respectively, all small effect size).
Comparison of EORTC-QLQ-C30 Mean Scores at >12-Month Time Point with Published Australian Population Normative Data 42
Example interpretation: for cognitive functioning scales, there was a mean difference of −10.8 (medium effect size), indicating lower HRQoL in thyroid cancer survivors at >12 months; the fatigue symptom scale revealed a mean difference of +8.8, indicating higher fatigue scales (worse HRQoL, small effect size) in thyroid cancer survivors.
Clinically important effect sizes according to Cocks et al. (not available for emotional functioning). 53
EORTC-QLQ-C30, European Organisation of Research and Treatment of Cancer; HRQoL, health-related quality of life.
Thyroid Cancer Quality of Life
ThyCaQoL items and scales over time points are summarized in Table 3. Statistically significant improvement was noted in voice (p < 0.01) and scar (p < 0.01) scales, but worsening was noted in neuromuscular (muscle/joint pain, leg cramps, feeling slowed down), global p < 0.01; and sensory scales (irritated eyes and skin), global p = 0.01; as well as reports of weight gain (global p = 0.03) (Fig. 3). Regression modeling to adjust for clinical and demographic variables confirmed improvement in voice and scar over 12 months (p < 0.01), but deterioration in neuromuscular (p < 0.01), sensory (p < 0.01), sympathetic (hot flushes, heat tolerance, p = 0.03), and psychological (p = 0.03) subscales (Table 3 and Supplementary Table S3). Lower participant age was associated with higher symptom burden (lower HRQoL) in scales related to concentration (p = 0.01), psychological (p < 0.01), and scar (p = 0.01). Male sex was associated with lower symptom burden (higher HRQoL) in domains related to neuromuscular (p = 0.02), sympathetic (p = 0.02), and sensory (p = 0.02); and less concern regarding weight gain (p = 0.04). High ATA risk was associated with worsening voice symptoms (p = 0.04), and university qualifications were associated with less neuromuscular symptoms (better HRQoL, p = 0.04). There were no significant associations between the symptom scales modeled and extent of surgery, geography, health insurance status, or need for thyroid hormone replacement.
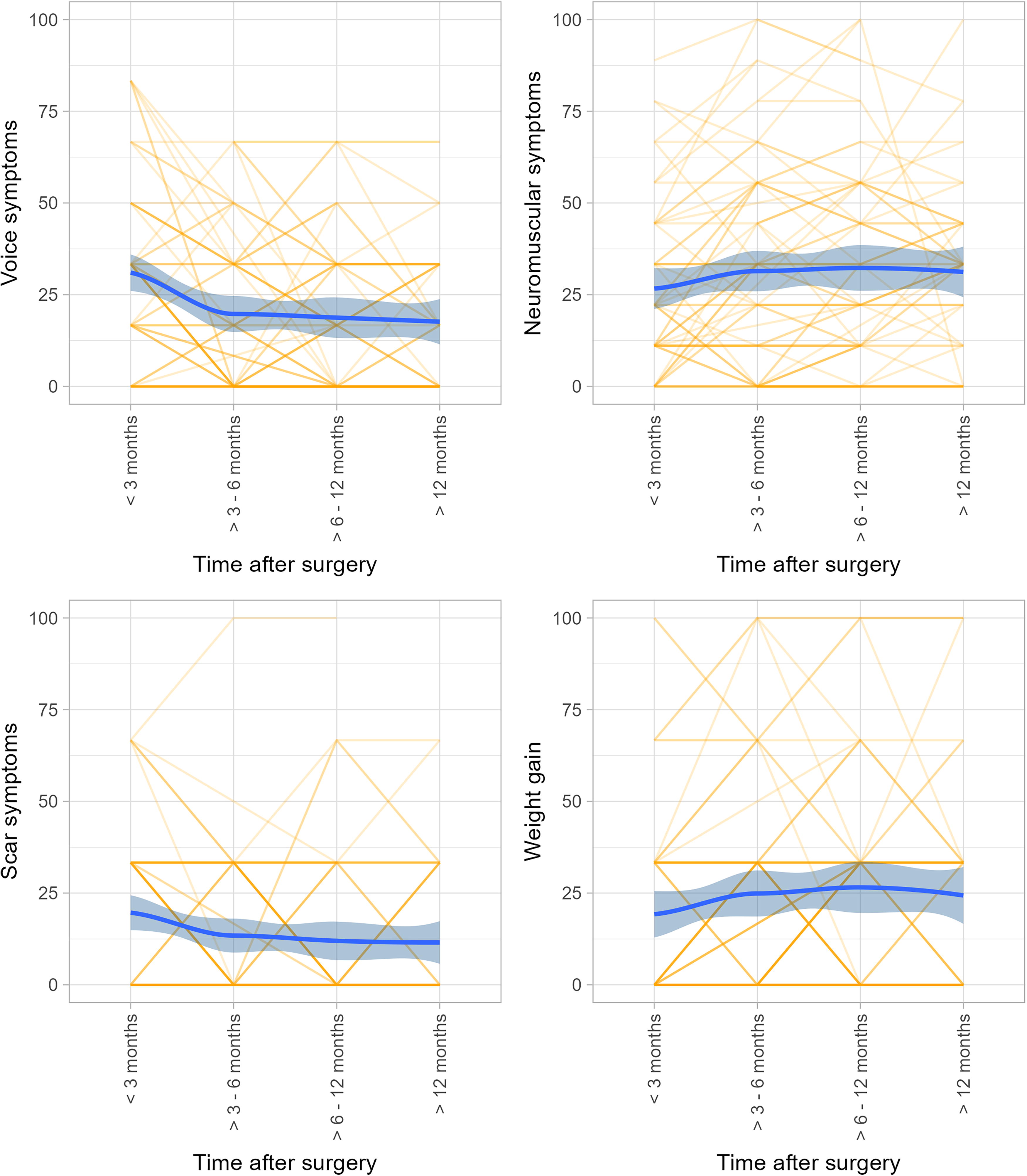
Graphical representation of change in ThyCaQoL symptom scores related to voice, neuromuscular symptoms, scar, and weight gain. ThyCaQoL, Thyroid Cancer Quality of Life Survey.
Summary of ThyCaQoL Individual Items and Scales
Bold values indicate statistically significant p-values (defined as <0.05).
Scale range 0–100; higher scores indicate higher symptom burden and lower HRQoL.
Mean (SD).
Mean (confidence interval). Regression modeling for change in ThyCaQoL <3 to >12 months after surgery performed where pairwise p-value <0.1. Example interpretation: With all other independent variables held constant, at >12 months following surgery a mean decrease in voice score of 13 (−18 to −7.5) is observed, reflecting less voice symptoms and higher HRQoL.
ThyCaQoL, Thyroid Cancer Quality of Life Survey.
City of Hope
No significant change over time was seen in COH-TV (score range 0–10, where higher scores reflect greater HRQoL) in total mean scores (6.5 < 3 months to 6.88 > 12 months, pairwise p = 0.31) or in any subdomain: physical (7.76 to 7.86, p = 0.26), psychological (6.43 to 6.92, p = 0.58), social (7.64 to 8.22, p = 0.35), or spiritual (4.22 to 3.75, p = 0.20).
Assessment of Survivor Concerns
Marked individual variation in ASC responses (assessing fear of cancer recurrence) was seen, but no statistically significant change in mean scores over time (global p = 0.86) (Fig. 4 and Supplementary Table S4). Of note, mean scores >12 months were 11.3 (3.4), indicating that some degree of fear of cancer recurrence was reported by most, with some individuals reporting severe fear. Regression modeling was performed for total ASC scores, with only younger age being significantly associated with fear of cancer recurrence (p < 0.01) (Supplementary Table S5). In this model, for each 10-year decrease in age, the ASC score increased (greater fear of cancer recurrence) by 1.3 (0.8–1.8).
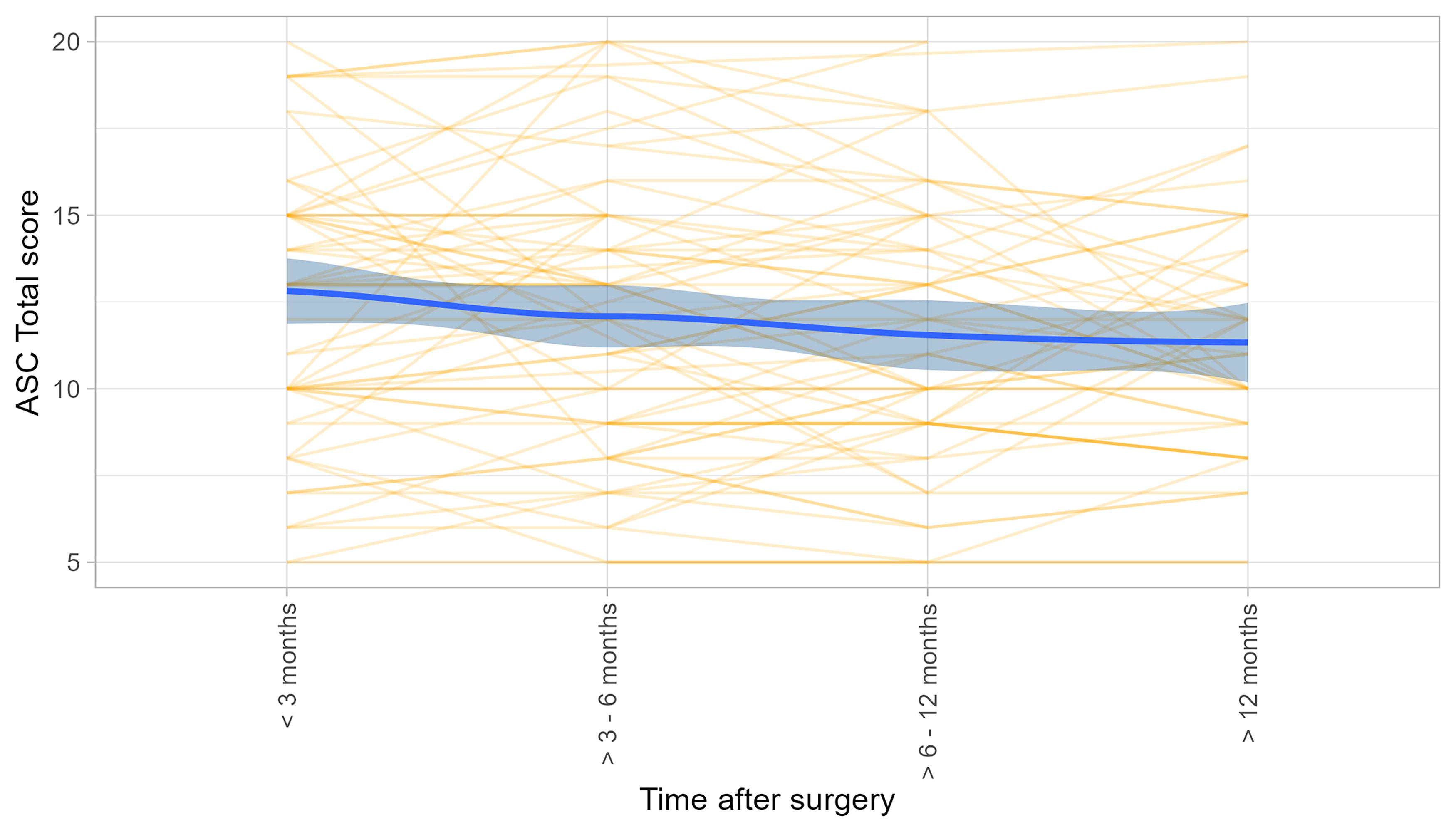
Trend over time in Assessment of Survivor Concerns (ASC) total score.
Discussion
These data map the trajectory of HRQoL changes of an Australian cohort of thyroid cancer survivors 12–18 months following diagnosis. In contrast to much of the prior published literature, participants were selected by their geography rather than being from a single medical center or self-selected survivorship group. By utilizing multiple tools with repeated measures over time, comparisons with normal population data were made, and the nuances of disease-specific symptoms were studied side by side. Of key importance is the SF-12 data showing that, despite improvements in PCS and MCS subscales over 12 months, on neither scale do thyroid cancer survivors return to normative population HRQoL values. This is independent of age, cancer stage, extent of surgery, education, health insurance status, or the need for thyroid hormone replacement. Only male sex was associated with higher (better) HRQoL scores.
HRQoL in comparison with population norms
Prior thyroid cancer survivorship studies using generic surveys have shown mixed results. While most identify short-term HRQoL deficits, in many cases mean results return to baseline. 54 The use of SF-36 and SF-12 seems to be more sensitive, with multiple authors reporting long-term small deficits in thyroid cancer survivors compared with population data. 18,55 –60 In this study, we have used the correlated method to calculate SF-12 scores. This method is more sensitive to HRQoL changes over time in an Australian population and is recommended over routine use of scoring manuals. 45 –48 Country-specific comparative data were used to interpret EORTC-QLQ-C30 scores and identified deficits in cognitive functioning, fatigue, insomnia, role functioning, dyspnoea, diarrhoea, and financial difficulties. While these findings are consistent with reports in other thyroid cancer survivorship studies, 13,57,61,62 the use of country-specific data further assists with determining effect sizes, which is essential to understanding clinical significance. This facilitates focus on HRQoL priorities, interventions, and their assessment for the target population. Based on the data from this study, we recommend future HRQoL studies in thyroid cancer survivors carefully choose HRQoL tools with proven sensitivity and utilize comparative, normative population data to determine clinically significant changes.
Thyroid cancer-specific HRQoL
The use of disease-specific scales is necessary, as thyroid cancer survivors experience unique HRQoL changes, 29 including voice, scar, weight gain, and dry eyes/mouth. While voice and scar symptoms did improve, the individual variation was apparent, with many patients still reporting concerns more than a year after surgery. These data are consistent with prior studies suggesting that persisting voice symptoms are common, even in the absence of nerve injury, and that surgeons need to be realistic with patients about the time course and individual variation in voice recovery. 30,63,64 Of more concern, some symptom scores worsened in the 12 months following surgery, including muscle/joint pain, weight gain, cramps, dry eyes and skin, and concentration. These symptoms were not clearly correlated with thyroid function nor the need for levothyroxine replacement. It is beyond the data presented to postulate the mechanisms behind these changes, but they are concordant with literature reporting persisting patient concerns that prevent re-engagement in work and social activities. 16,26,65 Patients report that these issues are infrequently addressed by current clinical information resources, 66 that persisting symptoms are often dismissed by clinicians, and that pathways for self-help are rarely available. 30,67 Further research should focus on interventions that may lessen symptom distress for those impacted and improve information and self-efficacy resources, all with the aim of optimizing well-being.
At the time of inception of this study, only two thyroid cancer-specific tools had been validated through Phase IV testing. COH-TV was the only survey to include all four of Ferrell’s HRQoL domains (physical, psychological, social, and spiritual well-being) 37,68 but was also the longest survey included in this study. Despite 41 items and 4 subdomains, the COH-TV provided minimal evidence of change over 12 months. In contrast, ThyCaQoL provided meaningful data regarding voice, scar, as well as symptoms related to weight gain, flushing, and cramps. These symptoms were also highlighted in the qualitative data aligned with this study. 30 The newer Thy34 module 69 is also designed to be administered alongside EORTC-QLQ-C30. It underwent extensive international testing during a robust development process and may become the preferred disease-specific tool for thyroid cancer. 69 –71 It is yet to be extensively tested within an Australian context.
Fear of cancer recurrence
Fear of cancer recurrence has been heterogeneously studied in the thyroid cancer literature. 19 Younger age was associated with higher levels of fear of cancer recurrence, a finding consistent with both the wider oncology literature and that specific to thyroid cancer. 72 –74 This is a particular paradox for thyroid cancer survivors where, despite generally improved prognosis in participants with younger age, fear of cancer recurrence is greater in youth. 20 Furthermore, fear of cancer recurrence does not improve significantly over time and can be a significant driver of poor HRQoL. 19,75,76 There is evolving research regarding screening for fear of cancer recurrence 77,78 in clinical practice, allowing interventions to be targeted for those at risk. 79 It is imperative that fear of cancer recurrence be studied in thyroid cancer survivorship research.
Limitations and strengths
The data of this study should be interpreted within its limitations. Despite inviting all patients of a geographic region (metropolitan and regional centers) to participate, sample size was limited by patient eligibility, ability to contact, and consent. A wider population could have been studied with a multisite trial, but ensuring accurate clinical follow-up and minimizing selection bias would have proved more difficult. As patients were recruited postoperatively, it is unlikely that we have captured the distress associated with initial diagnosis. Recruitment was enhanced after a naturalistic opportunity to evaluate methods was provided by the COVID-19 pandemic, 29 and response rates (to at least a single survey) were 59%. While this is lower than some studies from academic centers or survivorship groups, it is reflective of the “real-world” nature of research in unselected populations. 80,81 Survey burden was also significant and could have contributed to lower response rates. However, despite any time point including up to seven surveys, few failed to complete surveys once commenced. 29 We acknowledge that the results of this study should be interpreted with the limitations of the response rate at each time point.
A strength of this study was inclusion of patient data from multiple surveys administered repeatedly over 12–18 months following thyroid cancer diagnosis in a population of patients broadly representative of their community. This allowed HRQoL comparisons with normative population data while ensuring the nuances of thyroid cancer survivorship remain documented. Based on our data, we would suggest that future studies of thyroid cancer survivorship include at least one generic survey, a thyroid cancer-specific survey, and a validated fear of cancer recurrence tool. Survey selection should consider country-specific performance of tools.
Clinicians should be aware that patients may experience significant distress from persisting symptoms and that fear of cancer recurrence is common and does not ameliorate over time. These issues can prevent return to normal functioning. Future research should focus on identifying those at risk of persisting symptoms affecting HRQoL and developing and evaluating interventions for these target groups that improve well-being. In the meantime, clinicians should recognize and acknowledge patient distress, encourage self-efficacy, and facilitate pathways for supportive care.
Conclusion
Thyroid cancer survivors experience significant individual variation in HRQoL. Collectively, deficits persist beyond 12 months after surgery and prevent return of HRQoL to population norms. Future thyroid cancer survivorship studies should focus on identifying, acknowledging, and addressing persisting symptoms with the aim of optimizing holistic well-being.
Footnotes
Acknowledgments
The authors would like to acknowledge Dr. Shaun McGrath, A/Prof. Cino Bendinelli, Dr. Daron Cope, Dr. Kathleen Soeyland, Dr. Linda Fenton, Dr. Frank Sardelic, and A/Prof. Rob Eisenberg who contributed patients to this study. Thanks also Dr. Elvina Wiadji, Rosemary Carroll, Prof. Stephen Smith, Dr. Nicholas Blefari, Paula Bridge, Sarah Morris who contributed to research co-ordination and oversight for this study.
Authors’ Contributions
C.J.O.: Conceptualization and methodology (equal), data curation (equal), resources (equal), funding analysis (equal), project administration (equal), formal analysis (equal), visualization (equal), original draft (lead), and reviewing and editing (equal). C.W.R.: Conceptualization and methodology (equal), resources (equal), data collection (supporting), and reviewing and editing (equal). H.M.-B.: Data collection (equal), validation (equal), and writing—reviewing and editing (equal). M.A.C.: Data collection (equal), project administration (equal), and writing—reviewing and editing (equal). S.L.: Software, visualization (equal), formal analysis (equal), writing—original draft (equal), and writing—reviewing and editing (equal). T.C.-M.: Supervision (equal), data collection (supporting), verification (equal), and writing—reviewing and editing (equal). E.H.: Resources (equal), funding acquisition (equal), supervision (equal), and writing—reviewing and editing (equal). E.A.F.: Conceptualization and methodology (equal), resources (equal), data collection (supporting), and writing—reviewing and editing (equal). C.L.P.: Resources (equal), data collection (supporting), funding acquisition (equal), formal analysis (supporting), and writing—reviewing and editing (equal).
Author Disclosure Statement
The authors state that they have no conflicts to disclose.
Funding Information
This study was supported by grants from Hunter Cancer Research Alliance and Hunter Medical Reserach Institute Surgical and Perioperative Care Research Group.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
Supplementary Table S5
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.