
Abstract
Background:
Anaplastic thyroid cancer (ATC) has historically been almost uniformly fatal. In patients with the loco-regional disease (stage IVB), multimodal therapy (upfront surgery when feasible, radiation +/- concurrent chemotherapy) followed by observation is the current standard of care.
Methods:
Stage IVB ATC patients treated with multimodal therapy, followed by adjuvant pembrolizumab were studied. Data were combined from a prospective, phase 2 trial that closed early due to poor accrual, and a retrospective cohort of consecutive patients who received adjuvant pembrolizumab, mirroring the trial eligibility criteria. Patients received adjuvant pembrolizumab starting within 6 weeks after completion of radiation. An age and treatment-matched control arm treated with multimodal therapy without adjuvant pembrolizumab was selected for comparison. The primary objectives included median progression-free survival (PFS) and recurrence rate, and the secondary objective was median overall survival (OS).
Results:
Sixteen patients were included in each arm. The median age in both groups was 59 years. The median PDL1 score in the adjuvant pembrolizumab arm was 50% (range, 0–95%). The majority (88%) had upfront surgery in both groups. The median follow-up time was 24.3 months in the adjuvant arm and 56.7 months in the control arm. The median PFS in the adjuvant and control arm was not reached, and 5.4 months [CI: 2.04–16.20], respectively (p = 0.006; HR 0.24 [CI: 0.08, 0.73]). The median OS was not reached in the adjuvant pembrolizumab group. In the control group, the median OS was 31 months [CI: 13.9, NA] (p = 0.009; HR 0.11 [CI: 0.01, 0.83]). The 12-and 24-month survival rates were 80% [CI: 0.51–0.93] and 52% [CI: 0.25–0.74], respectively, in the control arm, whereas all patients in the adjuvant arm were still alive at 1- and 2-years.
Conclusion:
Adjuvant pembrolizumab appears to be a safe and effective strategy to prevent recurrences and prolong survival in stage IVB ATC patients following multimodal therapy. Confirmatory studies are needed.
Introduction
Until recently, a diagnosis of anaplastic thyroid cancer (ATC) was considered uniformly fatal. However, the past decade has ushered in a number of systemic therapies and treatment approaches which have shown efficacy in these patients. 1 –5 Patients with stage IVA (tumor confined to the thyroid) or IVB (loco-regional disease) have a far better prognosis than patients with distant metastatic disease (stage IVC) when treated with multimodal therapy. Traditional multimodal therapy consists of upfront surgery when feasible, radiation plus concurrent cytotoxic chemotherapy, followed by observation. This is the current standard of care included across all guidelines for non-BRAFV600E -mutated stage IVA/B ATC. 6 –8 However, relapse rates are high with multimodal treatment, likely due to microscopic metastatic disease, highlighting the need for effective adjuvant therapy. The Mayo Clinic group reported a 12- and 24-month overall survival (OS) of 68% and 48%, respectively, in this population. Relapses carry a very high risk of mortality, as 42% of patients died within 6 months. 9
In ATC, the Programmed Cell Death Protein 1 (PD-1) receptor-ligand interaction is a major pathway hijacked by tumors to suppress immune control and most ATC tumors express Programmed Cell Death Ligand 1 (PD-L1). 10 –12 Pembrolizumab, an anti-PD1 checkpoint inhibitor, blocks the interaction of PD1 and PDL1, resulting in an anti-tumor immune response. Thus, we hypothesized that adjuvant pembrolizumab would provide a local control benefit, in addition to targeting microscopic metastatic disease.
Methods
Patients with stage IVB ATC who were undergoing or had completed upfront multimodal therapy were given consideration for a prospective, phase 2 trial with adjuvant pembrolizumab (NCT05059470), called IMPAACT (“intensity-modulated radiation [IMRT] followed by pembrolizumab in the adjuvant setting in anaplastic cancer of the thyroid”). Unfortunately, the trial closed early due to poor accrual. Subsequently, a new study combining the data from six patients treated in the IMPAACT prospective trial with a retrospective cohort of consecutive stage IVB ATC patients who received adjuvant pembrolizumab outside of the trial was created. A 1:1, age- and treatment-matched historical group of patients with stage IVB ATC was selected as the control group. Informed consent was obtained for each patient on the IMPAACT prospective clinical trial, and an institutionally approved waiver of consent was in place for the patients in the retrospective trial. The protocols and amendments were approved by the institutional IRB. Both studies were performed in compliance with Good Clinical Practice guidelines and in accordance with the Declaration of Helsinki.
The retrospective cohort of patients treated with adjuvant pembrolizumab was chosen by using criteria that mirrored the trial eligibility criteria for IMPAACT. Eligibility criteria included: stage IVB ATC, completion of multimodal therapy (surgery when feasible and external beam radiation to the neck with or without concomitant cytotoxic chemotherapy), and adjuvant pembrolizumab within 6 weeks (+2 weeks allowed to account for latent toxicity resolution) after the completion of radiation. As this was an intention-to-treat analysis, patients who were thought to have stage IVB disease due to small, [18F]Fluorodeoxyglucose-PET scan equivocal lesions who were later identified as having metastases were included. Pembrolizumab dosing in the IMPAACT trial was 400 mg IV every 6 weeks. Patients outside of the trial could have received 400 mg every 6 weeks or 200 mg every 3 weeks. For patients receiving infusions every three weeks, treatment cycles were defined as six-week periods, with each cycle consisting of two infusions. Patients in the clinical trial were planned to receive pembrolizumab for 1 year with an optional 2nd year per patient and physician discretion.
Patients in the historical control arm were selected from our IRB-approved ATC database. Those having received adjuvant immunotherapy during radiation or adjuvant treatment after radiation therapy were excluded. Patients were observed off all treatment after the completion of multimodal therapy, which is the current standard of care. These patients were matched 1:1 by stage, age at diagnosis (matched within ±5 years of age), and by upfront treatment, specifically, by the extent of surgery (R0/R1 vs. R2) and dose of radiation (≥45 Gy vs. <45 Gy radiation). No patients prior to 2014 were selected.
The primary objectives of this trial were to estimate the recurrence rate and median progression-free survival (PFS) in patients with stage IVB ATC who treated with adjuvant pembrolizumab after the completion of initial standard therapy and compare them to the age- or treatment-matched historical control group. PFS was determined by using the start date of pembrolizumab (for adjuvant-treated patients) or end of radiation (for historical control patients), to the last radiographical assessment of progression or date of death. A secondary objective was to estimate and compare the median OS in the two cohorts, using the same starting dates as PFS.
RECIST v1.1 was used to evaluate relapses. For the efficacy endpoints, OS, and PFS, the Kaplan–Meier method was used to estimate their survival functions. The marginal comparisons in PFS and OS were performed using the log-rank test. The Cox regression model was used to estimate the hazard ratio (HR) of using adjuvant pembrolizumab, stratified by the matching factors of age and treatment.
Results
Treatment groups
A total of 16 patients between March 2020 and February 2024, were included in the adjuvant pembrolizumab group, and an equal number of historical control patients between May 2014 and January 2024. Figure 1 shows the flowchart for adjuvant pembrolizumab case selection. Seven of the excluded patients in the retrospective series received adjuvant pembrolizumab outside of the allowable 6-week post-radiation window (range 9.1–27.8 weeks; two patients have died of progressive disease and one is alive but relapsed; four are alive and have no evidence of disease). One patient who started adjuvant pembrolizumab within the allowable window was excluded due to lack of information, as he was treated and followed outside but was alive >2 years after the start of adjuvant pembrolizumab.

Case selection flow diagram for the adjuvant pembrolizumab cohort. Data from a prospective clinical trial (NCT 05059470) were combined with real-world, retrospective cases using entry criteria that mirrored the trial eligibility criteria. ATC, anaplastic thyroid cancer.
Table 1 shows the baseline characteristics of the included adjuvant pembrolizumab and control groups. Six (34%) of the adjuvant pembrolizumab patients were accrued in the IMPAACT trial, while 10 (63%) were identified from the retrospective study. Both arms were well-balanced in terms of age, sex, and extent of surgery. One patient in each group did not undergo upfront surgery. All patients in the historical control arm received IMRT ≥45 Gy and concomitant radiosensitizing chemotherapy. In the adjuvant pembrolizumab arm, all but one received IMRT ≥45 Gy with radiosensitizing chemotherapy. The patient who received lower dose radiation, underwent urgent palliative radiation (30 Gy in 10 fractions) using 3-dimensional conformal radiation to the intact tumor, without radiosensitizing chemotherapy.
Baseline Patient Characteristics
T and N stage were based on AJCC version 8. T stage included pathological measurements, preferably, but when these were not available, radiological measurements were used. N stage included only pathological information on nodal disease (biopsy or excisional).
T stage “N/A” refers to anaplastic transformation patients with previous thyroidectomy for differentiated thyroid carcinoma.
RT, radiation therapy; Gy, Gray.
Mutation and PDL1 analysis
All patient tumors were sent for molecular analysis. Only one patient’s tumor (in the adjuvant pembrolizumab arm) could not be genotyped due to a very high immune infiltrate. Thus, 15/16 (94%) of the adjuvant arm tumors were evaluated by Next Generation Sequencing (NGS) for mutations and 13/16 (81%) were evaluated for RNA fusions. In the matched historical control arm, all (100%) patient tumors were evaluated by NGS for mutations; 9/16 (56%) were evaluated for RNA fusions. Figure 2 shows the oncoprint with patient characteristics and NGS data. In summary, there were more RAS mutations identified in the adjuvant pembrolizumab group (6/15, 40%) compared with the matched controls (3/16, 18%). Otherwise, there were similar numbers of driver oncofusions and mutations in BRAFV600E and PTEN. The median tumor mutation burden was 3 mut/Mb (range, 0.5–29) but there was insufficient aggregate information in the matched controls due to the historical nature of this group. The median PDL1 (Clone 22C3, Dako PharmDx) Tumor Proportion Score was 50% (range, 0–95%) in the 15 patients whose tumors were tested in the adjuvant pembrolizumab arm. Insufficient aggregate data for PDL1 was available in the matched control arm.
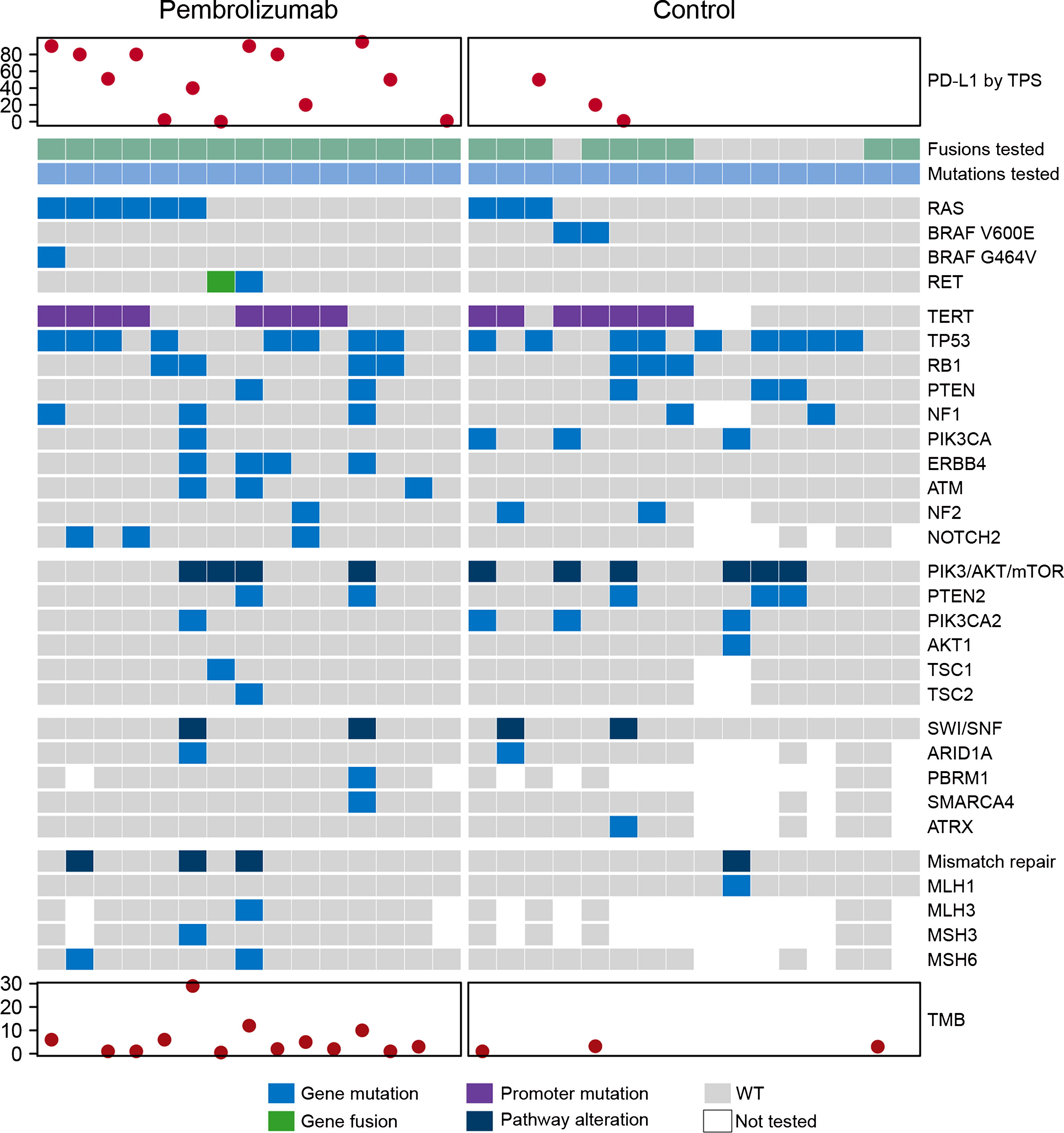
Oncoprint of targeted somatic gene mutations by Next-Generation Sequencing of tumors in patients with stage IVB Anaplastic Thyroid Cancer (ATC) in the adjuvant pembrolizumab and historical control arms. Several Clinical Laboratory Improvement Amendments (CLIA)-certified panels were used to assay for mutations in oncogenes of ATC tumors, including liquid biopsy (shown in figure). One patient with BRAFV600E positive immunohistochemistry, who was in the adjuvant pembrolizumab arm, is not included in the oncoprint because a mutation profile was not possible on his tumor.
Efficacy results
For patients who are still alive, the median follow-up was 21.2 months (IQR: 19.0–31.6) in the adjuvant pembrolizumab group and 39.9 months (IQR: 20.6–56.7) in the control group. In the adjuvant pembrolizumab group, patients received a median of 16 cycles (normalized to 6-week cycles for the analysis; range 1–19 cycles) of pembrolizumab. At the data cut-off, only two patients were in active treatment with pembrolizumab. These two patients had completed 11 and 16 cycles of pembrolizumab.
There were 3/16 (19%) patients who were counted as having recurrence in the adjuvant pembrolizumab group and 14/16 (82%) in the matched control arm (p ≤ 0.001). All three patients in the adjuvant pembrolizumab arm relapsed at distant sites, however, in retrospect the metastatic lesions were all present at the time of starting pembrolizumab (Supplementary Data). These metastatic lesions were considered non-specific at the time of diagnosis and are discussed below. One patient treated with adjuvant pembrolizumab died after 2.74 years without having experienced progression.
The median PFS was not reached in the adjuvant pembrolizumab arm but 5.4 months [CI: 2.04, 16.20; p = 0.006] in the matched control arm. The estimated HR was 0.24 [CI: 0.08, 0.73]. Using a 1:1 matched control design, a sample size of 16 patients per arm provided at least 90% power to detect a difference in 1-year PFS of 81% vs. 30% using a two-sided 5% significance level. The median OS was not reached in the adjuvant pembrolizumab groups. In the control group, the median OS was 31 months [CI: 13.9, NA; p = 0.009]. The estimated hazard ratio was 0.11 [CI: 0.01, 0.83]. At 1 and 2 years, all patients were alive in the adjuvant pembrolizumab arm, whereas 81% [CI: 0.53, 0.95] and 54% [CI: 0.27, 0.75] were alive in the matched control arm, respectively. Figure 3 shows the PFS (Fig. 3A) and OS (Fig. 3B) Kaplan-Meier curves, and the swimmer’s plot (Fig. 3C) of patients in the adjuvant pembrolizumab and historical control arms.
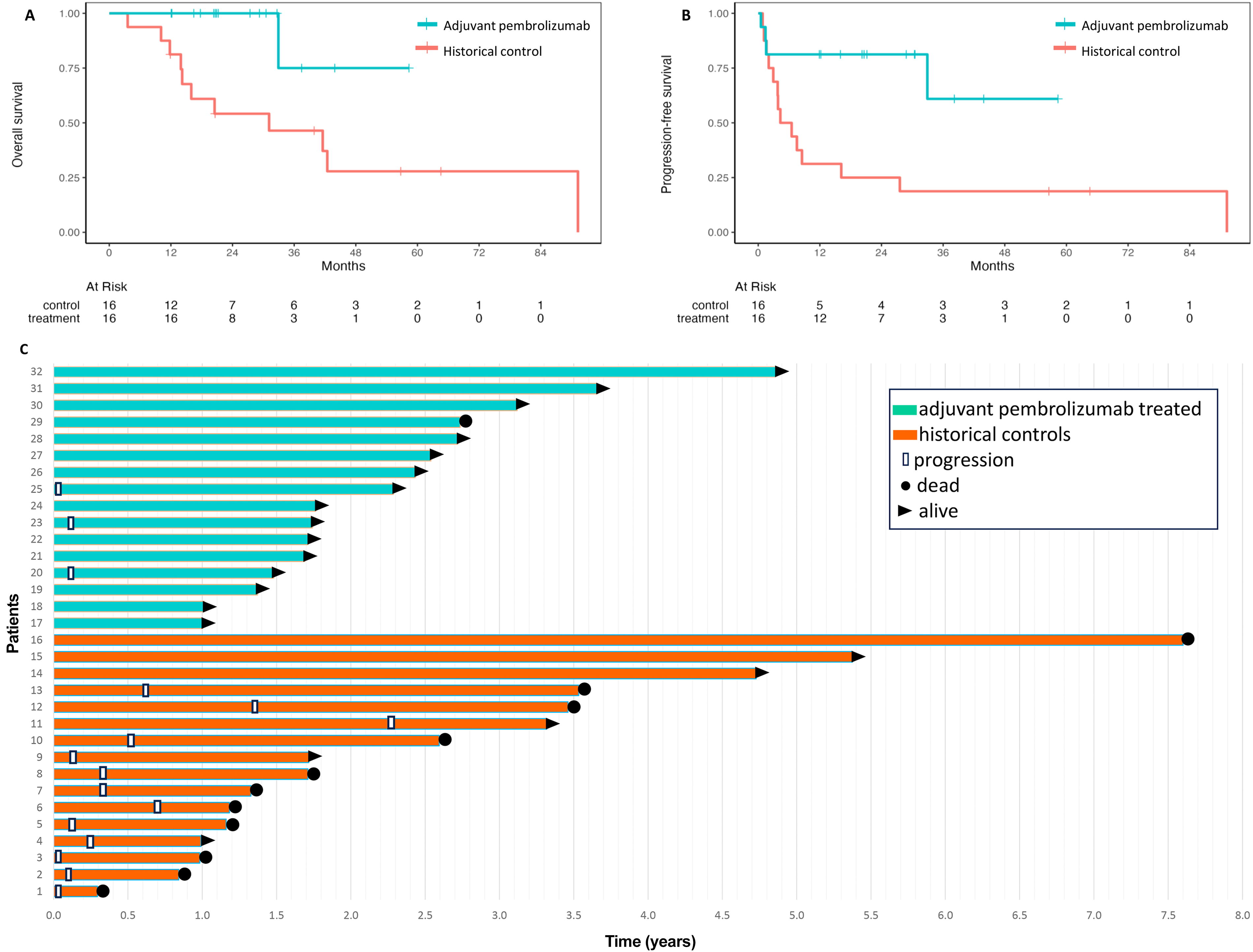
Median progression-free (3A) and overall survival (3B) in the adjuvant pembrolizumab cohort versus matched historical controls of stage IVB ATC patients. (3C) Swimmer’s plot showing the time in years from completion of radiation to progression and survival in stage IVB patients treated with adjuvant pembrolizumab or no adjuvant treatment. All patients, with the exception of patient 32, had upfront surgery prior to radiation. This patient had palliative radiation (30 Gy) to gross disease before starting adjuvant pembrolizumab. Relapses in the historical control group were due to distant metastatic disease in 79% of the 14 patients who relapsed (10/14 patients had distant relapse, 1/14 had both distant and locoregional relapse, and 2/14 had locoregional relapse).
In terms of serious adverse events (SAE) in the adjuvant pembrolizumab arm, grade 2 pneumonitis was reported in one patient. The patient was treated with steroids and pembrolizumab was permanently discontinued after four cycles. It was unclear if the SAE in the patient who died after developing gastric ischemia was related to pembrolizumab. The patient had chronic lymphocytic leukemia and was also taking acalabrutinib. He was admitted to an outside hospital with a diarrheal illness and found to have an ischemic injury to his stomach leading to sepsis and death. No other SAE were identified.
Discussion
This is the first study with adjuvant pembrolizumab for 1–2 years in stage IVB ATC. We found that the patients treated with adjuvant pembrolizumab within 4 weeks after completing multimodal therapy had a significantly longer median PFS and OS compared with the historical, age- and treatment-matched control patients who were observed after upfront multimodal therapy. The median PFS and OS have not been reached in the adjuvant pembrolizumab-treated group with a median follow-up time of 2 years. The only recurrences within the adjuvant pembrolizumab group were found to have been present prior to the first dose of adjuvant pembrolizumab. Even so, the recurrence rate was much lower in the adjuvant pembrolizumab patients, and these recurrences were ultimately deemed to be progressions of prior indeterminate lung lesions.
There are several clinical trials in ATC showing that the outcome of patients with locoregionally confined diseases (M0) is far superior to those with distant metastatic disease (M1), however, all of these demonstrate that the vast majority of patients with locoregionally confined disease relapse or die within 1–2 years of their diagnosis, despite surgery and radiation. 9,13,14 The NRG Oncology RTOG 0912 clinical trial with adjuvant pazopanib versus placebo subanalysis showed that in patients with M0/MX status, median survival in the placebo arm was 8.6 months [CI: 4.9, 16.2]. 14 By the 2nd year, only 4/21 (19%) patients in the placebo arm were still alive. However, these patients are not directly comparable to our historical control population due to differences in the surgical extent, which influences survival significantly. A retrospective study from MD Anderson showed that the median time to failure in stage IVB patients was 6.2 months and median OS was 12.3 months, 13 however, only 41% had been treated with upfront surgery. Despite this, within 2 years almost all patients had relapsed and/or died.
A retrospective study from the Mayo Clinic of stage IVB patients from 2003 to 2015 with multimodal therapy showed that at 1 and 2 years, 68% and 48% were alive, respectively, compared with our current trial’s historical cohort at 80% and 52%, respectively. In the Mayo cohort 19/22 (86%) patients had relapsed within the first 2 years after completion of multimodal therapy. Similar to our historical cohort, the majority (17/19 or 89%) of these patients relapsed at distant sites. At 5 years, 20/22 (91%) patients had relapsed. The difference between our historical cohort (31 months) and the Mayo cohort (22 months) is possibly due to better salvage therapies in more recent years because we only selected patients who presented after 2014. Our patients would have had access to more modern treatments such as BRAF/MEK inhibitors, lenvatinib/pembrolizumab, and clinical trials. This could explain the improvement in 1-year survival, however, at 2 years the MD Anderson and Mayo historical cohorts appear equivalent. This highlights the need for an adjuvant therapy to address micrometastatic disease. In our current study, the patients treated with adjuvant pembrolizumab seem to have far better outcomes than both the MD Anderson and the Mayo Clinic historical cohorts, with no patients having true progression and only one death which was not due to ATC recurrence. Longer follow-up is needed to determine if disease recurrences will appear after 1–2 years of adjuvant pembrolizumab treatment. ATC patients likely need at least 5 years of follow-up to understand whether they are cured.
All patients in the control arm and all but one in the adjuvant pembrolizumab arm had upfront surgery. More data are needed on the outcomes of patients who receive palliative radiation (i.e., <45 Gy) without upfront surgery, followed by adjuvant pembrolizumab, as many patients do not undergo surgical resection either due to unresectable disease or unacceptable surgical morbidity. On the other hand, if adjuvant pembrolizumab after upfront multimodal therapy is found to be curative, it may be time to consider performing more radical surgeries in otherwise healthy patients with non-BRAF-mutated stage IVB disease, similar to mucosal squamous cell carcinoma patients and in situations where checkpoint inhibitor therapy is possible.
Tumor driver mutation is important for determining prognosis in patients with ATC. The presence of a somatic BRAFV600E mutation, which is actionable with BRAF/MEK inhibitor therapy, is associated with a far better prognosis than RAS mutations. 15 Since BRAFV600E -mutated ATC patients usually undergo neoadjuvant BRAF/MEK inhibitor/anti-PD1 inhibitor, only one patient with BRAFV600E -mutated ATC was included in the treatment arm. Thus, it is unclear if the strategy of adjuvant pembrolizumab alone is sufficient for the BRAFV600E -mutated ATC patient. At this time, we continue to treat BRAFV600E -mutated patients with neoadjuvant and adjuvant dabrafenib/trametinib/pembrolizumab. 16 In our study, there were more patients with RAS-mutated tumors in the adjuvant pembrolizumab arm, thus favoring the control arm since RAS mutations are associated with far worse outcomes than BRAF-mutant ATC. 15 There was no difference in the number of patients with actionable mutations or fusions in the control versus adjuvant pembrolizumab groups. TMB and PDL1 scores were as expected in the adjuvant pembrolizumab arm but there was insufficient data in the control group, as many NGS panels did not include TMB, and testing for PDL1 score was not part of our standard practice prior to 2018.
The only serious adverse event that was clearly related to the pembrolizumab group was pneumonitis, a known adverse effect of the checkpoint inhibitors. Immune-related adverse events associated with these drugs can be life-threatening and warrant careful follow-up prior to each infusion. Another patient died 4 months after the last pembrolizumab infusion due to gastric ischemia/sepsis but it is unclear if this was a related event.
Unfortunately, the prospective clinical trial, IMPAACT, closed early for poor accrual, therefore we pooled data from the IMPAACT trial and from consecutive ATC patients who were treated “off-label” with adjuvant pembrolizumab. A number of factors could have contributed to the poor accrual to the trial. First, the trial was opened to enrollment in 2021, during the COVID-19 pandemic which severely slowed accrual. Second, pembrolizumab is commercially available in the United States and many physicians treat their patients outside of clinical trials for the convenience of the patient. Therefore, we combined data from the prospective clinical trial with real-world data in patients treated similarly. In order to determine whether the adjuvant treatment group benefitted from pembrolizumab, we created an age and treatment-matched cohort. However, questions remain regarding the efficacy of adjuvant pembrolizumab in patients with unresectable disease who undergo radiation to gross disease, as few patients were treated in our study. Other questions remain regarding adjuvant pembrolizumab treatment of patients with stage IVA disease.
The major limitations of this study include the largely retrospective nature and the small number of patients; however, this is expected given the rarity of ATC. We acknowledge that retrospective trials can introduce bias, however, we mitigated this by adding an age- and treatment-matched control group and included patients who had indeterminate lesions which only later were clearly metastatic disease. The feasibility of initiating and enrolling a multi-center, randomized clinical trial in a rare and aggressive cancer is a major problem, due to the time and expense needed to enroll and the acceptance of a control arm; therefore, novel observational studies could be an alternative to randomized trials in ATC in the future, such as the Master Observational Trial, 17 which recently opened at our institution (NCT06507878). Another limitation is the lead-time bias in the historical control group which could favor the adjuvant pembrolizumab group, as these patients were diagnosed more recently, and therefore have significantly less follow-up time. The control group could have worse outcomes due to being diagnosed in earlier years and there is likely a referral bias of patients who have relapsed. Even so, compared with the data from other institutions, the OS of our historical controls is significantly longer at 31 months.
Based on the findings from this study we updated our institutional algorithm for patients with stage IVB ATC with BRAF wild-type disease (Fig. 4). Once a stage IVB patient is identified, a biopsy specimen should be rapidly analyzed to determine the BRAF status by immunohistochemistry or single gene BRAFV600E mutation testing. If BRAFV600E has been ruled out, we recommend surgery if an R0/R1 surgery can be accomplished, followed by external beam radiation to the neck with concomitant radiosensitizing chemotherapy. Palliative radiation can also be considered when full-dose radiation is not possible. Adjuvant treatment should be started within 4–6 weeks of completing radiation since recurrences have been seen as early as 4 weeks in our historical cohort. Patients should be treated with 1–2 years of adjuvant pembrolizumab. Longer treatments are not advisable because of the risk of developing an immunotherapy-related serious adverse event, which can occur at any point during treatment with checkpoint inhibitor therapy. However, shortening treatment to 1 year could be studied in the future. Another area of future research is the use of adjuvant pembrolizumab in patients with stage IVA ATC, as well as those with BRAFV600E -mutated tumors. Our trial did not include sufficient numbers of the latter. Because neoadjuvant therapy in BRAFV600E -mutated ATC patients has been studied extensively, this is the preferred treatment for those patients. 1,2,18 However, in countries where complicated surgeries are not possible or BRAF/MEK inhibitors are unavailable, adjuvant pembrolizumab could also be considered for stage IVB BRAFV600E -mutated ATC.
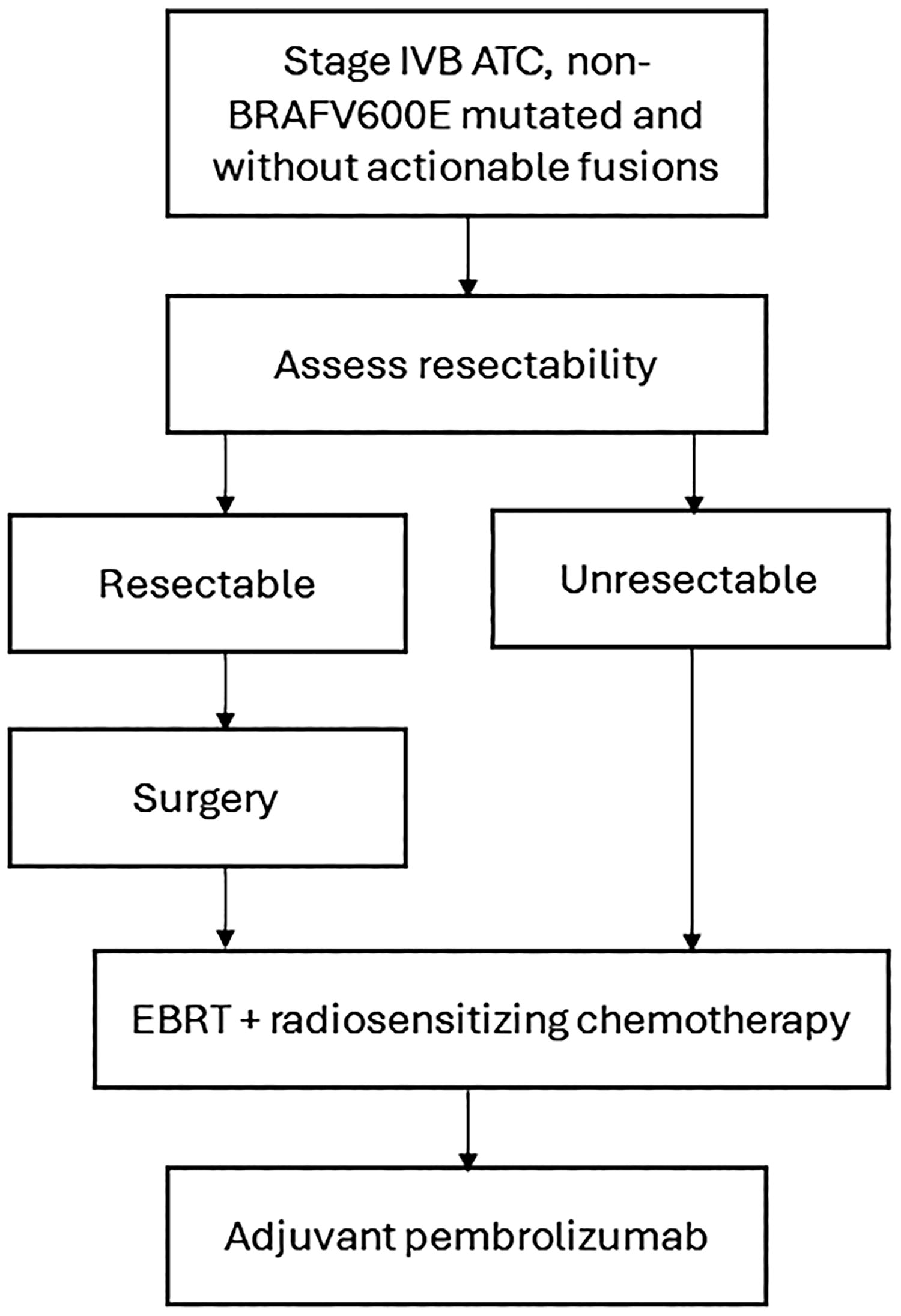
Proposed algorithm for patients with stage IVB anaplastic thyroid cancer without a BRAFV600E mutation. Once BRAFV600E has been ruled out, we recommend surgery when feasible, followed by external beam radiation to the neck with radiosensitizing chemotherapy. Palliative radiation may be considered when full-dose radiation is not possible or acceptable. Patients should be restaged prior to adjuvant pembrolizumab. Ideally, adjuvant pembrolizumab should be started within 4–6 weeks for a period of 1–2 years. ATC = anaplastic thyroid cancer; EBRT = external beam radiation therapy.
We conclude that adjuvant pembrolizumab appears to be a safe and effective strategy to prevent recurrences and prolong survival in stage IVB patients following upfront multimodal therapy. Further studies are needed to confirm these results.
Footnotes
Acknowledgments
The authors wish to thank Merck for providing drug support and the Petrick philanthropic funds for providing the funding for the trial. The authors also thank the brave patients and their families for their participation in the clinical trial and for entrusting their care to them.
Authors’ Contributions
M.E.C.: Conceptualization (lead), data curation (lead), funding acquisition, writing—original draft (lead). N.L.B.: Conceptualization (supporting), writing—review and editing (equal). G.B.G.: Conceptualization (supporting), writing—review and editing (equal). R.F.: Conceptualization (supporting), writing—review and editing (equal). M.G.-M.: Conceptualization (supporting), writing—review and editing (equal). M.Z.: Conceptualization (supporting), writing—review and editing (equal). R.D.: Conceptualization (supporting), writing—review and editing (equal). A.M.: Writing—review and editing (equal). M.D.W.: Writing—review and editing (equal). S.L.: Methodology (supporting) and Conceptualization (supporting), formal analysis (lead), writing—review and editing (equal). B.F.: Formal analysis (supporting). M.S.: Writing—review and editing (equal). S.H.: Writing—review and editing (equal). N.A.: Writing—review and editing (equal). A.L.: Writing—review and editing (equal). J.R.W.: Writing—review and editing (equal). L.de.S.: Writing—review and editing (equal). V.R.M.: Formal analysis (supporting).
Author Disclosure Statement
M.E.C. has received consulting fees from Bayer, Exelixis, Lilly, Merck and Novartis and research funding from Merck, Genentech, Eisai, and Exelixis. N.L.B. reports research funding from Eisai and personal consulting fees from Eisai and Eli Lilly. R.F. reports personal fees from Regeneron, Eisai Inc, Remix Therapeutics, Coherus BioSciences, Rgenta Therapeutics, BioAtla, Bicara Therapeutics, RAPT Therapeutics, and LEK consultant; non-financial support (to institution) from ISA Therapeutics, Merck Serono, Viracta, Gilead, Remix Therapeutics, Rgenta Therapeutics, and Mersana Therapeutics outside the submitted work. A.M. reports research funding from JAZZ Pharmaceuticals and Thryv Therapeutics Inc. M.D.W. has research funding from Bayer. N.A. has sponsored research with Aveo Pharmaceuticals, Innocare Pharma, Bicara Therapeutics, and Pfizer/Genmab and has received consulting fees from Genmab/Pfizer. M.Z. has received research funding from
Funding Information
M.E.C.: Merck provided drug support and the Petrick philanthropic funds provided financial support. N.L.B., G.B.G., R.F., M.G.-M., M.Z., R.D., A.M., M.D.W., S.L., B.F., M.S., S.H., N.A., A.L., J.R.W., L.de.S., and V.R.M.: No financial support provided for this study.
Supplementary Material
Supplementary Data
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.