
Abstract
Radiofrequency catheter ablation (RFA) is an effective treatment of arrhythmias. However, patients often remain symptomatic after the procedure. We aimed to assess the arrhythmia recurrence after successful RFA in relation to patients' symptoms using transtelephonic loop recorders. Thirty-six consecutive patients (age 50±14 years, 17 males/19 females) were enrolled after successful RFA for atrioventricular (AV) nodal reentrant tachycardia (n = 21), AV reentrant tachycardia (n = 8), atrial tachycardia (n = 2), atrial fibrillation/flutter (n = 4), and ventricular tachycardia (n = 1). During 23±6 days of follow-up, 679 events were recorded, 246 of which were true arrhythmic events, mostly (56%) asymptomatic. The vast majority of these true arrhythmic events were due to trivial arrhythmias (extrasystoles or sinus tachycardia), equally distributed among symptomatic and asymptomatic episodes. Arrhythmia relapse was shown in four patients, who had a total of nine episodes, eight of which were symptomatic. No high degree AV block was detected. Overall, symptom recurrence had low sensitivity (44%) and high specificity (95%) for the detection of any arrhythmia, and high sensitivity (89%) but low specificity (58%) for the detection of relapse. In conclusion, transtelephonic monitoring was a useful tool for the assessment of symptoms after RFA and its use may be reserved for the most symptomatic patients to detect a relapse or to reassure them for the benign nature of their symptoms.
Introduction
Radiofrequency catheter ablation (RFA) has replaced antiarrhythmic drug therapy for the treatment of many types of cardiac arrhythmia. 1 Since the early 1990s, RFA has been increasingly used in the management of paroxysmal supraventricular tachycardia and accessory atrioventricular (AV) pathway-mediated tachyarrhythmias because of its observed efficacy and overall safety when performed at experienced centers. Compared with antiarrhythmic therapy, catheter ablation improves the quality of life and is more cost-effective in the long term. 2,3 The success rate for curing supraventricular tachycardias with RFA is high, typically 90%–95%, and the recurrence rate has been based mainly on patients' symptoms and routine electrocardiograms (ECGs) or 24-h Holter recordings. It is believed that lesions created by RFA energy are irreversible, inhomogeneous, and therefore, potentially proarrhythmic. Despite high success rates, patients frequently remain symptomatic complaining of palpitations, dizziness, or discomfort. Conversely, asymptomatic recurrences of arrhythmias may remain undetected.
Transtelephonic electrocardiographic monitors transmit recordings by telephone via the conversion of ECG data to an audio signal. 4 Audio signals are received at a central station, which reconstructs the electrical signal into a conventional electrocardiographic recording. Transtelephonic continuous-loop event recorders are highly effective for establishing a diagnosis in patients with palpitations but are less effective for establishing a diagnosis in patients with syncope, mainly because of the high probability of palpitation occurrence during the limited period of continuous-loop recording (usually 2 weeks), in contrast to the lower probability of syncope occurrence within the same period. 5 These recorders are also helpful for assessment of the safety and efficacy of antiarrhythmic medications and the recurrence of symptomatic supraventricular arrhythmias. 6
The aim of our study was to use transtelephonic electrocardiographic monitoring to assess the recurrence of arrhythmias after successful RFA and explore whether symptoms were related to true arrhythmias or relapse. Moreover, we sought to assess the efficacy of transtelephonic electrocardiographic monitoring and the problems with its use in clinical practice.
Methods
Study protocol
During a 9-month period, consecutive eligible patients who underwent successful RFA were informed about the aim of the study, and after obtaining written informed consent they were enrolled in the study protocol. The study was approved by the ethical committee of our institution. Exclusion criteria were age <18 years and inability to use the device and follow the transtelephonic transmission procedure. A detailed clinical examination, full blood biochemistry including thyroid function tests, ECG, chest X-ray, Holter monitoring, and transthoracic echocardiography were routinely performed before the procedure. Amiodarone was discontinued for at least 1 month and all other antiarrhythmic agents were discontinued for five half-lives before ablation.
Ablation procedure
For the cases of AV nodal reentry tachycardias we used standard procedures, as described in literature. 7,8 Slow pathway ablation using anatomic criteria was used for AV nodal reentrant tachycardia (AVNRT) where the site of the shortest ventriculo-atrial interval during AV reentrant tachycardia (AVRT) was primarily used for concealed pathways. In cases of overt Wolf-Parkinson-White, RFA was delivered at the site of the shortest AV interval during sinus rhythm, or shortest ventriculo-atrial interval during tachycardia. In atrial fibrillation/atrial flutter cases, the cava tricuspid isthmus was targeted using the standard protocol. Interruption was validated with differential pacing. For atrial tachycardia and ventricular tachycardia cases, the site of earliest activation during tachycardia was targeted. Success was validated as noninducibility of tachycardia.
Transtelephonic ECG recorders
After ablation, all patients were supplied with a transtelephonic ECG recorder (Card Guard™ 6650) and were instructed on how to use it. The Card Guard 6550 is a personal three-channel ECG recorder and Holter featuring dual-mode operations of event recording (with autotriggering function of four events) and full disclosure Holter (removable flash memory minidisk). The device continuously records patient's ECG in a temporary memory buffer by overwriting ECGs (loop memory). When arrhythmia is detected, it records an ECG stripe of standard duration that consists of a pre-event period of 1 min duration and a postevent period of 2 min duration, which is stored in the permanent recording memory. Four algorithms were defined: tachycardia (heart rate >150 bpm), bradycardia (heart rate <50 bpm), atrial fibrillation, and asystole (pause >2 s). In addition to the autotrigger recording facility, patients were advised to use the manual recording mode in case of symptoms. The permanent recording memory can record up to five events (four autotriggered and one manual). The pacing algorithm was off, and the blank period between events was 15 min. Recording started at 6–8 h after RFA procedure. The transtelephonic ECG recorder was continuously attached to the patient with a cord using adhesive ECG patches, and batteries were used as energy source, which should be replaced every second day. Every 2 days, patients transmitted stored data to the contact center via a telephone call, where a cardiologist was available for ECG interpretation, symptom assessment, and counseling (Fig. 1A, B). ECG monitoring continued for up to 20 days or more if there are <10 valid recordings. Relapse was defined as recurrence of the preablation clinical arrhythmia.
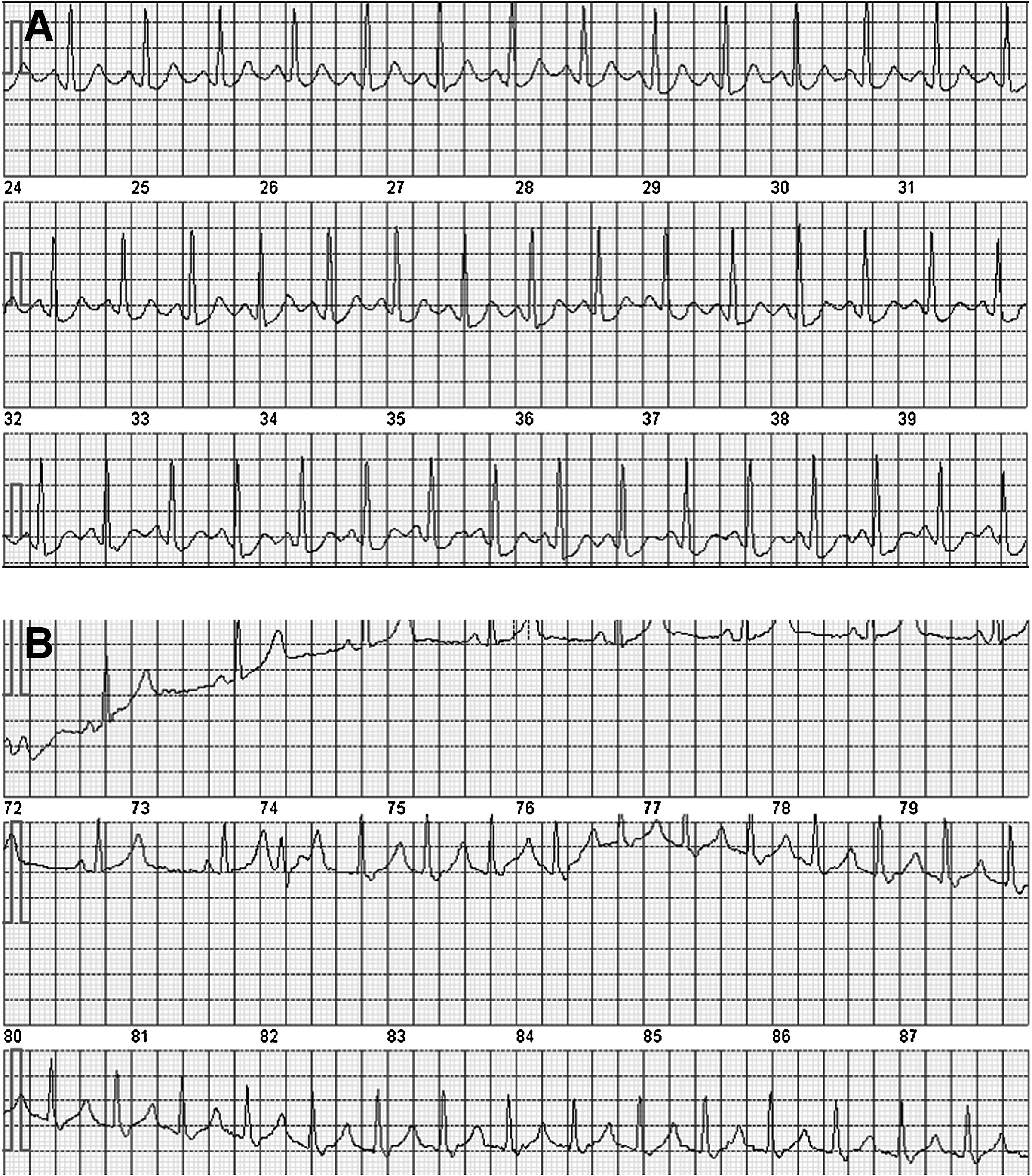
Examples of transmitted electrocardiogram recordings. (
Statistical analysis
Statistical analysis was performed using SPSS v13.0 for windows. Continuous variables were presented as mean ± standard deviation and categorical variables as absolute number (percentage). Differences among consecutive measurements for continuous variables (mean heart rates) were determined with analysis of variance general linear model for repeated measures. Differences between categorical variables were determined by chi-square test. Positive predictive value of algorithms of the transtelephonic ECG recorder to distinguish the types of arrhythmia was calculated as the number of true positive divided by the number of true positive plus number of false-positive results. A p-value of <0.05 was considered statistically significant.
Results
Thirty-six consecutive patients (mean age: 50±14 years, 17 men and 19 women) were enrolled in the study protocol. Most common arrhythmias before RFA were AVNRT (n = 21, 58%) and AVRT (n = 8, 22%). Mean duration of symptoms before ablation was 36±32 months. Patient characteristics are shown in Table 1.
Characteristics of the Study Population
AVNRT, atrioventricular nodal reentrant tachycardia; AVRT, atrioventricular reentrant tachycardia; RFA, radiofrequency catheter ablation.
Note: Values are presented as mean ± standard deviation, or absolute numbers (percentages).
Mean follow-up period was 23±6 days. Among 679 events recorded, 635 (93.5%) were autotriggered and 44 were manual (6.5%). Among the autotriggered events, 65 (10%) were recognized by the algorithms as tachycardia, 110 (17%) as bradycardia, 303 (48%) as atrial fibrillation, and 87 (14%) as asystole. Of the autotriggered events, 70 (9.6%) were unable to be recognized by the algorithms (unified events). Analysis of transtelephonic data revealed an increase in mean heart rate on day 2 postablation (Fig. 2). Holter analysis showed only 246 (36%) true arrhythmic events (mostly trivial) out of 679 recorded ones (Table 2). Arrhythmic events in the overall patient population were due to bradycardia (26%), sinus tachycardia (26%), atrial premature complexes (23%), ventricular premature complexes (15%), atrial fibrillation (7%), narrow QRS tachycardia (2%), and wide QRS tachycardia (1%). Among these true arrhythmic events, only 108 (44%) were symptomatic. Twenty-two patients (61%) had at least one symptomatic event. Symptoms experienced were mainly palpitations (80%), dizziness (5%), presyncope (5%), precordial pain (5%), and chest discomfort (5%). The presence of symptoms had low sensitivity (43.9%) but high specificity (94.7%) to detect a true arrhythmic event. The most frequent events in symptomatic patients were sinus tachycardia and atrial and ventricular premature complexes, whereas most of the true events recorded in asymptomatic patients were due to bradycardia (Fig. 3). Only eight (6%) of symptomatic events and one (0.2%) of asymptomatic ones revealed arrhythmia relapse. The sensitivity of symptom recurrence for the detection of arrhythmia relapse was high (89%), but the specificity was low (58%).
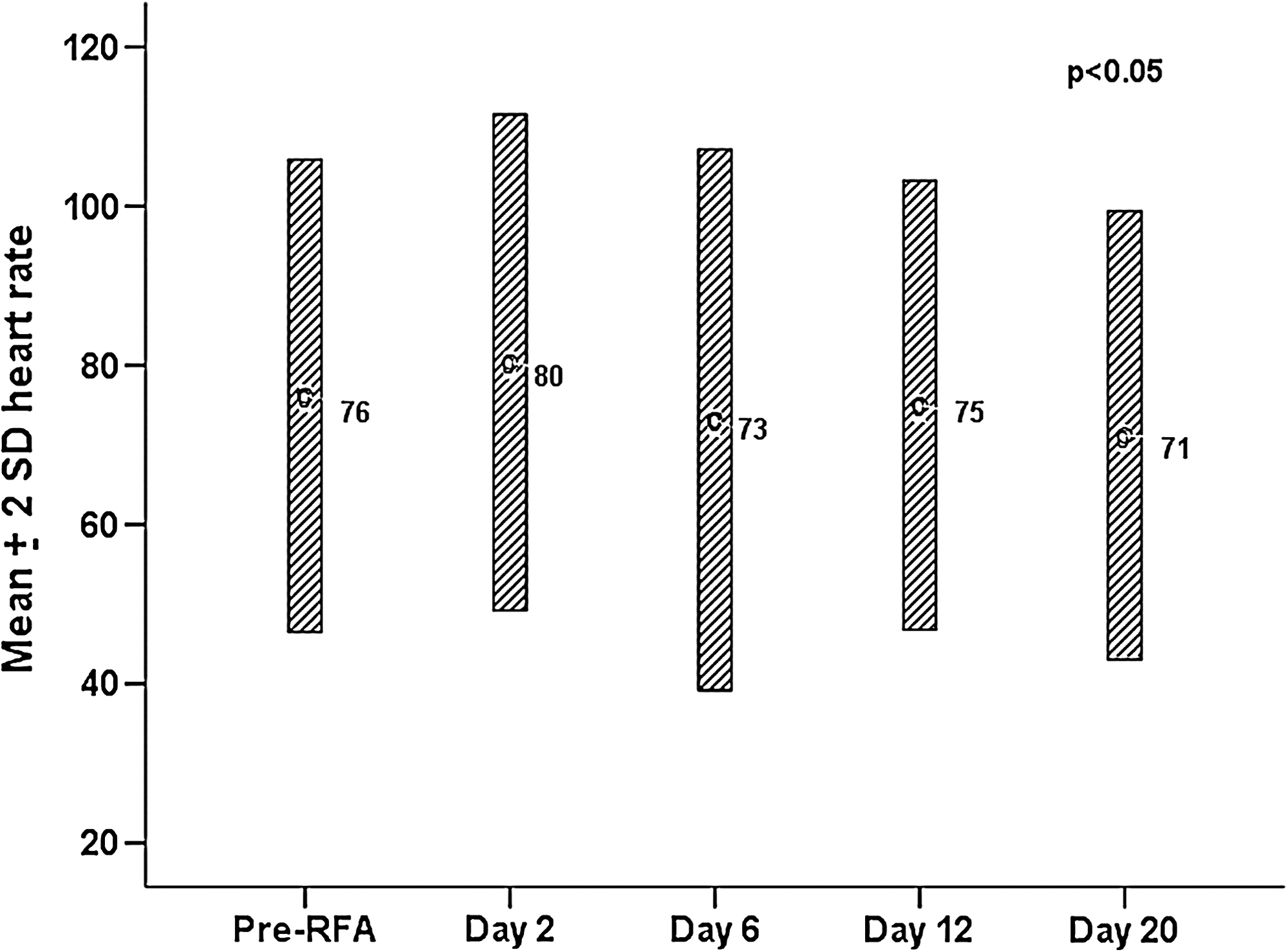
Mean heart rate±2 standard deviation (SD) before radio frequency catheter ablation (RFA) and on days 2, 6, 12, and 20.

Distribution of true arrhythmic events among symptomatic and asymptomatic patients. Percentages represent the prevalence of different arrhythmic events in the overall patient population. Afib, atrial fibrillation; APCs, atrial premature complexes; BRADY, bradycardia; NQRST, narrow QRS tachycardia; ST, sinus tachycardia; VPCs, ventricular premature complexes; WQRST, wide QRS tachycardia.
False and True Arrhythmic Events Among Symptomatic and Asymptomatic Events Recorded
Note: Results are presented as absolute numbers (percentages). Type of recording (autotriggered or manual) is also presented within each category.
The ability of the algorithms of the transtelephonic ECG recorder to distinguish the type of arrhythmia is shown in Figure 4. The tachycardia and bradycardia algorithms had a 71% and 85%, respectively, positive predictive value for obtaining the right diagnosis, whereas the corresponding percentages for atrial fibrillation and asystole algorithms were 7% and 0%.
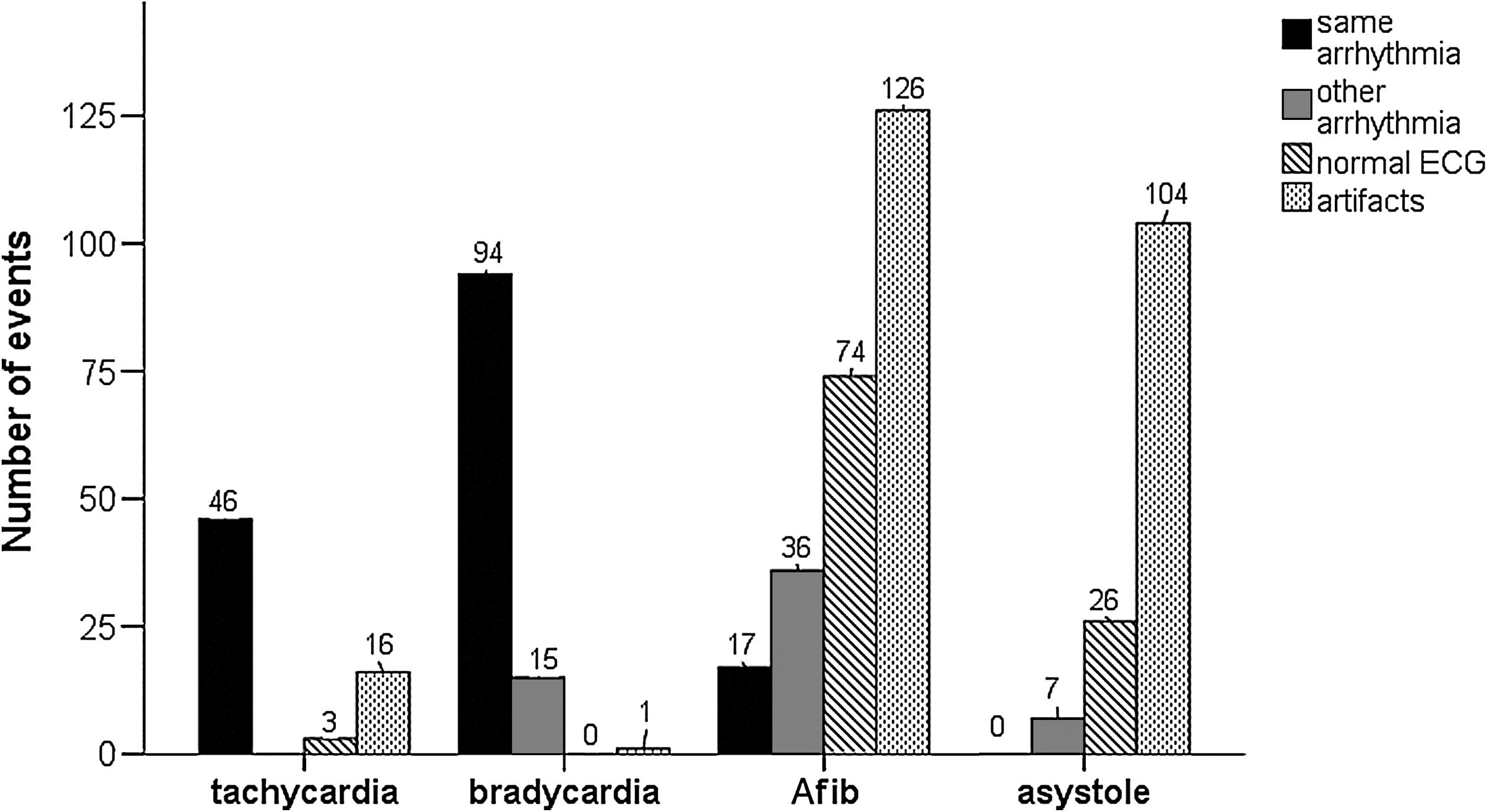
The ability of the algorithms of the transtelephonic electrocardiogram recorder to distinguish the type of arrhythmia. Afib, atrial fibrillation.
Concerning the paroxysmal supraventricular tachycardia recurrence, four (11%) patients had a relapse with a total of nine recorded episodes. Arrhythmia types were modified AVNRT in one patient, AVRT in one patient, and atrial flutter in two patients. All four patients were symptomatic, and only one out of the nine episodes was asymptomatic. The majority of the recorded episodes (75%) occurred within the first 9 days postablation. Finally, the main reported problems of the use of the devices were battery usage (20%), irritation from the patch (26.6%), and social problems associated with the continuous attachment to the device (20%).
Discussion
In this exploratory study we found that the majority of patients remain symptomatic after successful RFA. Nonetheless, the main reason for the postprocedural complaints of patients was the presence of sinus tachycardia and supraventricular or ventricular extrasystoles.
Increased heart rate on day 2 postablation may possibly be related to parasympathetic denervation, which has been reported after ablation of tachycardias. 9 The latter is frequently responsible for persistent inappropriate sinus tachycardia after RFA and it resolves within months following ablation. Nevertheless, we have assessed heart rate after prompted manual recording during programmed calls, and thus it does not represent a 24-h mean heart rate and it possibly depicts an instantaneous sympathetic activation due to anxiety during the first call.
The majority of our patients remained symptomatic complaining mainly of palpitations. It is known that recurrent symptoms may occur after RFA of the fast pathway in AVNRT, because of sinus tachycardia, other coexistent arrhythmias, or failure. 10,11 A previous study showed that palpitations, including palpitations reminiscent of preablation symptoms, are common following RFA and often do not predict pathway recurrence. 12 Transtelephonic transmission of event recordings in our study revealed that even though 78% of the symptomatic events were proved to represent a true arrhythmia, the type of the arrhythmia was mostly benign or trivial (atrial or ventricular extrasystole and sinus tachycardia). Nonetheless, repeat electrophysiological testing is frequently required to document long-term success of radiofrequency ablation for supraventricular tachycardia in patients with recurrence of major symptoms.
Interestingly, more than one half (57%) of the true arrhythmic events recorded were asymptomatic. The observed high incidence of asymptomatic arrhythmic episodes is in concordance with a prospective study of patients with paroxysmal atrial fibrillation or supraventricular tachycardia who were monitored for 30 days with periodic Holter monitoring and a transtelephonic device. 13 The authors showed that in the group of patients with paroxysmal atrial fibrillation, asymptomatic events occurred more frequently than symptomatic, whereas paroxysmal supraventricular tachycardia was more often symptomatic. Our study showed that asymptomatic events were almost always (99.8%) due to benign or trivial arrhythmias. A previous study by Bhandari et al. 14 showed a high degree of correlation between symptoms and ECG-documented attacks of paroxysmal supraventricular tachycardia or paroxysmal atrial fibrillation. The sensitivity of a symptomatic call was 91% for paroxysmal supraventricular tachycardia and 89% for paroxysmal atrial fibrillation. Conversely, lack of symptoms was associated with absence of paroxysmal supraventricular tachycardia or paroxysmal atrial fibrillation in ∼90% of the asymptomatic calls. Similarly, our results showed that symptom recurrence had 89% sensitivity for arrhythmia relapse, whereas absence of symptoms was associated with absence of relapse in 99.8% of the recorded events.
Event recording has been proved useful in distinguishing recurrence of AVNRT, sinus tachycardia, other types of supraventricular tachycardia, and atrial or ventricular premature beats, which all may be a reason for complaints during the first weeks after ablation. 15 As recurrence of tachycardia is unpredictable from a clinical point of view, event recording by the patient with transtelephonic transmission can be a useful tool for follow-up of patients with paroxysmal arrhythmias. 16 It provides a feeling of safety for symptomatic patients who often suffer from anxiety concerning the ablation procedure. Moreover, patients in a South European country are usually overconcerned about a new or a recurrent symptom and have an excess need for reassurance regarding the benign nature of their symptoms, when compared with North European populations. Hospital admission for a control study after several weeks and additional exposure to radiation can also be avoided. Therefore, in case one has doubts whether a procedure was successful or if a patient remains symptomatic, event recording is a superior way of differentiating recurrence of an arrhythmia from premature beats or sinus tachycardia, the two conditions frequently occurring before and after radiofrequency ablation, and in which the symptoms may resemble those of AVNRT in some patients. 17
In the present study, transtelephonic monitoring was proved to be a safe tool with good positive prognostic value for the detection of tachycardia and bradycardia episodes. Atrial fibrillation algorithm proved to have a very low positive predictive value. A possible explanation, apart from the different algorithm used, is that in our population the incidence of atrial fibrillation postablation was very low, a fact that increases the probability of false-positive results. A rising question with the use of transtelephonic monitoring is the duration of its use post-RFA. Zimetbaum and Josephson 5 evaluated prospectively 105 patients with transtelephonic monitors to track palpitations and found that most patients (83%) had an initial diagnostic transmission during the first 2 weeks of monitoring; diagnostic yield and cost-effectiveness were very low beyond this time period.
Another key finding in our study was that no patient experienced a high degree AV block episode after the procedure. The risk of permanent AV block in patients who undergo fast or slow pathway ablation is low and limited to the procedure or to the days immediately after the procedure, and there is no risk of second- or third-degree AV block during long-term follow-up. 18
One limitation of our study is the small number of enrolled patients because of technical limitations such as number of devices and personnel for transtelephonic follow-up communication. However, the recorded events were numerous and they partially balance the limited patient population.
In conclusion, transtelephonic electrocardiographic monitoring was an efficacious diagnostic modality for the evaluation of arrhythmic episodes in the immediate period postablation. Symptoms were seldom related to relapse, and asymptomatic patients had only trivial arrhythmias. Thus, transtelephonic loop recorders may be reserved for the very symptomatic patients post-RFA to detect a relapse or mainly to reassure the more concerned ones for the benign nature of their symptoms.
Footnotes
Acknowledgments
The authors thank Card Guard and Beny Zeevi for their help in providing the loop recorders and the technical modules used for this study.
Disclosure Statement
No competing financial interests exist.