
Abstract
Introduction
Telehealth utilizes information technologies and communication networks for delivering healthcare and education from one location to another, to lower costs, improve access, quality, and efficiency of healthcare services, and distribute limited healthcare resources and expertise. In a California study, it was noted that fewer than 60% of emergency departments reported cardiac surgery, otolaryngology, neurosurgery, plastic surgery, or vascular surgery on call. 1 In another report, Esposito et al. noted that the undersupply and maldistribution of neurosurgeons coupled with the apparent abandonment of trauma care by a significant number of rank-and-file neurosurgeons, and perhaps an over demand for their services, has created a crisis in access to neurotrauma care across the country. 2
Further, New Mexico is faced with having only about one-third of the number of neurosurgeons than other states of similar population size. 3 Increasing the use of telehealth could potentially decrease some of these difficulties including those that may arise in medical emergency-type situations such as intracranial hemorrhages. Many times, medical emergencies take place at or near a patient's home and this is usually followed by a trip to the local hospital. If the hospital is located in a town that is considered a medical shortage area, it is often limited or unable to provide the care necessary. Under those circumstances, in most cases, the patient may take a journey to a large central hospital for assessment, admission, treatment, and eventual discharge. This type of scenario means a long trip, which can delay treatment and influence outcomes. It also increases the distance from family members who may not be able to travel with their loved ones and weakens the link with their primary care physician. 4 In many parts of the United States, such as New Mexico, there is only one Level 1 trauma hospital with one neurosurgery center serving a very large geographic area. It is often the responsibility of the referral hospitals to provide the neurosurgeon with complete and reliable information regarding the patient's status. The neurosurgeon then may have to make a decision on whether or not to transfer the patient without all information that would be desirable.
This project analyzed the University of New Mexico Hospital (UNMH) neurosurgeons' responses to questions designed to determine if transport or management decisions were altered when using a telehealth Web-based program in response to a consultation request from a rural facility. Based on the experience of the UNMH neurosurgeons, we hypothesized that by using a telehealth Web-based system, 25% of neurosurgery transports would be avoided and that management recommendations would also be altered in 25% of the cases independent of the transport decision.
Methods
To enhance the quality of neurosurgery consultations, triage, and transport decisions between a Level I trauma service neurosurgery program at UNMH and referring hospitals, a secure Health Insurance Portability and Accountability Act (HIPAA)–compliant Web-based system was developed. This system enabled the transmission of digital brain and spine images for review by a neurosurgeon at the time of a referring physician's request for consultation or patient transfer. The Web site was developed in conjunction with the Department Chairman of Neurosurgery, the UNM Center for Telehealth and Cybermedicine Research, UNMH Information Technology Department, and a private company, New Mexico Software (Albuquerque, NM). This effort was initiated to provide improved support to referring hospitals and their healthcare providers in making better triage and management support decisions at the time of referral or consultation with UNM. An optimal consultation, aided by the patients imaging studies as well as the clinical history, will make it possible to identify those patients who will benefit from care at our tertiary medical center and the state's only Level 1 trauma service. The telemedicine application is designed to allow referring hospitals to transmit the diagnostic digital images (computerized tomography [CT], magnetic resonance imaging, Ultrasounds, X-ray, etc.) into this Web site called IMED-CON, providing the UNMH consulting doctors with the critical patient information on which to base their decisions at the time of a referral. Images were transferred using the imaging method of the referring hospital via the IMED-CON system, with subsequent access by the consulting service and their particular program. In the cases where the patients are transported to UNMH, this process acts proactively to aid the attending physicians in applying the appropriate care protocols, reduce the initial assessment time and prepare for immediate action as the patient arrives.
As noted, this telemedicine system is a secure Web-based computer imaging program called IMED-CON to which brain and spine images can be sent 24 hours a day at the time of a UNMH Physician Access Line Service consultation or transfer requests to which the neurosurgeons would respond upon being paged by that service. These medical images are produced at the referring hospital and sent to the secure HIPAA-compliant telemedicine Web-based system, allowing the neurosurgeons at UNMH to view the images during the consultation. This system has simple requirements, including Digital Imaging and Communications in Medicine (DICOM) files and images provided from the referring hospital medical imaging or Picture Archiving and Communications Systems (PACS) system, a PC running Windows operating system (2000 and above), and an Internet Explorer browser. All DICOM images are sent uncompressed with the system receiving the raw file. The transmission mechanism uses a Virtual Private Network (VPN) strategy to encrypt and secure the DICOM file and images from your location into telemedicine Web-based system. The system allows flexible Internet connections and will adapt as needed (dialup, wireless, broadband, T1, or higher connections). Typically, the consultant hospital workstations were connected via a T1 level or higher network. When the neurosurgeons accessed the Web site from their homes, a digital subscriber line (DSL) connection was used. The neurosurgeons reviewed images for consultative purposes and triage decision making but not for formal diagnostic readings using the browser and multiple types of workstations. Our study was conducted at the UNMH Neurosurgery Department with support from UNMH in absorbing all costs for utilization of this system. Software installation and training costs were waived. UNMH paid $20.00 transfer fee for every CT series sent to the secure Web site. There was no additional compensation for the consulting neurosurgeons and the system was integrated as part of standard on-call operations and the standard call schedule to assist in triage and transfer decision making. This allows rural hospitals to be able to participate without having to fund it themselves, thus allowing more hospitals to use the system. The medical images received by consulting hospitals are coupled with three questions on the Web site, which were used to gather the data necessary to determine if review of the CT brain and spine images at the time of consultation resulted in any changes in patient management decisions and avoidance of unnecessary transfers to UNMH neurosurgery department and UNMH, the only Level 1 trauma service in the state.
The project program involved the following aspects: Participating hospitals received training and installation on location. Once a medical event is identified requiring a medical consult from the consulting neurosurgical team, medical images produced from the referring hospital are sent to the telemedicine Web-based system, which is password protected. A case file is created, upon which the consulting medical team is able to securely view the CT scan from any Web browser while consulting with the referring physician (
Fig. 1
). The consulting physician can then make a decision utilizing the Web-based CT image and conference call to decide whether or not to accept the patient and/or make changes in their current medical care either for transfer or for observation and treatment at their local hospital. Before viewing the patient's CT brain and spine scan, the consulting physician is asked to answer one initial question and then two additional questions after reviewing the scans using a “Yes” or “No” radio button on the Web page (
Fig. 2
): “Before reviewing the case with the supporting information, based on your current knowledge would you have accepted this patient for transport?” (Yes or No). The physician then answers two more questions placed on the Web page before ending their telemedicine session: “After reviewing the case with the supporting information, did you accept this patient for transport?” (Yes or No) and “Did your management recommendations change?” (Yes or No). The answers to these questions were then compiled in a database by a system support specialist affiliated with IMED-CON. The binomial distribution was used to calculate 95% confidence limits for the percentage of patients transferred and the percentage with recommended management changes. Fisher's exact test was used to compare recommended management changes between those who were transported and those who were not transported. Power analysis was based upon a significance level of p ≤ 0.05 and a confidence interval of 97%, which are required to see a greater than or equal to 25% change in transport or management recommendations. The sample size needed to test the hypotheses was determined to be a minimum of n = 30. The data gathered were used to determine if there was a decrease in predicted patient transfer rates and if there was a change in the patient management recommendations independent of the transfer decision after using the Web-based telemedicine system.
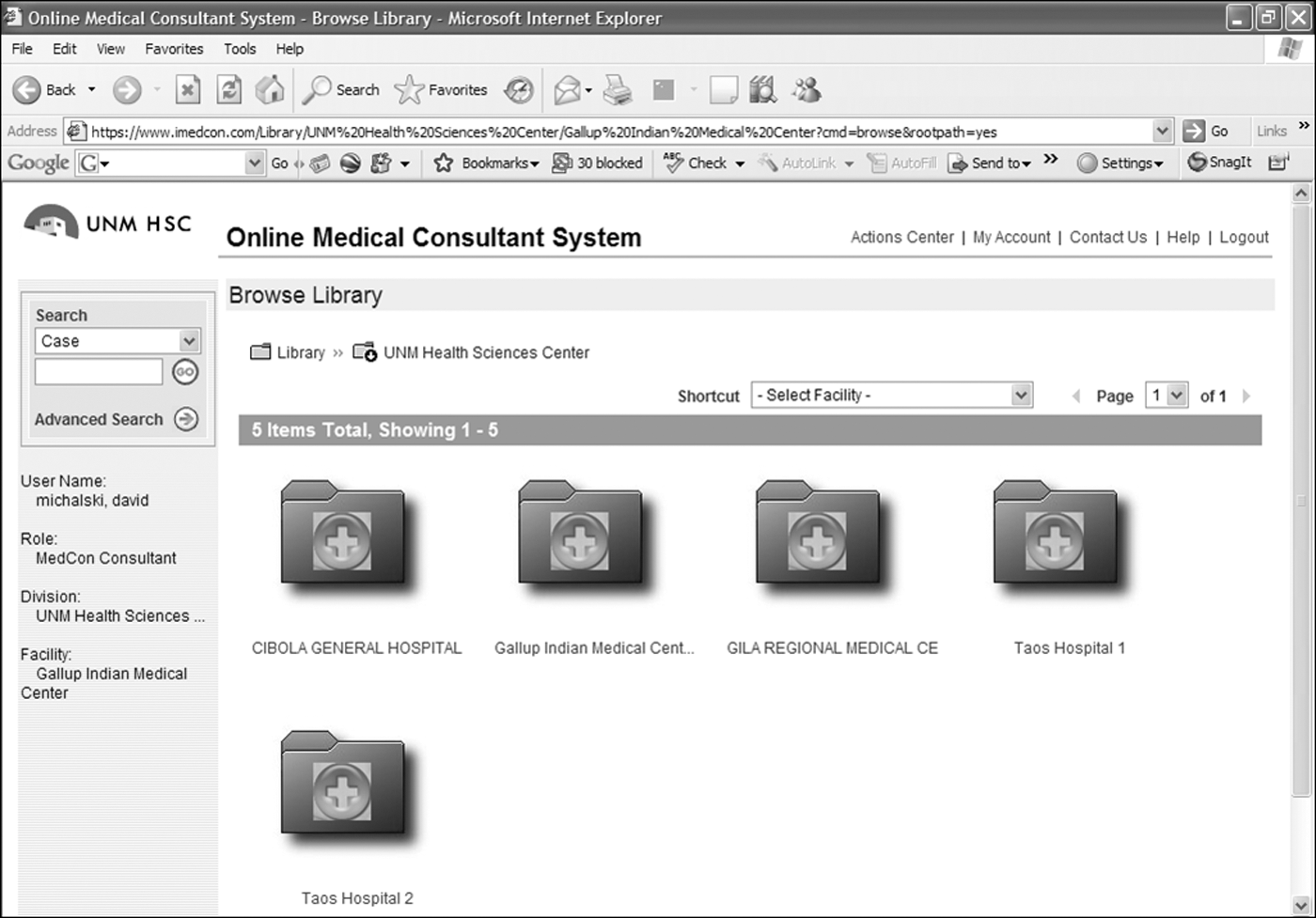
The consulting neurosurgeons' initial view of the online Web site and available cases.

Screen shot of the Web page with access to the three evaluation questions and actual images that could then be enlarged.
Results
During the time frame November 2007 through October 2008, 39 consultations regarding head trauma were received at UNMH from seven participating referring hospitals: Gallup Indian Medical Center, Cibola General Hospital, Gila Regional Medical Center, Taos Holy Cross Hospital, Lovelace Hospital, Rehoboth McKinley Christian Hospital, and St. Vincent Hospital. Based upon the first question asked on the IMED-CON Web site, the consulting neurosurgeons anticipated that 25 of 39 (64%) of the referral requests would have been accepted for transport to UNMH, but after the neurosurgeons reviewed the Web-based images, only 14 of 39 (36%) of those consults resulted in a transfer. Therefore, only 14 of 25 (56%) of those cases initially anticipated for transport actually required a transfer to UNMH, that is, 44% (11/25) of the transports were avoided and the patients were managed at their local facility (95% confidence intervals = 24%, 65%). After reviewing the images, the neurosurgeons recommended management changes in 17 of 39 (44%) of all consultations (95% confidence intervals = 28%, 60%)—14 of 25 (56%) of the cases in which the patients were not transported and 3 of 14 (21%) of the cases when they were transported (see Table 1 for summary of results).
Outcome Data Using Web-Based Telemedicine Neurosurgery Triage System
Ninety-five percent confidence intervals = 24%, 65%.
Ninety-five percent confidence intervals = 28%, 60%.
Using this system, the results exceeded the expected transfer rate avoidance of 25%. Instead, after looking at the images, 44% of cases, in which neurosurgeons would have accepted the transfer, did not result in a transport, leading to a transfer rate that decreased even more significantly. Among those patients who were not accepted, the neurosurgeons felt that the patient could be adequately served at the referring hospital, thus appropriately utilizing resources at the local hospitals and keeping more beds available at the UNMH Level 1 trauma service. The specific changes in recommendations were not collected for this study. After reviewing the images, none of the consultations in which there was not a transport request or in which the neurosurgeons were not originally planning to accept the patient in transfer resulted in a transport.
Discussion
In many parts of the United States, such as New Mexico, there is only one or a limited number of Level 1 trauma hospitals with one neurosurgery center serving a very large geographic area. It is often the responsibility of the referral hospitals to provide the neurosurgeon with complete and reliable information regarding the patient's status. The neurosurgeon then may be forced to make a decision on whether or not to transfer the patient without adequate information. However, with the implementation of a system such as IMED-CON, the consulting neurosurgeon can more accurately assess and triage the patient with both only verbal and visual image information.
Telemedicine has been implemented successfully in multiple hospitals and locations for use in the decision making regarding the transfer of neurosurgical patients. 5 –14 Teleradiology is already used by many medical facilities around the world, these systems are reliable, and the quality of transferred images has been good, allowing prompt and accurate interpretation by the consulting neurosurgeon or neuroradiologist. 14 This has been shown to accomplish an improvement in the outcomes for the patients and decrease costs for the neurosurgical departments located at the Level 1 trauma centers and the transferring hospitals by preventing unnecessary transfers. In addition, in patients who do need to be transferred to the neurosurgical center, teleradiology allows changes in treatment to be done in the referring hospital upon the advice of the neurosurgeon being consulted. There is an additional advantage that allows the accepting neurosurgeon to have more involvement in the care the patient is receiving even prior to arrival and thus potentially improve patient outcomes.
The multiple benefits of current teleradiology systems, which include improving patient outcomes, reducing unnecessary patient transfer, and decreasing the costs that are spent by both the neurosurgery center and the rural hospitals, are important in evaluating the effectiveness of implementing a teleradiology system in other areas, specifically areas that are more rural and distant to a neurosurgery center that pose a challenge and additional expense. Evidence from perspective observational studies that looked at the difference in the clinical parameters and outcomes from before and after a teleradiology system, which was used to assist in transfer decisions, has shown that unnecessary transfer can be reduced by 21% (14/66), and most importantly, the proportion of patients with a favorable outcome is higher in the teleradiology group. 6 Teleradiology was originally implemented in patients with head trauma in the early 1990s, and since then, Lee et al. described a 43% reduction in neurosurgical referrals. 7 This can be attributed to the neurosurgeons ability to view the images while discussing the need to transfer, thus allowing the neurosurgeon to make a much more informed decision. This approach and the results experienced are also similar to those reported by Bailes et al., who used neurosurgical telemedicine network with ability to review teleradiology images. They also reported cost savings primarily through the avoidance of unnecessary tertiary referrals by helicopter transport. 11,12 Although a cost analysis was not done in our study, transport avoidance would have been a major component of cost avoidance and savings. Presumably, the decreased use of a tertiary care center would have also resulted in cost savings. The reduction in the number of patients being transferred frees up more bed space in the neurosurgical ward and allows the rural hospitals to care for the patients closer to their homes. The use of computer imaging and the ability to better determine the need for transfer provides benefit in preventing unnecessary transports, allows more rational use of resources, and reduces cost by reducing the number of transfers. 3,9 In addition, the use of teleradiology for patients who do need to be transferred to the neurosurgical center allows the consulting neurosurgeon to make appropriate changes in management recommendations that can be implemented at the referring hospital prior to transport and improve stabilization. 4 In an additional study performed in the Ospedale Maurizio Bufalini regional neurosurgical center including a total of 541 patients, 467 of the patients involved in image transmission never reached neurosurgery and were entirely managed in peripheral hospitals. 10
With advancing technologies, there is a possibility for images to be transferred to the consultant's laptop, other handheld devices, or mobile phone. The recent advances in telemedicine and availability of real-time audiovisual teleconferencing have been shown to have a favorable impact on emergency neurosurgical referrals in other programs as well. 14
Our study suggests that utilization of this secure HIPAA-compliant Web-based computer imaging program will help decrease unnecessary patient transfers and help with timely management decisions. Additionally, our data show that there is a proportion of patients who would not likely benefit from a hospital transfer, who otherwise might have been transferred to the consulting hospital. The ability of the consultant to view the images at the time of consultation by using the Web-based computer-imaging program allowed for more informed transfer decisions and management recommendations. Although statistically significant, limitations of the study include a small sample size. In addition, the study was completed to evaluate positive outcomes primarily for the tertiary care center in transfer avoidance. Future studies would be needed to evaluate the outcomes at the referring institutions, including confidence in managing the patients locally, morbidity, and mortality as well as overall cost savings. Additional studies can be done to determine the ultimate outcome of those patients who are not transported, types of management recommendation changes, as well as trauma center preparation changes that occurred when using this Web-based system. Future applications of this approach may also be beneficial for case reviews, continuing quality improvement, and training and education in triage, transfer decision making, and stabilization of head trauma patients.
In summary, this Web-based telemedicine system resulted in improved head trauma triage decisions, avoidance of a significant number of transports and associated costs, allowed more patients to remain in their local community facility closer to family support, and avoided the unnecessary use of limited resources and beds at the Level 1 trauma center. For those patients who are transported, the trauma center can also be better prepared for managing those patients upon arrival.
Footnotes
Acknowledgments
The authors thank Dr. Betty Skipper for her assistance with the statistical analysis and Mr. David Michalski for his assistance in the collection of the data and his continued correspondence throughout the duration of the study. The two first authors were medical students who worked equally on this project. The order of their listing was purely alphabetical.
Disclosure Statement
No competing financial interests exist.