
Abstract
Introduction
The significant health inequity between Aboriginal and Torres Strait Islander children and nonindigenous Australian children is well documented. 1 –3 Chronic disease is becoming increasingly prevalent with progressively younger age of onset in the Aboriginal and Torres Strait Islander population. 4 –6
Otitis media is one preventable chronic disease that is highly prevalent among the indigenous community. 3,7 Evidence in the literature has suggested that untreated otitis media can result in abnormal hearing levels with subsequent speech and language difficulties leading to learning difficulties, truancy, and low self-esteem. 8,9 Additionally, the incidence of impaired vision among school-age children is also considered another reason for learning difficulties in the classroom. 10 The health problems associated with chronic illness among children in indigenous communities has prompted consideration of more efficient strategies to deliver specialist health services in a collaborative and culturally acceptable manner.
Asynchronous telehealth (such as the collection and transmission of prerecorded video-otoscopic images) has been reported as a feasible method for the assessment of ear, nose, and throat (ENT) conditions for rural indigenous children. 11 However, the feasibility of integrating telehealth with existing community-based services for the early detection, monitoring, and treatment of chronic disease in Australian indigenous children has not been established.
The objective of this study was to determine the feasibility of integrating a mobile telehealth-enabled ear, hearing, and vision–screening service with existing community-based health services for Aboriginal and Torres Strait Islander children in Australia.
Materials and Methods
Ethics
Ethics approval for the study was provided by the Royal Children's Hospital and Health Service District Ethics Committee in Brisbane and the University of Queensland Medical Research Ethics Committee. The project complies with National Health and Medical Research Council (NHMRC) Guidelines for Ethical Conduct in Aboriginal and Torres Strait Islander health research.
Participants
Participants in the study were Aboriginal and Torres Strait Islander children aged between 0 and 16 years, attending schools and daycare centers in the South Burnett region of Queensland.
Intervention
Community consultation, engagement, and collaboration in all areas of the project were integrated into the development of the service and research project. This included the evaluation and establishment of the identified community health needs and project design requirements.
A mobile health-screening service was developed and taken to selected local community primary schools and daycare centers to conduct health-screening assessments of indigenous children.
The screening service was delivered from a Mercedes Sprinter (Fig. 1), custom fitted with work benches, storage facilities, handwashing sink, and refrigerator (Fig. 2). A wireless capability of 802.11g was installed to provide networking within the screening van. Remote database access was facilitated by a High-Speed Downlink Packet Access wireless broadband connection to a commercial telecommunication carrier.

Health screening van used to routinely assess indigenous children in the South Burnett region of Queensland.
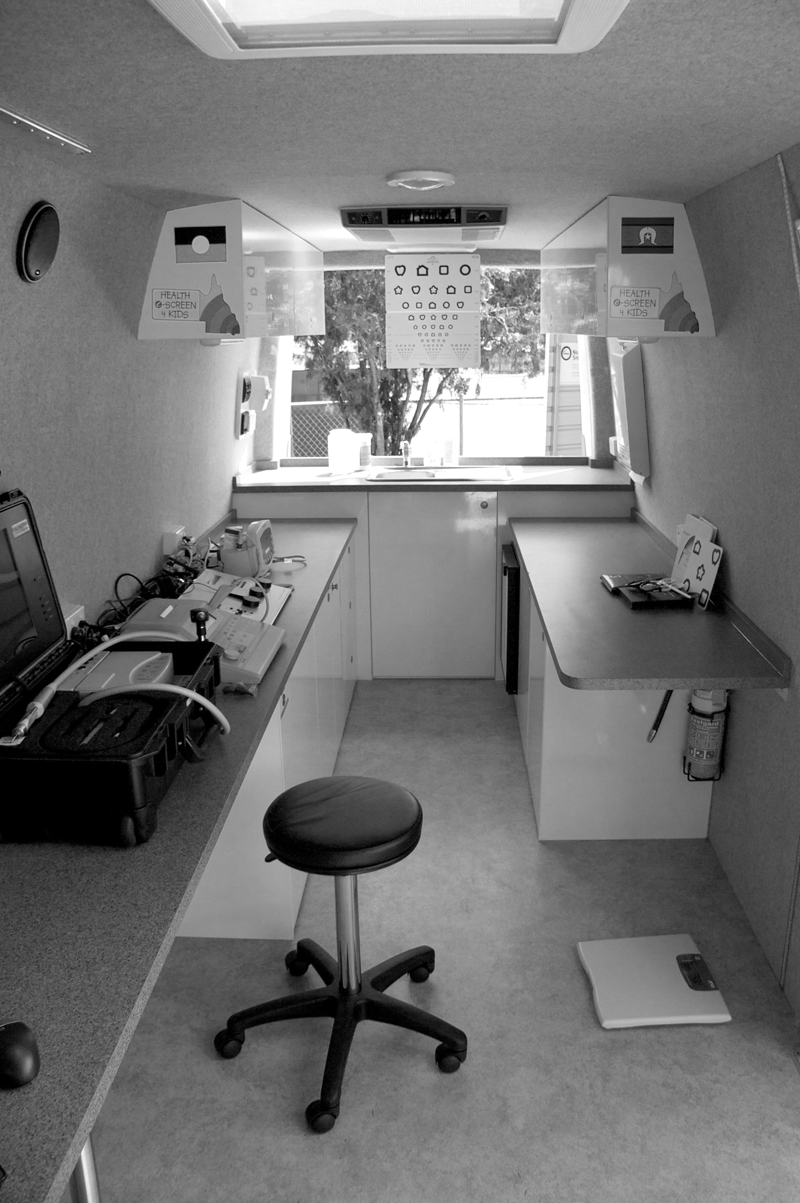
Health screening van (interior view)—fully equipped with diagnostic equipment and telecommunications for the collection and transmission of information.
The van contained ear health-screening equipments including a hand-held otoscope (Welch Allyn Hand Held Otoscope), tympanometer (GSI 38, Auto Tymp), audiometric testing equipment (GSI 68 Diagnostic Audiometers), and video-otoscope (Inline System, Carry Case). The van was also equipped with vision-screening devices including visual acuity at 3 m (PattiPics Chart; Precision Vision), cover test (Ishihara), occluder, Randot Stereo Test (Stereo Optical), glazed flippers + 1.50 (Cyclopean Design), and color vision test made easy (Waggoner).
An aboriginal health worker with advanced hearing-health training and extensive experience in ear health was employed as part of the program through the community health service, to coordinate the local service and to perform the screening assessments (Tables 1 and 2).
Screening Assessments Diagnostic Criteria for Middle Ear Disease
Type A tympanogram suggests normal pressure in the middle ear and normal mobility of the eardrum. Type B indicates little or no eardrum movement, suggesting fluid in the middle ear space. Type C tympanogram refers to a middle ear with negative pressure, suggesting retraction of the eardrum or blockage of the Eustachian tube.
Screening Assessments Diagnostic Criteria for Hearing Impairment Based on the Minimum Audible Sound Pressure Levels
dB, decibel; Hz, Hertz.
Information sheets and consent forms were distributed by the schools to parents/guardians in advance of screening clinics. Children, who presented to the clinic with parent consent, were screened by the aboriginal health worker.
Following screening, the results of assessments were uploaded to a secure database specifically designed for the project via a laptop and wireless broadband Internet connection. For children who failed screening assessments, referrals were made to local health services for further review and management. Children who failed eye-screening assessments were referred via the database to the optometrist (refer to Table 3 for eye test criteria and referral pathways). For those failing ear-screening assessments, tele-otology clinics were completed with an ENT specialist in Brisbane.
Vision-Screening Assessments Test and Criteria
Vision-screening assessment measures as per Australian Optometry Standards. All tests were performed on children above 4 years of age.
The ENT specialist reviewed ENT Online Assessments via a database that included patient information (images of the tympanic membrane; health-screening information shown in Tables 1 and 2; medical chart from the hospital, including hearing test results and audiology reports, if available). This information was used for the ENT decision to provide a diagnosis and treatment plan ( Fig. 3 ).
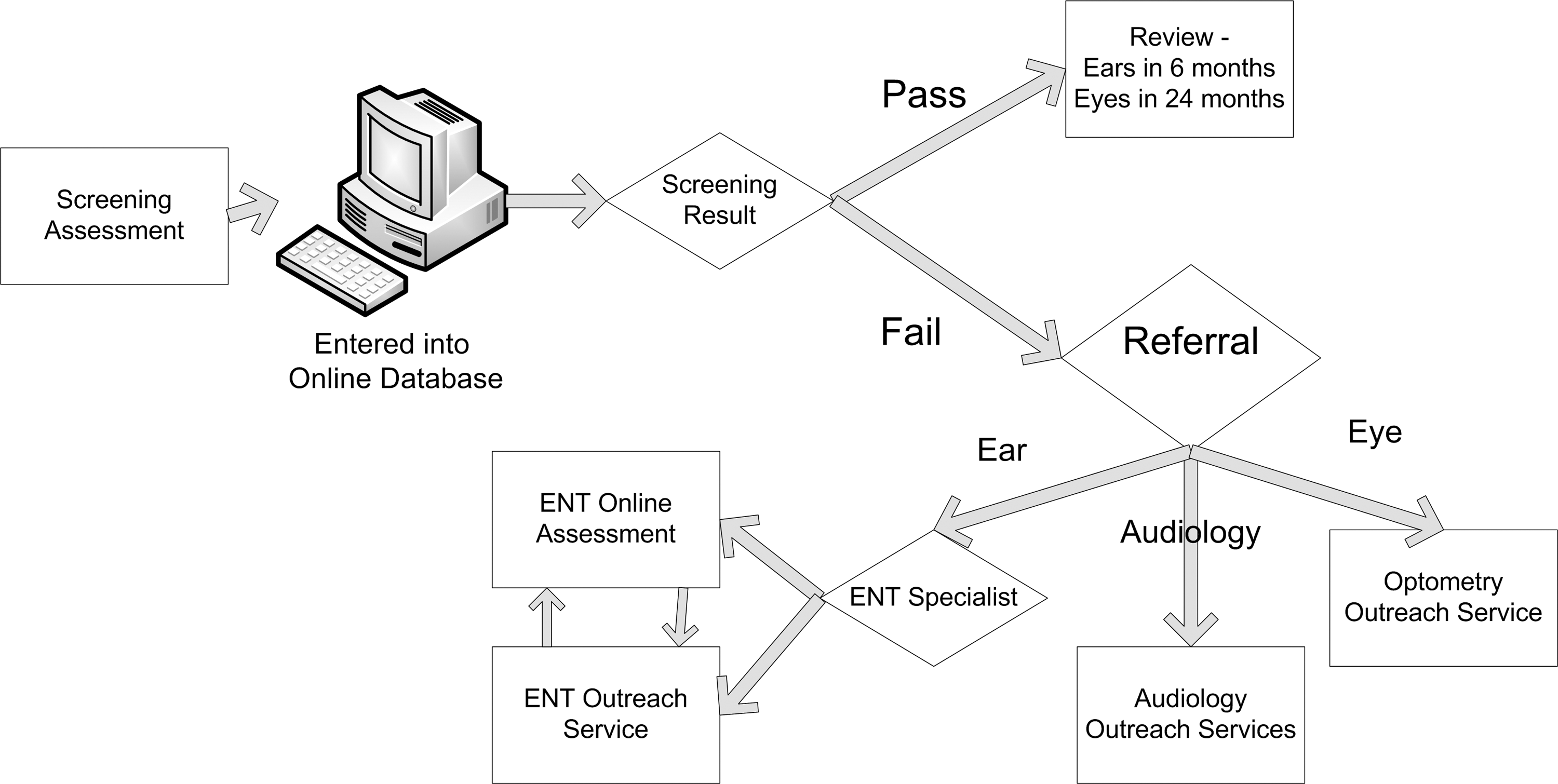
Patient referral pathways—demonstrating actions taken during the health screening process.
Outcomes
Feasibility was evaluated across a number of areas including community acceptance, integration with existing community-based services, and the technical/practical feasibility of presenting diagnostic information for telemedicine (online) consultations. Community acceptance was measured by the consent rate (consent forms returned) and the participation rate (number of children who utilized the screening service/consenting children). Integration with existing community-based services was measured by the number of referrals made and the referral rate (the number of children seen by the service they were referred to). Technical feasibility was measured using a simple three-point categorical scale: excellent, good, and poor, according to the quality of screening images as rated by specialists reviewing the information online.
Sample Size
As this is a feasibility study, no formal sample size calculation was completed. To assess feasibility using the outcomes described above, the entire population of indigenous children, whose parents/guardians gave consent, attending 16 local community primary schools was used.
Results
Consent Rate and Participation Rate
Between February and July 2009, 743 of 980 consent forms distributed were returned (76%). During the first 6 months, 12 of the 16 schools recruited to the project were visited by the screening service. Of the 743 children with parental consent, a total of 442 (59%) were screened.
Screening Result and Number of Referrals
Forty-one percent of children failed one or more components of the ear-screening assessment, 12% had signs of hearing impairment, and 15% failed vision-screening assessment. All patients failing screening assessments were referred to other community health services for management and/or follow-up review in the screening clinic in 3, 6, or 12 months (Table 4).
Summary of Assessments: Results for 743 Children Screened Between February 2 and July 31, 2009
Screening rates are expected to improve, as, in the first 6 months, 12 of the 16 schools enrolled in the study have been visited as part of the screening program.
The age of the children in this group precluded accurate audiometric and visual acuity testing.
Referral categories are not mutually exclusive; all 183 children failing screening assessment were referred to one or more community services.
ENT, ear, nose, and throat.
Referral Rate and Technical/Practical Feasibility
Of the 157 referrals made to the ENT specialist for online review, three separate tele-otology clinics were conducted with an ENT specialist. In the 6-month study period, 59 children's cases were reviewed through an ENT Online Assessment (Table 5). The ENT specialist rated the diagnostic images viewed using the online database as excellent or good in 90% of cases, indicating that 10% of the images were either out of focus or too dark to make a valid decision. For the 46 referrals made to local optometry services, 18 patients (39%) have been reviewed in a single outreach optometry clinic.
Summary of Tele-Otology Clinics Conducted Between February 2 and July 31, 2009
This list is not mutually exclusive (e.g., all seven patients being referred for both audiology assessment and review at the next ENT outreach clinic).
Discussion
Telemedicine has been shown to be useful for the assessment and management of ENT conditions. Pioneering work was reported in the early 1990s by researchers in Alaska, who used videoconference networks for real-time consultations between general practitioners and an otorhinolaryngologist. 12 Subsequently, a number of studies have been also conducted to show relatively high patient satisfaction and comparable diagnostic accuracy between consultations done via videoconference and conventional face-to-face assessments. 13 –15
Asynchronous telemedicine methods have been also reported in this field. As part of the development of a store-and-forward tele-otology system for use in western Australia, Eikelboom et al. assessed the quality of images obtained using four different video-otoscopes. 16 The study identified that commercial video-otoscopes can be used to capture video footage of the ear canal and tympanic membrane. Compression of these video-sequences at a ratio of 1:300 would be suitable for tele-otology. As a result of these early findings, a training package was developed to support the use of tele-otology screening in remote communities. In a study with 30 aboriginal health workers, reasonably good-quality images could be obtained after a short period of training. 17 In a follow-up study with 66 children in remote communities, Eikelboom et al. concluded that good-quality still images of the tympanic membrane, audiological and tympanometric data, and clinical history provide an ear specialist with sufficient information to make a confident diagnosis and provide management advice. 18
In Queensland, Smith et al. evaluated the accuracy of prerecorded video images for the ENT assessment of rural indigenous children using telemedicine. 11 In this study of 58 subjects (mainly indigenous children), the diagnosis reported by an ENT surgeon face-to-face was identical to the blinded diagnosis made by the same ENT surgeon some months later in 81% of cases. Decisions relating to clinical management were identical in 75% of cases. Prerecorded images were shown to be useful for the assessment of common ENT conditions. In Alaska, a similar study also showed that the use of prerecorded patient information was an acceptable method of following up postsurgical patients who normally would have traveled to see the specialist in person. 19
Building on these findings, this study has evaluated the feasibility of integrating a mobile telemedicine-enabled screening service with existing community-based services. This service has been developed specifically for Aboriginal and Torres Strait Islander children at risk of developing chronic diseases, including ear disease. Instead of children and families having to travel to health centers or regional hospitals for health screening, our service provides easy access within their own local community.
The results of this preliminary study suggest that this is a feasible approach. The early consent rate and participation rate achieved is a positive reflection of community acceptance and community uptake of the project. The early consent of 743 of 980 children approached (76%) and the participation rate in the first 6 months accounting for 442 of these 743 children (59%) are promising indications of community acceptance. In 2007 and 2008, the average number of children screened per annum for ear disease was 440. Within the first 6 months, we had reached the same workload (number of children screened) using this alternative method of health screening. We feel that important factors in the success of the service so far include the consultation and collaboration undertaken with the local community in an appropriate and culturally safe manner and the involvement of a local health worker to coordinate the service, to be involved in the research team and to conduct the screening assessments.
The screening service appears to be integrating well with the existing local community services, with the number of referrals to other services and with the number of follow-up specialist clinics being completed. Referrals of children failing screening assessments to existing community-based health services are resulting in the early treatment and/or management of the children who had chronic conditions identified. This includes the review of ENT online assessments for 59 children by a specialist ENT surgeon in three tele-otology clinics. Additionally, vision screening resulted in the local review of 18 children in an optometry outreach clinic, out of 46 children failing eye-screening assessment.
The specialist ratings of the images collected by the health worker indicated that an adequate-quality image can be obtained and presented for sufficient review online.
Limitations
The cost and long-term impact of this community-based screening service have not been evaluated as part of this feasibility study. These aspects will be examined prospectively as part of the research program.
Conclusions
The mobile telehealth screening service developed aims to identify, monitor, and support the treatment of Aboriginal and Torres Strait Islander children who are at high risk of developing chronic disease within their local community by using telehealth. For Aboriginal and Torres Strait Islander children, it is feasible to integrate a mobile telemedicine-enabled screening service with existing community-based services.
Further research will be required to evaluate the long-term impact on Aboriginal and Torres Strait Islander child health and the cost-effectiveness of this approach. The preliminary results described in this article are very encouraging and demonstrate the feasibility of integrating a mobile telemedicine-enabled screening service with existing community-based services. Although our initial experience has focused on hearing and vision assessment, there is the potential for this health-screening service model to be adopted for the screening of other chronic illnesses in other communities, such as diabetes and renal disease.
Footnotes
Acknowledgments
The authors are grateful for the support of the Cherbourg Aboriginal Community and the Darling Downs West Moreton Health Service District (South Burnett Programs). The authors acknowledge the following project collaborators: Queensland Health—Cherbourg Community Health Service and the Deadly Ears Aboriginal and Torres Strait Islander Ear Health Program. In addition, the authors thank Professor Richard Wootton for his advice and support during the preliminary stages of this project. Funding has been provided through the Royal Children's Hospital Foundation by corporate and community sponsors including Virgin Blue, the Telstra Foundation, the Australian Children's Trust, the Zig Zag Foundation, the Rio Tinto Aboriginal Fund, the Ian Potter Foundation, the Sidney Myer Fund, Grosvenor Foundation, and Perpetual Trustees.
Disclosure Statement
No competing financial interest exists.