
Abstract
Introduction
Globally, Canada contributes 2% of all greenhouse gas (GHG) emissions and is one of the highest per capita emitters among developed countries. 1 In 2007, Canadians produced an estimated 747 megatons of carbon dioxide equivalents (CO2eq) in GHG emissions. 1 The second largest emission-producing category was the transportation sector, which accounted for 35% of Canada's GHG growth from 1990 to 2007. 1 There has been a renewed effort by all levels of government to reduce dependence on the personal automobile and increase the viability of public transit and cycling. Telemedicine being “green” has been suggested in the recent years. 2,3 Telemedicine provides the opportunity to increase access to care and help reduce GHG emissions produced by personal vehicle travel use.
Previous studies have demonstrated that videoconferencing reduces the distance traveled and leads to substantial reduction in vehicle emissions. 4 –8 One of the earlier studies by Henderson and Mokhtarian on telecommuting in the workplace empirically determined travel benefits for eight staff members using self-report travel diaries to collect travel data such as vehicle odometer readings from home to a center-based telecommuting location. 8 A U.S. study found significant reductions in travel distances for telecommuting days in comparison to nontelecommuting days, with an emission reduction of 49% in nitrogen oxides (NO x ) and 53% decrease in particulate matter (PM) emissions. 8 Similarly, a U.K. study by Lewis et al. used self-report questionnaires to estimate the amount of emissions saved by videoconferencing for a total of 51 multidisciplinary team meetings instead of driving to the meeting location over the time span of 2 years. 7 The study found a total of 38,800 km in travel reductions, which resulted in avoidance of 4,286 kg of CO2, using videoconferencing to facilitate multidisciplinary team conferences. 7
More recently, two studies have focused on clinical telemedicine involving patient travel data to calculate travel and emission savings from using telemedicine. 5,6 In a U.K. study by Dorrian et al., a standard route planner from the Automobile Association was used to calculate the journey distance to the consultant site for 42 telemedicine patients over a time period of 17 months. 5 Dorrian et al. estimated a carbon emission avoidance of 123 kg of CO2 emissions per person per journey. 5 Similarly, a large-scale study in Australia reviewed retrospective telemedicine activity data for 1,000 telepediatric burn assessments over a 6-year time period. 6 Smith et al. calculated the travel distance between each of the 65 regional centers and the consultant hospital and estimated that over 1.4 million km were saved in patient travel, resulting in a further reduction of CO2 emissions of 234 tons. 4,6 In summary, travel distance calculations differ in the reported studies and either self-report or standard route estimation methods were used. In addition, emissions were calculated according to methodologies set by respective government agencies for the location where those studies have taken place. Despite the variability in methodology between studies, the results consistently found reduced travel distance and associated emission reductions. To this date, there has been no Canadian study on telemedicine and GHG emissions. The present study provides an analysis of the travel and emissions impact of telemedicine consultations in the Canadian setting.
Materials and Methods
The purpose of this study was to calculate the travel distance and GHG emissions avoided for 840 teleconsultations completed in a 6-month time period at an academic health science center consisting of three hospital sites. The distance calculation used Web mapping calculator tools and postal code data for the patient's home, telemedicine site attended, and the consultant hospital site. Our model also considered GHG emissions produced by the energy used to run the telemedicine videoconferencing units. Personal cost factors were also discussed and a calculation to determine the potential cost avoidance for the Northern Health Travel Grant (NHTG) Program was included.
Sample Characteristics
The University Health Network is a multisite academic hospital in Toronto, Ontario. Ontario is Canada's second largest province covering more than 1 million km2—an area larger than France and Spain combined. 9 Our three hospitals provide quaternary care to patients with complex illnesses. The University Health Network provides a range of specialized healthcare services accessed by a wide patient population base across the province of Ontario. Over 25 healthcare specialties were accessed by this sample, with 30% of teleconsultations consisting of surgical critical care assessments.
Methodology
Outpatient teleconsultations completed in the province of Ontario within a 6-month period (October 2008 to March 2009) were selected for this investigation. The final data file contained 840 records, consisting of 615 unique postal codes and 88 telemedicine site locations across the province of Ontario. The parameters considered were (1) the estimated distance from patient's home to actual telemedicine site attended for the teleconsultation; and (2) the estimated distance from patient's home to the consultant site if the patient were to have attended in-person. Geographic coordinates were obtained using postal code data of the patient's residence, telemedicine site, and consultant hospital site. Google Maps™, the Web mapping site used for this investigation, is well known and widely used. 10 Travel distances were calculated in kilometers for each teleconsultation using the Google Maps travel calculator tool.
The following assumptions were made to facilitate the analysis: car travel only and average journey time under normal driving conditions. The type of road, the route taken, the time of travel, the weather, and the type of vehicle, which can all influence journey time, were not considered.
GHG Emission Calculation
Avoided GHG and pollution releases were estimated using emission coefficients provided to Metrolinx (an organization responsible for regional transportation planning in the Greater Toronto Area) by Transport Canada. 11,12 The coefficients estimate the amount of GHG (CO2, methane [CH4], and nitrous oxide [N2O]) and air contaminants (PM, sulfur oxides [SO x ], and NO x ) released per vehicle kilometer traveled by gasoline-powered cars and are based on the latest available data from 2005. To calculate CO2eq, CH4 and N2O were considered to have global warming potentials 21 times and 310 times, respectively, greater than CO2. 13 CO2 emissions were calculated by multiplying the kilometers avoided by the emission coefficients provided by Metrolinx. This was repeated for CH4 and N2O, multiplying by the applicable global warming potential. Total GHG emissions in CO2eq were then calculated by adding the results for CO2, CH4, and N2O.
Videoconference Unit Energy Consumption Calculation
To estimate carbon dioxide emissions associated with use of videoconferencing equipment, a Watts Up Pro meter was used to obtain sample electricity demand (i.e., watt) values for devices. A 32" LCD videoconference unit was selected to conduct this investigation. It is recognized that unit sizes vary and may be smaller than a 32" LCD; however, the larger model is useful in demonstrating maximum energy consumption. Based on electricity consumption, annual CO2eq were estimated using 2006 emission factors (in grams CO2eq/[kW h]) for Ontario from Environment Canada's National Inventory Report: Greenhouse Gas Sources and Sinks in Canada, 1990–2006. 14
Personal Cost Factors
Cost avoidance was calculated in Canadian dollars (CAD) and estimated using the following assumptions reflecting the time period of the study. For cost calculation, the car factors assumed the following parameters: $0.885 CAD gas cost ($/L); 10 fuel efficiency (L/100 km). A sensitivity analysis incorporated fuel costs up to $1.20 CAD ($/L) and a fuel efficiency up to 12 (L/100 km).
NHTG Program
An additional cost factor of relevance for this sample is the NHTG. Advanced Canadian healthcare services are concentrated in larger urban centers, and provincial health ministries subsidize travel for necessary care. 15 Therefore, northern Ontarians who reside in underserved communities and townships may be eligible for assistance from an NHTG to alleviate their travel costs to access specialized healthcare. In fiscal year 2008–2009, the Ontario Telemedicine Network estimated the travel distance avoidance for northern Ontarians who would otherwise be eligible to receive assistance from the NHTG, at over 36 million km if the patients attended an in-person appointment instead of using telemedicine. 16 The NHTG Program is funded by the Ministry of Health and Long-Term Care of Ontario and helps pay some of the travel-related costs for northern Ontario residents, who must travel at least 100 km one way for medical specialist or designated healthcare facility services that are not locally available. 15 This grant is currently paid at $0.41 per kilometer based on return road distance travel between a patient's area of residence and the location of the nearest medical specialist or designated healthcare facility that can provide the service. 15 In addition, the NHTG Program provides an accommodation allowance of $100 CAD per eligible trip to patients whose one-way road distance is at least 200 km. 15 Although it was not the aim of the present study to collect information on NHTG costs, this information can be approximated using the patient's residence data.
Results
Figure 1 presents the patients' residence postal codes on a digital map of Ontario to illustrate the span of the patient population in this study.
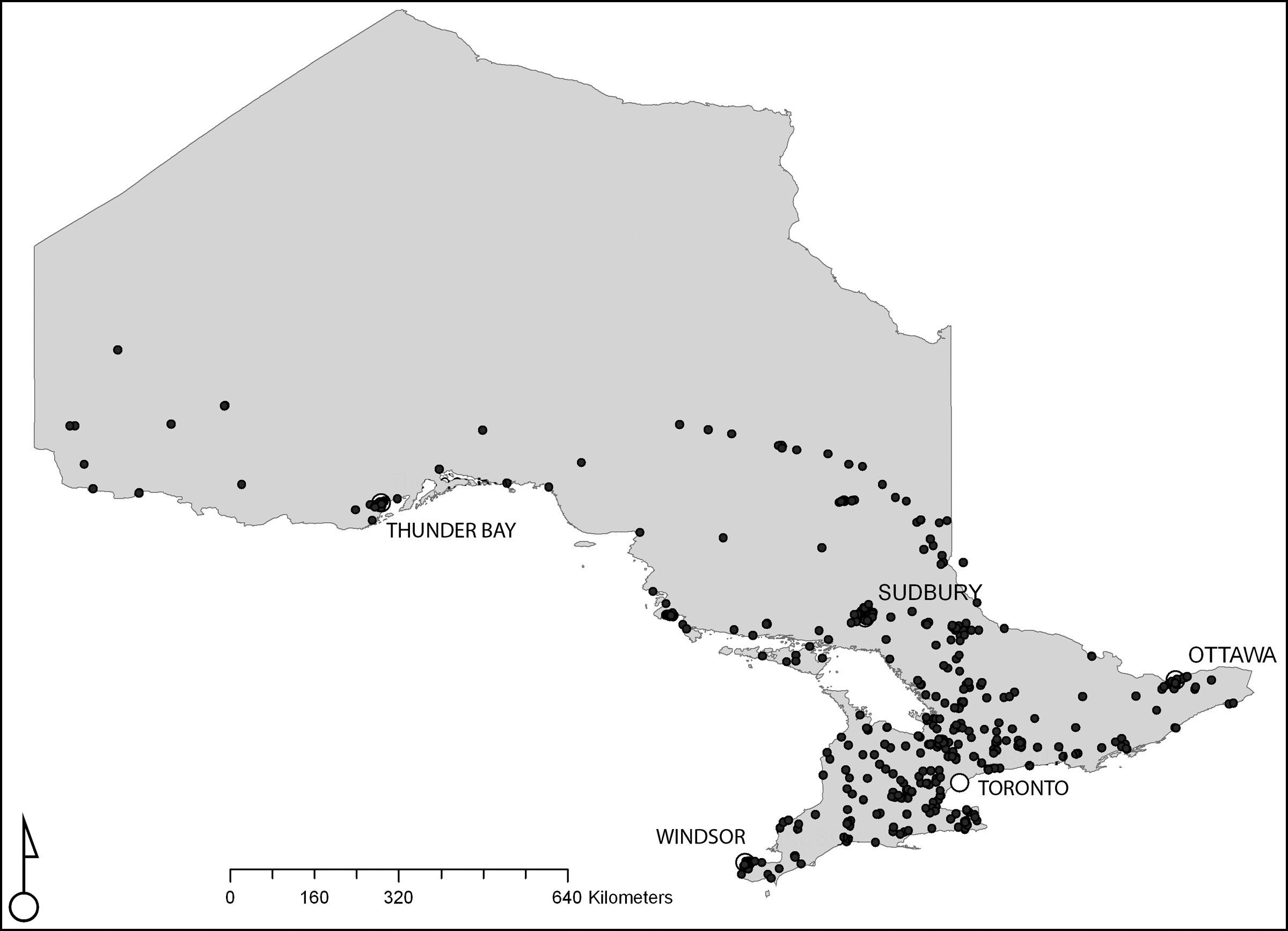
Map of Ontario showing the location of residence based on postal codes. Source: DMTI Postal Code Suite 2008.
The total distance traveled from the patient's residence to the consultant hospital site for 840 teleconsultations in the sample was estimated to be a total distance of 397,140 km one way (mean = 473 km, SD = 408 km). In comparison, the total distance traveled from the patient's residence to the telemedicine site attended was estimated to be a total of 18,523 km one way (mean = 22 km, SD = 51 km). The travel distance avoided was derived by subtracting the two distances, which is a total of 378,617 km one way. Therefore, the total travel distance avoided including return trip was estimated to be 757,234 km.
GHG Emissions
GHG emission avoided was approximately 185,159 kg or 185 metric tons of CO2eq. Approximately 360 kg of other air pollutant emissions (PM, SO x , and NO x ) was avoided.
Videoconferencing Energy Consumption
To estimate GHG emissions associated with use of videoconference equipment, a 32" LCD videoconferencing unit with a measured electricity demand of 138 watts was selected to calculate energy consumption. A 1-h appointment, using a single device, would use 0.138 kW h and generate 0.02 kg of CO2eq. Taking into account the energy consumption of two telemedicine videoconference units (telemedicine unit at the patient site and telemedicine unit at the consultant site) for the 840 teleconsultations would give us a total consumption of 232 kW h with 42 kg of CO2eq emitted for this sample. The estimated cost of electricity used to operate the videoconference units would be $20.88 CAD (based on a rate of $0.09/kW h) for this 6-month sample. Therefore, the overall GHG emissions associated with videoconferencing unit energy is minor when compared with those avoided from vehicle use.
Personal Cost Factors
Estimated consumer gas savings based on average fuel efficiency factors totals $67,015 CAD. Using the upper range of our sensitivity analysis, the estimated total is $109,042 CAD (Table 1).
Personal Gas Cost Sensitivity Analysis
Gas costs are in Canadian dollars and reflect the prices during the study period.
NHTG Program
In the present sample, 282 teleconsultations involved northern Ontarians who reside in an eligible township and potentially could apply for assistance from NHTG. The total travel distance from the patient's residence to the consultant hospital was estimated to be 430,068 km with return trip. The NHTG has a deductible for first 100 km of travel distance. 15 Therefore, the total chargeable distance is 401,868 km and equals the travel cost of $164,765.88 CAD. If we assume that accommodation assistance was warranted, a total of 279 visits would be eligible and result in an accommodation travel cost totalling $27,900 CAD. The total cost avoidance for the NHTG program is estimated to be $192,665.88 CAD.
Discussion
The present study is an important addition and complementary to the existing literature. The study found that the use of telemedicine reduced travel distances by a total of 757,234 km and resulted in a GHG emissions avoidance of 185 metric tons of CO2eq in vehicle emissions. In addition, the formula used to calculate GHG determined a broad range of pollutants as well as the customary CO2 emissions. Approximately 360,444 g of other air pollutant emissions was also avoided. However, videoconferencing units also generate emissions. The present study also estimated the GHG emission due to energy consumption by videoconference units to be 42 kg of CO2eq for this sample. Consequently, videoconference units' power consumptions resulted in having a minor effect in comparison to GHG emissions produced by automobiles. In addition, the practical use of a Web mapping calculator tool Google Maps provided an inexpensive and readily accessible measurement tool to estimate travel distances especially in large-scale patient populations, whereas other studies had used standard and average calculations.
The present study is only the tip of the iceberg in investigating empirically the impact of telemedicine on GHG emissions. Apart from the present study, there is no empirical research that involves the measurement of energy consumption of telemedicine videoconferencing equipments. Alternatives to automobile travel, such as rail or air, should be included as part of energy consumption calculations for future research.
Conclusions
Environmental benefits are clearly an additional reason to implement and support telemedicine services. Patients, providers, payers, and government agencies should consider environmental factors in planning and utilizing telemedicine services. Programs and researchers must refine models and metrics to evaluate GHG emissions associated with travel to provide more accurate assessment of the environmental benefits of specific programs. The methodologies employed in the present study can be generally applied and incorporated into telemedicine expansion and carbon emission reduction strategies.
Footnotes
Acknowledgments
The authors thank Kambria Ernst, Frances Hoy, Sharon McGonigle, Sheryll Nelson, and Ferdous Noman for their contributions and support.
Disclosure Statement
No competing financial interests exist.