
Abstract
Despite some clinical, economic, and other qualitative advantages associated with remote cardiac device monitoring systems, one of the main challenges concerns the management of the out-of-hospital data. Manual updating of hospital databases with the data stored in the manufacturers' servers increases time requirements and may introduce mistakes in the entries. The use of communication standards such as Health Level 7 for data interchange could provide a safe and easy way to access patient and device information. The present study of 38 patients was carried out with the Carelink® remote monitoring technology. A formal process for remote cardiac device monitoring was established, including some features in the Arrhythmias Information System: mobile phone and e-mail were included for communication between patients and hospital, with a new gateway for automatic message sending. Device reports generated through the manufacturer's application were attached to the patient's record. Once the information concerning the transmission session was reviewed, the physician made a medical report, which was sent via post and e-mail to the patient. A new interface was created for Health Level 7 communication with the manufacturers' applications, so that the Arrhythmias Information System could automatically interchange information concerning the device and/or the patient when this kind of communication system is available. The volume of data generated by system warning alerts and transmission sessions makes it very difficult to meet the hospital database updating requirements. Standard-based communication between hospital and manufacturers' applications is fundamental to automatic and reliable update of data.
Introduction
The increasing number of implantable cardioverter defibrillators (ICD) and cardiac resynchronization therapy devices (CRT-D), as well as the greater complexity of such implantable devices, has created a major problem for clinic follow-up programs. These devices have to be reviewed a minimum of 3–6 months interval program, causing significant burden for hospital resources. 1,2
Nowadays, physicians can use new tools such as remote monitoring systems, which offer the possibility of reducing the number of visits that patients must make to the hospital of clinic for standard follow-up procedures. 3,4
Such tools, which allow physicians to review the remotely collected data from the patient's home through a Web-based platform, have proved to be very safe and reliable. 5,6
This technology also enables continuous monitoring of ICD and CRT-D, thus allowing for early detection of device-related problems and prompt clinical intervention if necessary. 7 –9
Detailed research has shown very positive results regarding the level of satisfaction of patients and physicians when using such tools. 7,9
Regarding cost analysis, remote monitoring technology may help healthcare systems by reducing the time physicians and/or nurses dedicate to conventional monitoring procedures, replacing about half of the scheduled visits to the hospital of ICD or CRT-D recipients with remote data collection sessions. There are also other cost savings related to remote monitoring, such as patient transportation costs. 7,9 –11
The main challenge for remote monitoring systems may be the management of the collected data (either device- or patient-related data). 2,12,13 Hospital databases must be updated manually through specific applications and Web sites provided by each device manufacturer, thus increasing time commitment and the risk of errors from manual data retrieval.
The use of standards of communication between manufacturers' and hospitals' applications, such as Health Level 7 (HL7) 14 standards, would allow for automatic and safe data interchange and could alleviate workload related to data management. 9
Methods
A study was carried out between June 2007 and December 2008, analyzing safety, reliability, and economic aspects of a remote monitoring system based on the Carelink® (Medtronic) technology.
Patients' view on the system reliability, performance, and ease of use concerning the new monitoring system was surveyed. Some results of this survey were considered in the design of the new process. 15
At the end of December 2009, 85 patients (cardiac device recipients) were put under a remote follow-up program. The new process was defined by the following features: ICD or CRT-D were monitored in the clinic at 1 month after implantation and again after 7 months. Remote follow-up sessions were then scheduled for the following 18 months, with transmissions arranged every from 3 to 6 months. Scheduled and physician-authorized (nonscheduled) transmission sessions were performed. Nonscheduled transmissions were usually requested by the patient in the event of an acute episode. Patients receive a Short Message Service (SMS) message before and after the scheduled transmission session. After each scheduled session, patients received a report, via post or e-mail when available, containing the results of the device revision. A continuous remote monitoring was performed for heart failure patients. Different warning alerts were set according to their severity criteria: yellow (battery status, low/high left ventricular pacing lead impedance, ventricular accelerated arrhythmia episode, etc.) and red (limited battery capacity, low/high shock lead impedance, low/high right ventricular pacing lead impedance, etc.). Warning alert messages were automatically sent through each manufacturer's application, either by e-mail, telephone, or fax. Physicians then reviewed the data concerning these warning alerts and patients were contacted when necessary, although no medical report was sent. All patients were requested to sign a specific informed consent document to accept remote monitoring.
The Arrhythmias Unit developed its own software, consisting of a Relational Database and its Graphical User Interface to store and manage patient and procedures information. This system has independent modules for electrophysiologic studies, ablations, ICD and CRT-D, pacemakers, and other procedures.
Common graphic data were captured from the Hospital Information System (HIS) through HL7 messaging (Admit Discharge Transfer messages). To achieve a full implementation of the new remote follow-up program in the current information system, the following actions were taken: The Arrhythmias Relational Database and Graphical User Interface were completed to include the previously mentioned workflow. As far as demographics are concerned, a mobile phone number was mandatory, whereas patient's e-mail was optional. A new gateway was implemented for automatic SMS and e-mail sending. The schedule for programmed remote follow-up sessions was automatically generated and sent to the HIS, via HL7 (Scheduling Information Unsolicited messages). The specific agenda for the remote follow-up program was used to recover clinical activity as well as to manage patient's visits portable document format (Adobe Systems®) device reports for new transmission sessions. These reports were then stored in a public folder. Once a new report was stored, a confirmation SMS message was sent to the patient and the portable document format file was attached to the patient's record. Nonreviewed transmission sessions appear in the information system as a pending task. The physician reviews transmission data and completes the medical report, printing it for postsending. This medical report is automatically sent by e-mail when available.
As far as the HL7 communication with the manufacturer's application is concerned, a new interface has been created, complying with the manufacturer's conformances, capable to integrate Outbound Event Observation Reporting and Scheduling Information Unsolicited messages. These messages could be used to send all the information concerning the device performance in all scheduled transmission sessions, as well as in those required by physicians or triggered through the warning alert system. Data would then be automatically updated at the hospital database, eliminating connections to different Web sites and manual entries. Figure 1 shows the links between main stakeholders and information systems related to remote monitoring process.
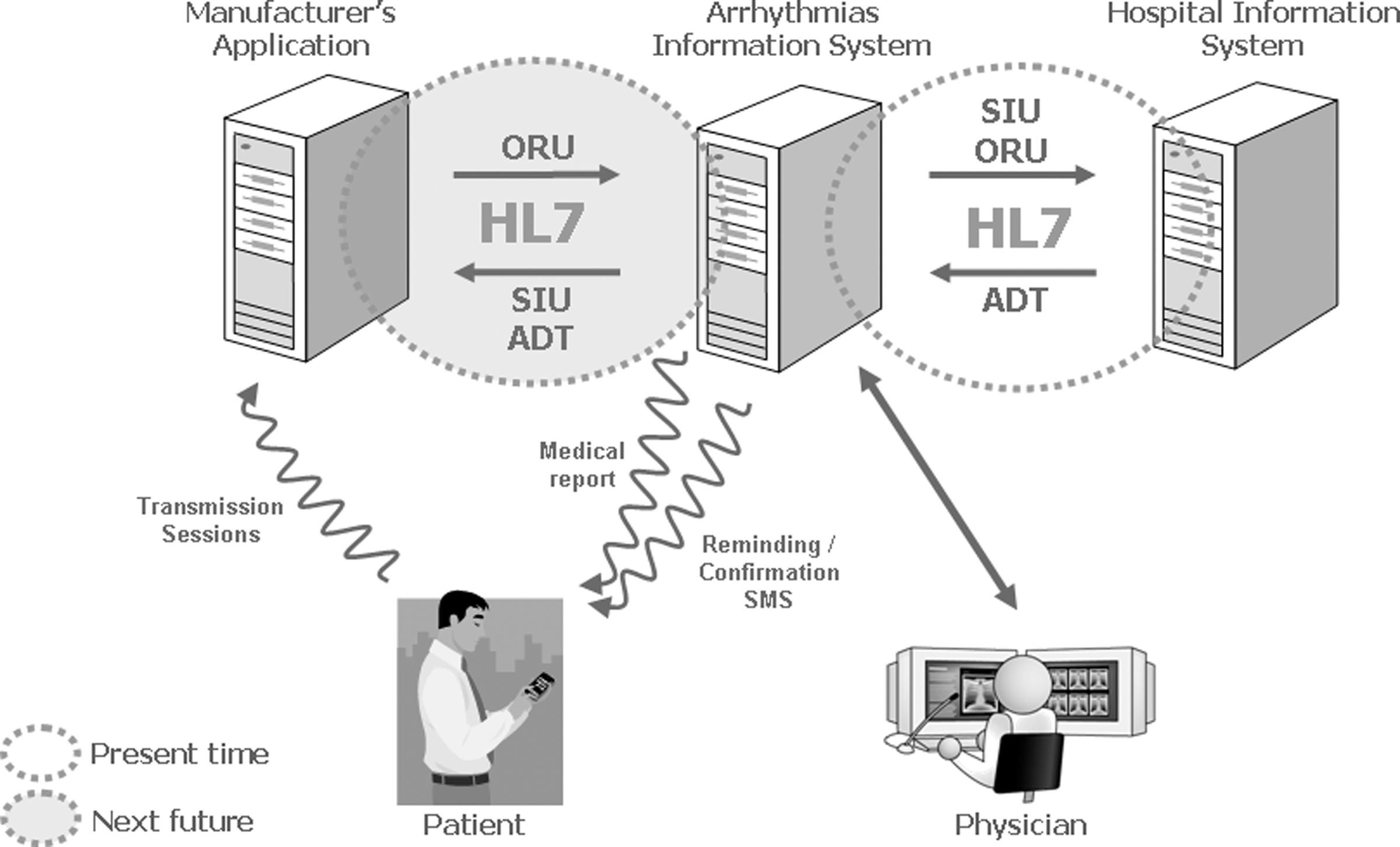
Communication between patients, physicians, and different information systems concerning remote monitoring process. HL7, Health Level 7 communication standards; ADT, Admit Discharge Transfer messages; SIU, Scheduling Information Unsolicited messages; ORU, Outbound Event Observation Reporting; SMS, Short Message Service.
Results
In September 2009, a first version of the Arrhythmias application was finalized and ready for testing. By the end of that same year, 89 complete transmissions had been performed. Communication with the HIS, associated with this first set of transmissions, reported no errors, and only some minor improvements were required to enable the automatic attachment of transmission files to each patient record. A new software version, including such improvements, has been running since early 2010, with a total of 165 programmed consultations and 82 transmissions already performed and reviewed through June 2010, all of them with no information management or transmission errors.
Conclusions
A reliable information system contributes to a complete implementation of a new process such as remote cardiac device monitoring.
Some communication links, including SMS messages and medical reports between the patient and the hospital personnel, which were very appreciated by the patients, can be included as part of the duties of the information system.
As long as there is no automatic and standard communication with the device manufacturers, the burden of the data generated by system warning alerts and transmission sessions makes it very difficult to meet the hospital database updating requirements.
HL7-based communication between manufacturers' or other external applications and HIS is crucial to achieve consistent and safe update of data related to device performance and/or different patient's parameters.
Footnotes
Disclosure Statement
No competing financial interests exist.