
Abstract
Introduction
In Manitoba (Canada), the telehealth network provides a range of services within a wide range of medical specialties and sub-specialties. Since 1999, telehealth technology has been utilized for the assessment of fetal alcohol spectrum disorders (FASDs). 1 Partnerships to provide FASD assessments via telehealth were formed with two rural and remote communities: The Pas/Flin Flon in 2000 and with Norway House in 2003. A necessary component of the implementation of telehealth, as described by the Institute of Medicine, is the evaluation of clinical and social effectiveness. 2 To improve access and services, it is essential that telehealth programs are evaluated. 3 This is especially important within the field of FASD, given the stigma attached to the diagnosis 4 and the complex nature of the assessment. 5 The purpose of this study was to evaluate the FASD telehealth program with The Pas/Flin Flon and Norway House by comparing community practices from the perspective of professionals involved with the program in the communities.
FASD is an umbrella term that encompasses three specific medical diagnoses that result from prenatal exposure to alcohol: fetal alcohol syndrome (FAS), partial FAS (pFAS), and alcohol-related neurodevelopmental disorder (ARND). FAS describes those individuals with a characteristic pattern of physical and neurological birth defects, including facial dysmorphology, growth deficiency, and neurobehavioural abnormalities; pFAS refers to those with facial dysmorphology and neurobehavioural abnormalities but no evidence of growth deficiency; ARND pertains to those individuals who have characteristic neurobehavioural abnormalities but no dysmorphology or growth retardation. 5 The spectrum of brain differences with FASD varies by individual and may cause different learning, behavioral, and daily living challenges for each. Children who are seen, either in-person or via telehealth, for multidisciplinary diagnosis through the Manitoba FASD Centre are diagnosed using the Canadian Guidelines for FASD Diagnosis. 5
Referral, Assessment, and Follow-Up Processes
Norway House and The Pas/Flin Flon, both rural and remote Northern communities with populations <6,000, can use telehealth once per month for either an assessment or follow-up session (see Figure 1 for process).
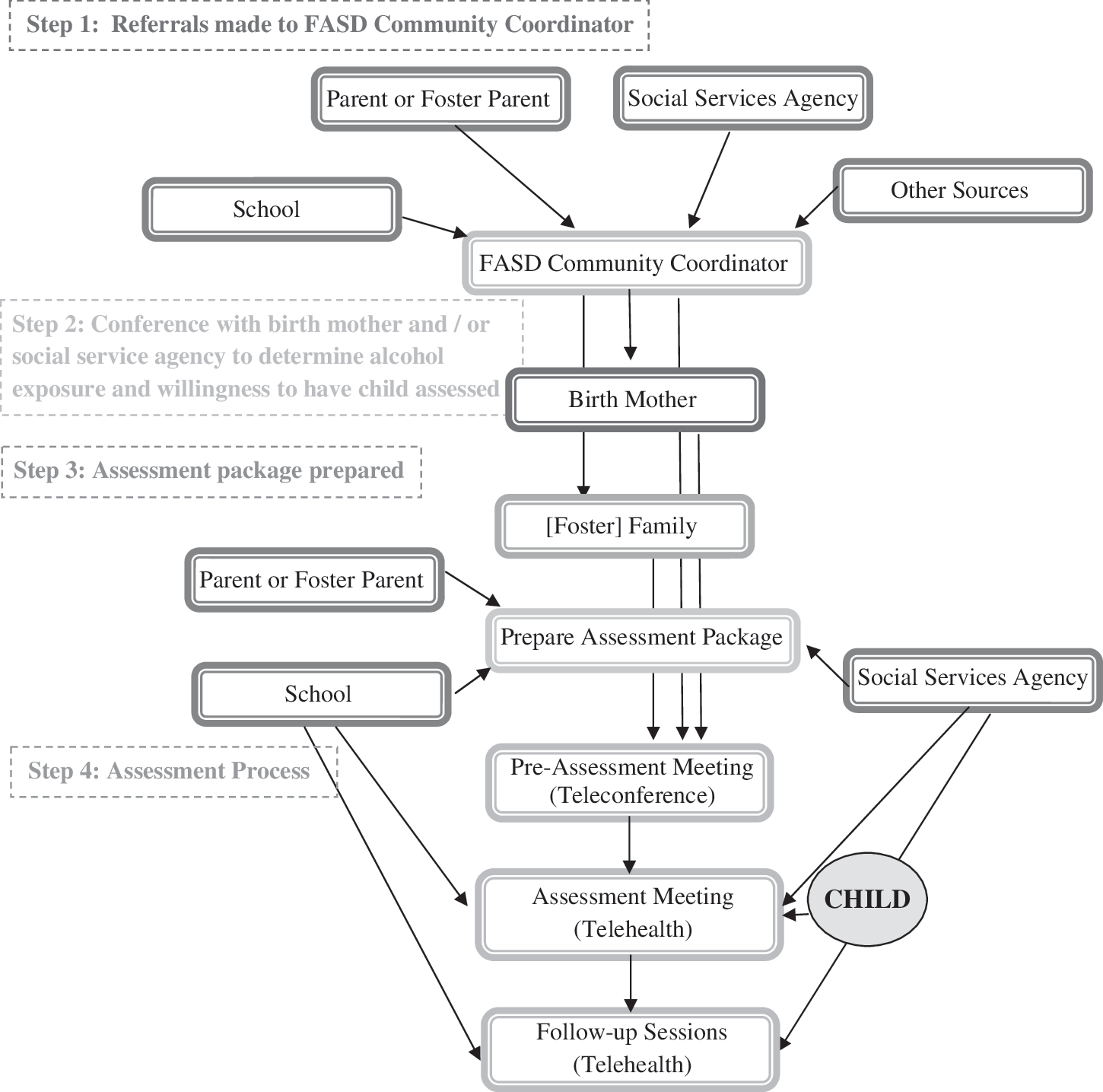
Using telehealth: From referral to assessment.
From 2005 to 2009, 41 FASD telehealth sessions have been conducted with the two communities. In Norway House, 20 assessments have been conducted since November 2005; 12 (60%) have resulted in a diagnosis of ARND, 2 (10%) of pFAS, 1 (5%) of FAS, 2 (10%) with a deferred diagnosis,* 1 (5%) was incomplete, and 2 (10%) of the resulted in non-FASD diagnoses. Of the 21 assessments completed in The Pas/Flin Flon, the majority (12 or 57%) resulted in diagnoses of an ARND, 2 (10%) were diagnosed with pFAS, and 7 (33%) were either deferred or provided a non-FASD diagnosis.
Materials and Methodology
This study utilized qualitative techniques to evaluate the use of telehealth in the field of FASD by two Manitoba communities. Semistructured interviews were conducted from October 19 to December 11, 2009. Participants (N = 26) were comprised of professionals from the communities and Manitoba FASD Centre team members. Community members were approached to participate in an interview if there had been involvement with the FASD telehealth process within the previous 5 years. Only one individual chose not to participate due to scheduling conflicts. It was typical that community participants had attended up to three sessions over a 5-year period; the three FASD team members had participated in more of the assessments. The small community samples indicate that there were few people involved in this process as attempts were made to contact all participants known to the telehealth coordinators. Likewise, the sample size of FASD team members was a direct reflection of the small group of practitioners involved in telehealth FASD assessments. Interview data were digitally recorded and extensive notes were taken in each session. The qualitative data were analyzed thematically using a method described by Shank, 6 which involves an ongoing search for patterns within the data toward the formation of themes. General findings or common aspects in each community were identified.
The analysis was completed manually as opposed to with the aid of a computer program as the transcripts were manageable using this method. Principles of good qualitative research were attended to, as outlined by Mays and Pope 7 ; data were reviewed by an independent author (AHD) and discussions were held to reach consensus on the themes. The aim was to present data in an authentic manner to capture the experience as detailed by participants.
Results
Participants
Interviews were mostly conducted in the home communities of the participants and were conducted in participant's places of work or at a mutually agreed upon site. The largest representation came from the education sector (18 or 54.6%) and the majority of the respondents were women (n = 30 or 90.9%). Interviews ranged in length from 25 to 90 min with an average of 47 min (Table 1).
Two emerging themes highlighted the experiences of using telehealth for an FASD assessment. The first theme extends primarily from the community participants' experiences and the second contains a mix of both community participants and physicians' interview data.
Demographics of Study Participants (n = 26)
Theme #1: Benefits Outweigh Drawbacks
Benefits
FASD assessment via telehealth was regarded as an effective solution to participating in a diagnostic process while living in a remote setting. With telehealth, the assessment took place in the child's own community and a greater number of participants could be involved. The process was also perceived to create a stronger network of caregivers.
The costs, both financial and social, were perceived to be greatly reduced with telehealth. In-person sessions could generate extensive travel, accommodation, and childcare costs, for example, which could be overwhelming for families. Additionally, being in the city for medical appointments was described as being stressful. Social costs, or the implications associated with things like missing work and school, the removal from a place of comfort, and the lack of a support system, were also described by participants. The overall costs with telehealth were much reduced.
Participants described how the medical team was able to develop rapport with the remote group, a perceived benefit with the telehealth service. Physicians were described as attentive to each individual's responses and interested in feedback by all participants.
Drawbacks
The technology could cause frustration or anxiety for some respondents. Problems like pixilated pictures, difficulties maintaining the connection, or general unease with the technical aspects were described. Having the telehealth coordinator—the individual responsible for the telehealth videoconferencing—available for immediate technical assistance allowed participants to focus on the clinical assessment, but this was not always feasible. As the equipment was typically used once a month or less, very few participants were perceived to have mastered the technology.
Respondents also expressed concern over the medical language used in the assessments. It was perceived that participants had some difficulty understanding the discussions due in part to language barriers and perhaps perceived difficulties in communicating via the link. Translation services were provided inconsistently and by untrained community members.
Theme #2: Dreaming of Change
The perception was that certain elements could have benefitted from further development.
A dedicated space for the child
Typically the child is not present for the complete telehealth session. In some cases, the child is brought back to school but often he or she often remains at the telehealth site for the entire duration. This was perceived to create discomfort for the parent still involved in the telehealth meeting as well as the child who was separated from his or her caregiver.
An inviting and welcoming environment
Telehealth sessions were typically hosted in hospital boardrooms. It was perceived that such a setting, besides being foreign for some of the participants, was not conducive to sharing detailed personal information as required. Participants suggested that a home-like setting would relax participants. The importance of providing a welcoming and respectful environment, in particular for the older participants, was stressed.
The physicians' perspectives
Barriers did exist in some cases that could not be overcome via telehealth. For example, the inability to conduct a full developmental assessment including a physical examination deterred some assessments from being completed over the link.
The medical team is typically much smaller than the remote group, making it more difficult for the medical team to see the entire group on the telehealth screen. Even with the equipment's panoramic capabilities, the visual acuity in group sessions was described as reduced, making it challenging to read visual cues as well as assess dysmorphology. Physicians suggested that a priority was to improve clarity. This might be achieved through furniture reconfiguration, better training with the telehealth equipment, and improved equipment.
Discussion
This is the first study designed to understand the role of telehealth in remote communities for the purpose of an FASD diagnostic assessment. Participants in this study described how the use of telecommunication provided a critical and creative service in this sensitive field. It was clearly expressed that the perceived benefits of using telehealth services for children, families, and service providers outweighed the limitations. Altering several aspects of the services could eliminate a number of the perceived drawbacks.
Addressing Barriers for Children
Central to the findings was the role of the child in the telehealth diagnostic process. Using telehealth as the assessment medium was felt to support the best interests of the child; keeping the child in a familiar environment surrounded by their family and their support network was described as positively contributing to the diagnostic process in remote communities.
The pragmatics of the assessment process was not always described as being ideal for the child. Structural inadequacies inherent in the local facilities, both during the assessment and while the child was not actively participating, were identified. Further challenges of the use of this technology during the assessment were described by physicians, including the difficulties in being able to conduct an effective developmental assessment as a direct result of using telehealth. On the basis of the themes emerging from this study, it is important to consider the central role of the child in the structure of the assessment process itself. Thus, restructuring of the local assessment sites to facilitate child comfort and developmentally appropriate supervision while telehealth was occurring should be considered in telehealth programs dealing with children and families. Comfort level of participants has been shown to be a significant predictor in satisfaction, 8 suggesting that an important element of telehealth conferencing is participant preparation especially as it pertains to the family's ability to direct the process to meet the needs of their child.
In addition, adapting local clinical sites to meet the medical requirements of dysmorphology and developmental assessments of children are crucial to the success of the medical assessment. The complexities of this type of multidisciplinary assessment may require in advance communication between community professionals and the medical diagnostic team to appropriately adapt the site for successful telehealth assessment.
Addressing Barriers for Family Members
Previous research has indicated that telehealth is well received within child health settings and has been utilized in a wide range of pediatric medical specialties and sub-specialties. 9 A recent qualitative study found that the use of telehealth both reduced the burden and maximized supports for telehealth users. 10 Although challenges such as additional training for healthcare participants or general organizational issues have been described, 11,12 telehealth is recognized as a valuable method to bring healthcare closer to remote communities lacking in healthcare services. 9 Persistent barriers in the use of telehealth within Canada include being low income, from an ethnic minority group, being a rural resident, and speaking a minority group language, 13 all descriptors that may apply within the communities that are accessing telehealth for FASD assessment. Participants in this study described how parents, grandparents, foster parents, and other members of the support team spanned generations and cultural backgrounds. Some of the participants did not speak English as a first language and all were living in remote regions of the province. Many of the families involved were described as relying on social assistance.
It was felt that the majority of the people attending the sessions would not be familiar with teleconferencing, so attending a telehealth conference may have been viewed with uncertainty. For others, simply attending a medical appointment would create some unease. It was perceived that the families participating in telehealth assessments would like associate a stigma to the diagnosis of an FASD. Thus, participants may experience apprehension for any number of reasons. Spaulding et al. 8 stress that apprehension before and during a telehealth conference is not unusual. However, it may be exacerbated given the social, behavioral, and physical implications implicit within an FASD diagnosis. 14 In identifying elements for successful implementation of telehealth programs, Gagnon et al. 15 stressed that telehealth must be tailored to fit the unique health and social needs of the community.
Providing a culturally sensitive process was important to participants. One possible solution may be to incorporate Aboriginal elders when appropriate or desired. Part of an elder's role is to provide support and spiritual guidance to families throughout their life journey; in having an Aboriginal elder attend the FASD assessment, he or she could provide additional support to the community-based team. Recent clinical findings, based out of research in the neighbouring Canadian province of Saskatchewan, support the view that traditional elders can impact health-related experiences. 16 In that study, which examined the role of traditional elders in the field of family violence, the authors wrote: “Including elders in the care of people [who have experienced challenges] is effective. We speculate that it helps by providing traditional stories about relationships and roles [that do not include those challenges]. Spiritual approaches within aboriginal communities may be more effective than more secular, clinical approaches.” 16
Other contextual barriers were seen to have a negative impact on the telehealth process. For example, in this study, the telehealth equipment was based in the community's hospital and typically in a conference boardroom; both the setting and the location were seen as drawbacks. Study participants described the negative impact of situational discomfort on the telehealth process and diagnostic assessment. It was expressed that participants who did not feel comfortable in the telehealth setting would not contribute as openly throughout the session in comparison to those feeling at ease. Study participants expressed how minor modifications may go a long way to making those involved more comfortable.
Recent research also highlights the need to plan in conjunction with the community before implementing a telehealth program for children; putting all participants at ease is valuable and has been shown to be a critical element in program planning. 17 On the basis of the experiences of participants in this study, a number of recommendations for multidisciplinary telehealth clinical assessments in remote communities are suggested to improve the experience for participants. First, creating a comfortable and family-centered atmosphere should be emphasized. The schedule for the remote site could include an informal welcome and coffee or refreshment to increase the comfort level of the participants, allay any concerns about the process, and provide a culturally appropriate and sensitive environment. Second, the choice to include an elder, as culturally appropriate, should be offered to parents or guardians. Ideally, the elder should have familiarity with FASD and the telehealth process. This process could be supported by the local community coordinator with the readiness and support of the community. Finally, simple considerations, such as placement of furniture in the telehealth assessment room to create a less formal atmosphere, may facilitate participant comfort and thus may be more conducive to open communication in these clinically sensitive assessments.
Addressing Barriers Identified by the Medical Team
The Canadian guidelines for FASD diagnosis 5 were created after extensive consultation of expert practitioners working in the field of FASD. These guidelines reinforced the need for a comprehensive multidisciplinary approach in the assessment and diagnosis of individuals who may have an FASD. The medical diagnosis requires careful consideration of dysmorphology and growth, as well as a comprehensive assessment of neurobehavioural functioning. 5 The physicians who participated in this study identified some difficulties with technical aspects of the assessment. Challenges with the clarity of the picture were seen to impact the assessment of dysmorphology and could result in the need for a subsequent in-person assessment, thus increasing the costs involved with leaving one's geographic community and support system. Remote sites need to additionally consider the comprehensive needs of the medical team required by this unique diagnosis in their assessment of the child to best facilitate the diagnostic assessment. To facilitate the diagnostic assessment, this study supports the need for a preassessment planning meeting between the medical team or their designate and the local community coordinator to discuss the specific assessment planned and discuss the medical team's session requirements. This would also allow for discussion of unique aspects of family and community dynamics that may impact the interpretation of assessment findings to best meet the needs of the family and community on the telehealth day.
Limitations of Study
The purpose of this study was to evaluate the FASD Telehealth program within two rural and remote communities. The participants involved in the study included the medical staff based at the Manitoba FASD Centre, school personnel, social services representatives, and telehealth staff. This study was not designed to evaluate the perspectives of children and their families who have been referred for FASD assessment. This critical perspective will be extremely important as the telehealth program expands within the province; understanding whether an FASD assessment via telehealth contains unique aspects, possibly related to the stigma of a diagnosis, will be paramount. Further research would be useful to gain a stronger understanding of the experiences of the individuals and families served by telehealth assessment.
Conclusions
This qualitative study is the first to evaluate the use of telehealth in multidisciplinary FASD assessments in remote communities. The perspective of professionals involved in the assessments was chosen to guide implementation of further expansion of a telehealth network in the province. Themes addressed the perceived strengths and drawbacks with the program with meaningful suggestions to improve the service. Participants regarded the FASD telehealth program as successful and useful, especially given the remote location of the communities and the lack of on-site services. The Manitoba FASD telehealth program is a successful assessment and diagnostic program for remote and underserved communities. This evaluation will provide a solid basis for the successful further development of the FASD telehealth program in the province of Manitoba.
Footnotes
Acknowledgments
We would like to thank the Changes for Children Initiative for funding this study and Healthy Child Manitoba for their direction and support. We are grateful to the participants from The Pas, Norway House, and the Manitoba FASD Centre as well as the FASD Community Coordinators in The Pas and Norway House.
Disclosure Statement
No competing financial interests exist.
*
A deferred diagnosis most frequently occurs in a young preschool child who presents for assessment with a confirmed history of prenatal alcohol exposure but who is too young for comprehensive neuropsychological assessment of brain domains.