
Abstract
Introduction
The role of social networks in determining health was first studied in the 1970s, when researchers demonstrated that they could affect mortality; the mechanisms involved in this influence include social support, social influence, social engagement, person-to-person contacts, and access to resources. 1 The most widely researched network effects are dyadic effects, especially spouse pairs, followed by nonspousal relationships, such as parents and children or best friends. As Smith et al. state, the new frontier of social network research is the “realm of supradyadic effects,” 1 which have started to reveal a kind of person-to-person contagion of biobehavioral traits, such as in the spread of obesity. 2 Social network analysis has therefore been mentioned as a useful tool for designing more appropriate health prevention programs. 3
As Internet usage increased and interactive tools emerged, the idea that “when a computer network connects people, it is a social network” has come out, as well as the idea that social network analysis could be useful for understanding these computer-mediated interactions. 4 As a new object of research, online social networks need new models to be studied, in terms of tools for data capturing and analysis. 5
In 2001, the debate about the benefits and disadvantages of online support in the field of health concerned the so-called “comprehensive online support services” (limited to experimental research projects) and “private single function forums,” which included private bulletin boards, chat rooms, and mail groups—rudimentary tools that had the specific feature that was to become one of the main characteristics of Web 2.0 as being open to all interested parties. 6 Since then, the participatory Web developed to create virtual worlds and virtual communities, with specific involvement in the field of health. On one hand, the opportunities of the virtual worlds as Second Life® in terms of public and environmental health have been discussed 7 ; on the other, the enormous challenges represented by online social communities of patients started to be recognized. In particular, the themes of patient participation and the emergence of personal health record systems have been tackled, considering the unprecedented potential in terms of patient empowerment and research data collecting, not forgetting the complex privacy issues these new tools create. 8
A 2004 review assessing the effects of online peer-to-peer interaction failed to find robust evidence of the health benefits, although many limitations of the selected studies were identified. 9 Besides, a study on the quality of user-generated health information on health social networks found that about half of the postings had medical contents, and 54% of them were either incomplete or contained errors that were potentially clinically significant in 85% of cases. 10
In the United States, the findings of the National Cancer Institute's Health Information National Trends Survey 2005 revealed the use of online support groups by only 3.8% of participants. 11 This was significantly predicted by worse health status, access to Internet primarily from home, and lower income. The authors explain that it seems an infrequent activity citing the general decline in online chat room participation, but they also hypothesize that the survey underestimated the data, due to the method adopted, which could have led the participants not to include in online support groups such activities as forums, online communities, chat rooms, and blogs.
Besides the question of the efficacy of these tools and how many people use them, to our knowledge the literature contains no overview of online health social networks or a description of their characteristics. So, to analyze existing online social networks dedicated to health issues, we performed an active search on the Internet for such Web sites and analyzed their features according to the content analysis method.
Methods
The study was performed in September and October 2009. We analyzed a sample of health social networks for patients, selected using the Altavista©, Bing©, Google©, and Yahoo© search engines, with the following key words: “Online health communities,” “Health communities for patients,” and “Medical social networks.” The first 100 references were analyzed for each set of keywords, so we ended up gathering 1,200 references (4 search engines × 3 search terms × first 100 references).
We selected Web sites that act as health social networks (or health social communities), that is, ones enabling users to subscribe, create a profile, insert personal health data, access other members' data, and get in contact with them. In other words, we were interested in Web sites similar to Facebook in their structure and their functioning, but with a special focus on diseases and health conditions.
To ascertain the durability of the Web sites, their existence on the Web was re-checked in August 2010.
The selected social networks were coded using an ad hoc codebook, according to the content analysis method. 12 The codebook was elaborated to investigate four areas, since analyzing a social network Web site gives access to two kinds of information: Web site characteristics, since the social network could not exist without a Web site, and information about the social community made available on the Web site.
The four areas of the codebook are General information: name and Web address. Technical characteristics and utilities: extension of the Web site address; presence of copyright and/or trademark symbols, and access quality certifications (W3C-WAI,W3C-CSS, and W3C-HTML) or other technical certifications; presence of the Health On the Net (HON) foundation's logo as evidence of the reliability and credibility of the medical information provided by the site; access counter; accessibility tools, including the presence of a site map and internal search engine; availability of the contents in different languages; presence of contact details (e-mail, post, telephone, and fax) and references or links to other social online communities, not related to health. Characteristics of the Web site and general contents: declaration of the Web site's authors, sponsors, or partners; history of the social network, team running the Web site, and professional profiles of the team members; declaration of terms of use, disclaimers, mission, privacy policy, and usage of patient data; presence of a financial report and a press room; links to other Web sites, news area, and scientific research area; chance to subscribe to a newsletter or RSS RDF (Resource Description Framework) Site Summary feed; presence of a frequently asked questions (FAQ) section, forum, career section, and merchandizing area. Web site contents related to the online community: number of registered members and Web site themes (on one or more diseases); information on registered patients; presence of marketing statements to persuade users to register as members; presence of information about doctor and hospital contacts; presence of medical information—regarding diagnosis and therapy—and bibliographic references; access to aggregate statistical data about the social network patients.
We performed a descriptive analysis of the data collected. We also attempted to group networks and to compare them. We compared Web sites having at least one quality certification with ones with no certification, monothematic and plurithematic Web sites, Web sites with referral to medical instructions, and ones providing no medical recommendations. These groups were compared as regard help navigating pages; access to the disabled; availability in languages other than English; internal search engine; site map; at least one quality certificate; declaration of authors, sponsors, partners, and managing team; privacy policy; disclosure of the financial report; one or more health themes; research area; hospital referral; referral to specific drugs; or therapeutic information.
All the descriptive and analytical analyses were conducted using the Stata statistical software package (version 10.0; Stata Corporation, College Station, TX).
Results
The research led to a sample of 41 social networks, which are listed in Table 1. All the Web sites in the sample were still active 10 months after the first detection but one (
List of the Social Networks Analyzed, with Their Names and Web Addresses
Technical Characteristics and Utilities
The majority of the Web sites had the extension .com (28 Web sites, 68.3%), followed by .org (11, 26.8%); only in two cases were national extensions used, for Canada and the United States. A trademark symbol (® for registered trademark or ™ for trademark) was present on 17 Web sites (41.5%). The copyright symbol © was shown on almost all the Web sites, 38 (92.7%). Fifteen Web sites (36.6%) had at least one quality certificate, the most frequent being the HON code on 13 Web sites, followed by TRUSTe (a certifier for online privacy seals,
An internal search engine was available on 30 Web sites (73.2%), a site map on 12 (29.3%) and help pages on 8 (19.5%). Three Web sites (7.3%) had text display for the poor sighted. Six Web sites were available in other languages besides English, five partially and one completely; in five cases the language was Spanish, one of the Web sites offering Chinese and Russian as well. One site used the Google translator.
Regarding Web site contacts, 19 Web sites (46.3%) provided a space for suggestions or information about technical problems. The majority of the sample (36 Web sites, 87.8%) gave a way of contacting the Web site. The most frequent method was e-mail or an online form, on 31 Web sites, followed by ordinary mail (26), telephone (17), and fax (12).
With regard to networking with other online communities, 14 (34.2%) of the networks analyzed claimed to be present as a group in at least one other social network. The Facebook symbol was present in 11 cases, Twitter in 11, and Myspace in 2.
The data given here are represented graphically in Figure 1, in order of frequency.
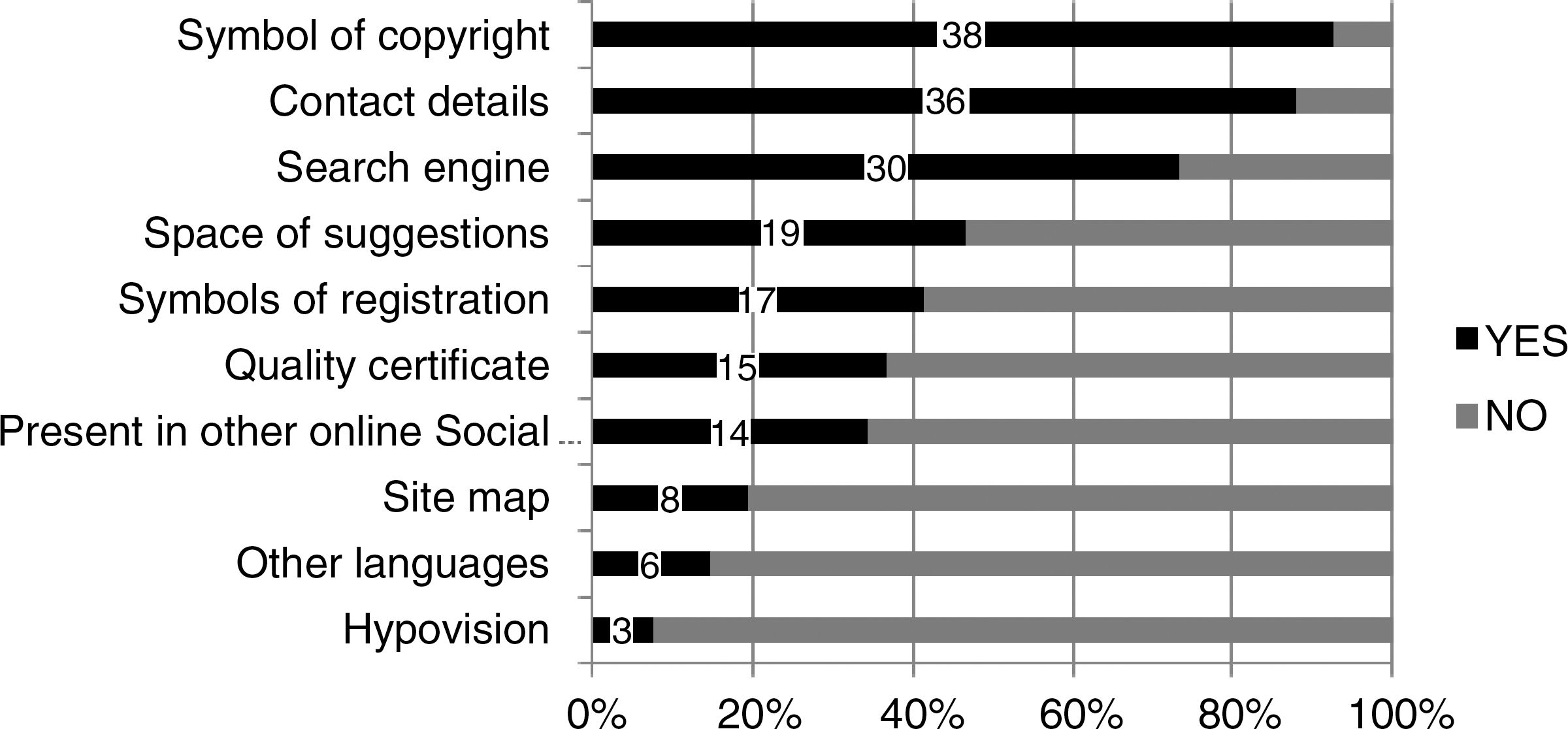
A graphic sketch of the technical characteristics and utilities present on the Web sites, in order of frequency. The absolute numbers of the Web sites where the characteristics are present are indicated, over the total number of 41 Web sites (100%).
Characteristics of the Web Site and General Contents
Five Web sites (12.2%) showed the name of the author or the operating organization. Eight Web sites (19.5%) indicated one or more sponsors, which were pharmacies (five), hospitals (three), associations (two), and universities (two). Nine Web sites (22.0%) had one or more partnerships, with pharmacies (five), associations (four), hospitals (two), and universities (one). Often it was not easy to establish whether the relationship with the collaborating organizations was on of sponsorship or partnership.
A list of the members of the team running the Web site was present in 21 cases (51.2%), the teams most frequently comprising doctors (17 Web sites), informatics experts (7), psychologists (5), journalists (5), engineers (3), and patients (3). The history of the social network was available on 19 Web sites (46.3%).
The mission was declared by 27 Web sites (65.9%), the terms and conditions by 37 (90.2%), and the privacy policy by 39 (95.1%); disclaimers were present on 37 Web sites (90.2%). Two Web sites (4.9%) stated that they would send the collected data to pharmacies and/or institutes. It was declared that the data would be used for research on four Web sites (9.9%) and for marketing on eight (19.9%), by the Web site itself or by the external organization receiving the data.
A financial report was available on 4 Web sites (9.8%) and a press area on 14 (34.1%). Only one Web site required registration before access. To register, the information most often asked for was an e-mail address (90.2%), followed by birthday (58.6%) and name (51.2%).
One-fourth of the sample (10 Web sites, 24.4%) had at least one link, to update news (8 Web sites), associations (4), and universities (1).
A news area existed on 19 Web sites (46.3%). It was possible to subscribe to a newsletter in 15 cases (36.6%) and to an RSS feed in 10 (24.4%). Nine Web sites (22.0%) had an area dedicated to scientific research, and six (14.6%) gave the chance to apply for medical research studies. An FAQ area was available on 23 Web sites (56.1%), an images/video area on 18 (43.9%), and a medical glossary on 11 (26.8%). Ten (24.4%) had a calendar of patient activities. Virtually, all the social networks (39, 95.1%) had a forum.
A careers section was available on 12 Web sites (29.3%), providing details of job opportunities (9) and/or voluntary activities (4).
A quarter of the Web sites (10, 24.4%) received donations, and the same number had a merchandising area (gadgets, books, and so on). Five Web sites (12.2%) sold health-related products, especially medical devices and parapharmaceutical products (four) and over-the-counter drugs and supplements (two).
The data given here are represented graphically in Figure 2, in order of frequency.
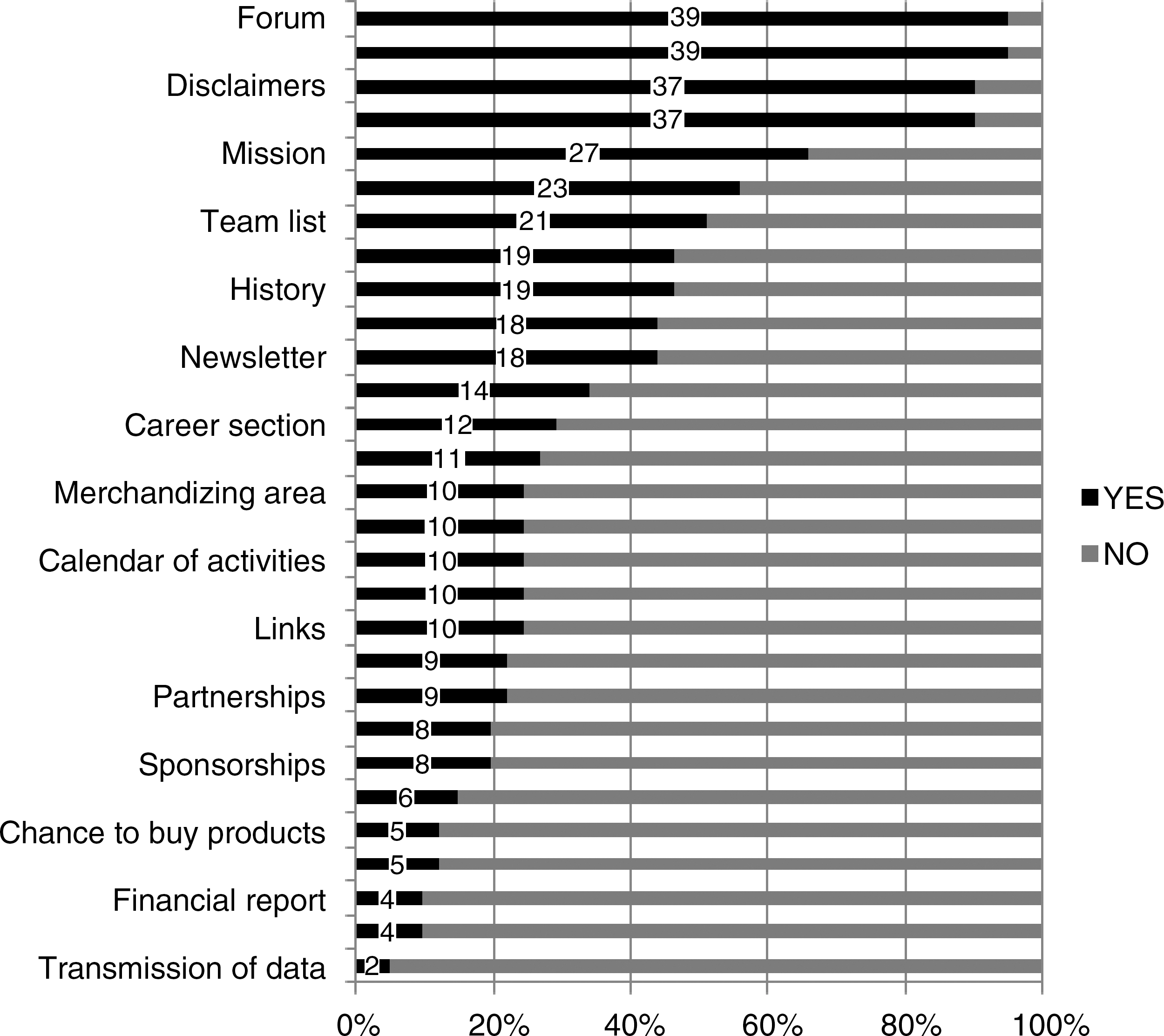
A graphic sketch of the characteristics and general contents present of the Web sites, in order of frequency. The absolute numbers of the Web sites where the characteristics are present are indicated, over the total number of 41 Web sites (100%).
Web Site Contents Related to the Online Community
As regard patient communities, a registered user counter was available on nine Web sites (22.0%), a list of registered users on all of them, and a tool for searching them on almost half of the sample. The search options were by gender (13), age (12), username (11), area (9), disease (8), name (6), and symptoms (4), such as the most frequent search keys.
Twenty-three Web sites (56.1%) were dedicated to several diseases (plurithematic) and the remaining 18 focused on one subject only (monothematic). Nineteen of the 23 plurithematic Web sites (82.6%) provided an A-to-Z list of diseases and medical conditions, and even the chance to create a new group. The groups found most often concerned neurological diseases (16 Web sites), cancer and pregnancy (both 14), and allergies (13). The 18 monothematic social networks in the sample focused most frequently on diabetes (5), cancer (3), breast cancer (2), and mental health (2); the others concerned disability, herpes, rare diseases, obesity, psoriasis, and patients' opinions on hospitals.
Nineteen Web sites (46.3%) displayed convincing statements attempting to persuade the user to register with the social network and become a member; of these, 18 Web sites gave the opportunity to share illness experiences, and 18 offered advice on disease management.
Twelve Web sites (29.3%) gave users the chance to search or contact doctors; doctor search could be by specialization (nine), name (six), or area (four), and the doctors could be contacted online (eight) or at their e-mail address (one). Two Web sites (4.9%) had an “ask the doctor online” service and one (2.4%) took online bookings. Four Web sites (9.8%) advertised or indicated hospitals or clinics.
Referring to disease, 12 Web sites (29.3%) provided therapeutic information: 9 about drugs, 4 about surgery, 4 about diet, 3 about radiotherapy, and 2 about behavioral treatment. Sixteen Web sites (39.0%) gave general information about drugs, 12 stated the name of the active ingredient, and 11 the commercial name, therapeutic indications, and dosages. Two Web sites (4.9%) had a self-diagnosis section. Eight Web sites (19.5%) gave bibliographic references in support of the information provided.
Two Web sites (4.9%) published aggregate statistical data about the social network patients; both gave information on drug efficacy, and one on drug usage and side effects. One Web site indicated who performed the analysis.
The data given here are represented graphically in Figure 3, in order of frequency.

A graphic sketch of the contents of the Web sites related to the online community present on the Web sites, in order of frequency. The absolute numbers of the Web sites where the characteristics are present are indicated, over the total number of 41 Web sites (100%).
Comparison of Groups of Web Sites
A comparison of Web sites with at least one quality certification and ones with none for the variables listed under Methods section gave no statistically significant result (chi-squared test, null hypothesis p < 0.05). The same result was obtained with monothematic and plurithematic Web sites. Web sites providing therapeutic indications were more likely to have a research area (p = 0.050), and logically drug information (p < 0.000).
Discussion
Our findings reveal the high heterogeneity of health-related social networks, due to the spontaneous nature of the phenomenon and its predisposition to continuous evolution. As a limitation of the study, it has to be highlighted that the Web site selection method does not claim to be exhaustive, although we probably found the most clicked-on Web sites, due the ranking process of search engines, which gives priority to the Web sites with the most hits. Besides, the sample provides a picture of the social networks available at a certain time that is intrinsically variable and could change from day to day. However, a re-appraisal of the sample 10 months later showed that these Web sites are quite stable, as only one was unavailable.
Some of the data raise interesting considerations on hot topics such as the quality of online health information, research perspectives, interactivity and patient empowerment, openness and transparency, privacy, and economic issues.
With regard to quality issues, only 15 Web sites had at least one quality certificate and only 13 the HON Code concerning the quality of health information. This is a matter of considerable concern since the quality of online health information is one of the most worrying and complex issues when it comes to the public health effects of the Internet. Further, it can be seen that the academic world is virtually absent from our sample, since only one Web site declared a partnership with a university, two a sponsorship, and one a link to a university. However, six Web sites enabled users to apply for medical research studies, which means that there should be some kind of contact between the social network and the scientific sector.
The great potential of the scientific sector in terms of research has been highlighted: these platforms can be useful for lower-cost recruitment in studies, and more importantly they allow access to large data sets that are continuously updated by patients. It has been reported that 5% of all amyotrophic lateral sclerosis (ASS) patients in the United States are members of PatientsLikeMe—the largest and best-known health social network 13 —represents the largest existing data set on the disease, although the problem of the reliability of this information is closely linked to the nature of the open source data collecting models. In other words, its potential (the fact that it can be implemented by individuals and continuously updated) is its very limitation (in as much as it is difficult to verify the reliability of self-reported information). In the crowd-intelligence logic, collaborative filtering has been indicated as a crucial mechanism in trust-building in Web 2.0 tools. 8,13
Yet, it is not just a question of data reliability; there is also an issue regarding the usage and interpretation of aggregate data. Indeed, two Web sites in our sample, including the cited PatientsLikeMe, displayed aggregate data on the efficacy and side effects of treatments. This information needs to be handled carefully, as it is descriptive data from an uncontrolled sample; this concept could be taken for granted by health professionals, but it is probably not so obvious to Web site users.
The aggregate data displayed, together with the overall information about treatments and opinions expressed by other users, shows that one effect of these Web sites is undoubtedly a drive toward self-medication. Besides, according to the interactive philosophy of Web 2.0 tools, the majority of social networks had a forum and it was possible to contact the Web site, and one third had links to or mentioned other famous online communities not related to health. Online social networks represent a development of the new concept of health, based on self-empowerment, which broadens the initial focus on illness to include the improvement or resolution of chronic diseases, the prevention of unhealthy states, and the promotion of wellness. 13 In this context it has been suggested that individuals will become “action-taking in a number of areas such as measuring, tracking, experimenting and engaging in interventions, treatments and research,” doing so in collaboration with health peers and in co-care with physicians and other health professionals. This is the revolutionary shift from “intermediation environment” to “apomediation environment” described by Eysenbach, 8 where power and cognitive elaboration are given back to the consumer, and credibility becomes a dynamic process that involves consumers, and is not just in the hands of the experts.
It is not surprising that half of the Web sites that displayed some persuasive statements in favor of registering and becoming a member focused on the concept of sharing the experience of illness, and obtaining helpful advice from other members, in a peer-to-peer approach. An analysis of the contents of posts in PatientsLikeMe has confirmed that members posed questions to others with a shared experience, gave advice and recommendations, and reinforced relationships based on similarity. 14
Web 2.0 is not just participation and interactivity—it is meant to be openness and transparency. However, despite the presumed openness philosophy of Web 2.0 tools, only five Web sites displayed the name of the operator, and often it was quite difficult to determine whether the collaborating organizations were sponsors or partners. It should also be pointed out that pharmacies, which have a commercial interest in patients, were the most frequent in both sponsorships and partnerships. Besides, only half of the Web sites displayed a list of the team running the Web site, and quite surprisingly only three Web sites had patients from the online community on the team.
The theme of openness in Web 2.0 is closely connected to personal data handling. This issue is much more sensitive when it comes to private health data. Almost all the Web sites dedicated sections to terms and conditions of usage, privacy policy, and disclaimers. It is significant that eight Web sites said that they use the data for marketing purposes and two said that they passed on patient data to pharmacies and/or other institutions. The risk of Web 2.0 tools is that when you feed your information into the system you cannot get it out again; for example, on Facebook you can deactivate your profile, but Facebook keeps your data and it can be made public again at any time, if the former user decides. It has been highlighted that Medicine 2.0 applications unfortunately work the same way, and that consumers may be unaware of the persistence of Web information, which is easily perceived as ephemeral but “is often permanently archived and may be accessible long-term.” 8
Besides that these Web sites sell anonymised data to pharmaceutical companies, universities, and research labs, 13 their commercial nature is revealed by the fact that a quarter of them have a merchandizing area, and one-eighth sell health-related products. Another possible commercial role of these Web sites is advertising, by doctors and health facilities, and by the pharmaceutical companies. This could lead to conflicts of interest and fraud, although Swan 13 has suggested that “health social networks could develop into large-scale online aggregated communities with market power, providing visibility into demanded research and remedies and directing and funding research priorities.”
In conclusion, health social networks are likely to become an important entity of influence in the medicine of the future, as they are generated bottom-up rather than top-down, by those who make medicine exist, namely, patients. This is why we “cannot afford to ignore” the opportunities presented by these tools. 15 The great challenge for the public health sector is to make the most of these opportunities, and avoid the tendency of all institutions—including medical ones—to keep things as they are, facing up to the fact that if patients change then medicine has to change as well. More importantly, medicine should encourage a process whereby patients play an increasingly important role in the management of their health, and social networks provide a good means for doing this, specifically in a community perspective. 16
Unfortunately, our findings confirm the criticalities of online health social networks, which have already been expressed in the scientific debate, showing a lack of commitment by the public health sector in this field. Strong involvement is required on the part of the public health sector in this revolutionary and changing era for information, and consequently for health, to minimize risks and enhance the benefits of a process that cannot be halted as long as patients are free to share their experiences on the Web.
Footnotes
Acknowledgments
The authors thank the “Quality and Technology Assessment, Governance and Communication Strategies in Health Systems” Study and Research Centre of University of Brescia (Italy) for their support. Besides, we thank the “e-Health–IADIS Multi Conference on Computer Science and Information Systems” held in Frieburg (D) in July 2010, where these results were presented in an oral communication entitled “Virtual Profile, Real Patient: In the Dynamic World of Online Social Networks Criticalities Stand Still.”
Disclosure Statement
No competing financial interests exist.