
Abstract
Introduction
In 2009, the World Health Organization declared the first pandemic influenza outbreak in 41 years. 1 In April 2009, shortly after this declaration, 46% of Americans were concerned that they or someone in their immediate family might get sick from H1N1 (subtype hemagglutinin 1 neuraminidase 1) influenza A during the next 12 months. 2 It was initially unclear what the public health impact of this pandemic would be and how medical practices should respond. In the United States, the Centers for Disease Control (CDC) press briefings on the H1N1 pandemic chronicled the challenges of dealing with an ongoing and rapidly evolving public health threat. 3 Starting in April 2009, the CDC had regular press briefings on H1N1 and in the ensuing 12-month period to April 2010 the CDC held 61 such briefings. During some weeks of the pandemic the CDC even held daily briefings. Media coverage of the pandemic was equally intense, and a Harvard School of Public Health (HSPH) survey found that 76% of adults were exposed to the intensive public health advertising about the importance of getting the H1N1 flu vaccine. 4 Another poll by the same institution at the end of October 2009, after H1N1 was already rapidly spreading, showed that two-thirds of parents and high-priority adults who wanted an H1N1 vaccination were unable to get it. 5 The lack of vaccine during the H1N1 outbreak provoked the need for prioritization of who should be vaccinated. 6
For primary care practices the combination of an inadequate vaccine supply, an informed and nervous public, rapidly changing CDC recommendations, and the threat of waiting rooms filled with sick and potentially contagious H1N1 patients amounted to a perfect storm. In addition to this was a potential shortage of oseltamivir, one of the approved treatments and prophylactic agents for H1N1. Fortunately, telemedicine offered a solution by using standardized telephonic protocols administered by nurses with computerized decision support to rapidly respond to changes in CDC recommendations. This telephonic and computer-aided solution allowed standardization of advice across a geographically dispersed practice and could help prevent unneeded office visits and spread of disease.
Our aim was to examine symptom calls received by a primary care practice during an acute call volume surge caused by the H1N1 pandemic. We wanted to quantify the effect of telephone triage and telephone treatment protocols on face-to-face medical services. This study demonstrates the potential impact of telephone triage and telephone treatment protocols on an acute surge in patient demand for medical care.
Methods
Setting
Telephonic influenza protocols and nurse-directed telephone triage were the primary telemedicine response to the H1N1 outbreak for primary care patients at Mayo Clinic in Rochester, Minnesota. The telephonic response was coordinated and standardized between three separate divisions, which make up the primary care practice. Primary Care Internal Medicine, Community Pediatrics and Adolescent Medicine, and Family Medicine all participated in designing and editing the telephone protocols. The practice is spread over four separate geographical sites. These practices serve the community of Rochester, Minnesota, as well as employees of Mayo Clinic. The total number of providers in primary care (including physicians, nurse practitioners, and physician assistants) is 138 (62 Family Medicine, 50 Primary Care Internal Medicine, and 26 Community Pediatrics and Adolescent Medicine). Mayo Clinic primary care has 135,500 paneled patients who in 2009 accounted for a total of 330,000 office visits. Over the course of the pandemic, the panel size was relatively stable. There was a net gain of only about 1,400 (1%) patients from the 3rd quarter to the 4th quarter 2009.
Influenza protocols were developed by one of the authors (G.B.) using CDC and Minnesota Department of Health guidelines and assistance from Mayo Clinic specialists in infectious diseases. Three separate telephonic influenza protocols were developed, one each for children, adults, and asymptomatic exposure to influenza. The protocols were then hard-coded into the institutional telephone triage software (ExpertRN) and used by Mayo Clinic primary care nurses to help guide them through symptom assessments. The influenza protocols in the triage software allowed the triage nurses to make expert-guided decisions on who should receive antiviral prescriptions, who should stay home without antivirals, and who should come in for further evaluation. Further details of the expert system triage software used by Mayo Clinic have been described elsewhere. 7
Due to changes in vaccine supply and rapidly changing recommendations on priorities for antiviral treatment and vaccination, the content and logic of the influenza protocols was updated multiple times during the most rapidly evolving stage of the outbreak. The software was used by each of the primary care triage nurses, thus ensuring that the most up-to-date influenza protocol was standardized across all four practice locations. In addition, the software included important medical content regarding how long patients should remain confined to their home for an influenza-like illness and what types of home care was appropriate for their influenza symptoms.
Callers to the practice were transferred to a triage nurse for both symptom assessment and questions about asymptomatic H1N1 exposure so that nurses could use the software to help determine the best disposition for the patient based on a symptom algorithm or treatment protocol. Callers with symptoms fitting all inclusion criteria for H1N1 (fever, headache, myalgias, and cough) were put through the treatment protocol algorithms. The H1N1 treatment algorithms were not trivial. For example, the adult H1N1 treatment algorithm contained 16 separate exclusion criteria for history and 8 other current illness criteria that all recommended face-to-face visits. In addition, there were several other criteria, including decreased levels of renal function, that the decision support branched to appropriately reduced oseltamivir doses.
Data Collection
As with other symptom assessments, triage nurses gave dispositions to each caller categorized by urgency and place to seek care. For example, a caller with flu symptoms and shortness of breath was directed to the nearest emergency department (ED). Other callers who fit all the inclusions for H1N1 influenza and had no exclusions for treatment were given a prescription for oseltamvir via fax to their pharmacy of choice. Dispositions were categorized as recommendation for ambulance, ED evaluation, urgent visit (visit within 4 h), acute appointment (visit from 4 to 24 h), routine visit (visit beyond 24 h), treatment with medication (no face-to-face visit), and home care (no prescription and no further diagnostic tests or office visit). These disposition recommendations were captured by the triage software. After the call we also asked what the caller would have done if the triage service was unavailable. In this way, we were able to estimate the effect of the nurse telephone triage and treatment protocols on healthcare utilization. For example, a caller who was intending to get an appointment for an office visit may have stayed at home based on the nurse recommendation, thus decreasing healthcare utilization. Likewise, a caller who was asymptomatic but may have been exposed to the flu could have intended to schedule an office visit to get a prescription for an antiviral. Instead, the nurse could provide the same service by telephone protocol and decrease further exposure to H1N1 from or to sick patients in the office.
Statistical Analysis
On the basis of the Minnesota Department of Health influenza surveillance 8 and our own call volumes concerning influenza, we defined the months of September, October, and November 2009 as the peak influenza months and the months surrounding that period (July, August, and December 2009, and January 2010) as nonpeak months. Our triage call volume data collection was not in place throughout 2008 so a seasonal control was unavailable. Categorical counts were analyzed by the χ 2-test. Statistical software was JMP 8.01 (SAS Institute, Cary, NC).
This study was approved by the Mayo Clinic's Institutional Review Board.
Results
Symptom call volumes are illustrated graphically in Figure 1. Symptom calls showed a sharp peak in October, which coincided with the peak H1N1 infection rate in Minnesota. 8 The total number of home care recommendations by telephone triage nurses also dramatically rose during the peak month of October. By comparison, office appointments and ED visits for those same months only rose slightly. Mean monthly call volume was 5,596 during the peak of the pandemic from September through November 2009, which was 56% above the mean of 3,595 calls for the nonpeak months of July, August, and December 2009, and January 2010 (p < 0.001). The peak month call volume of 7,593 came in October and was 111% above the nonpeak months (p < 0.001).
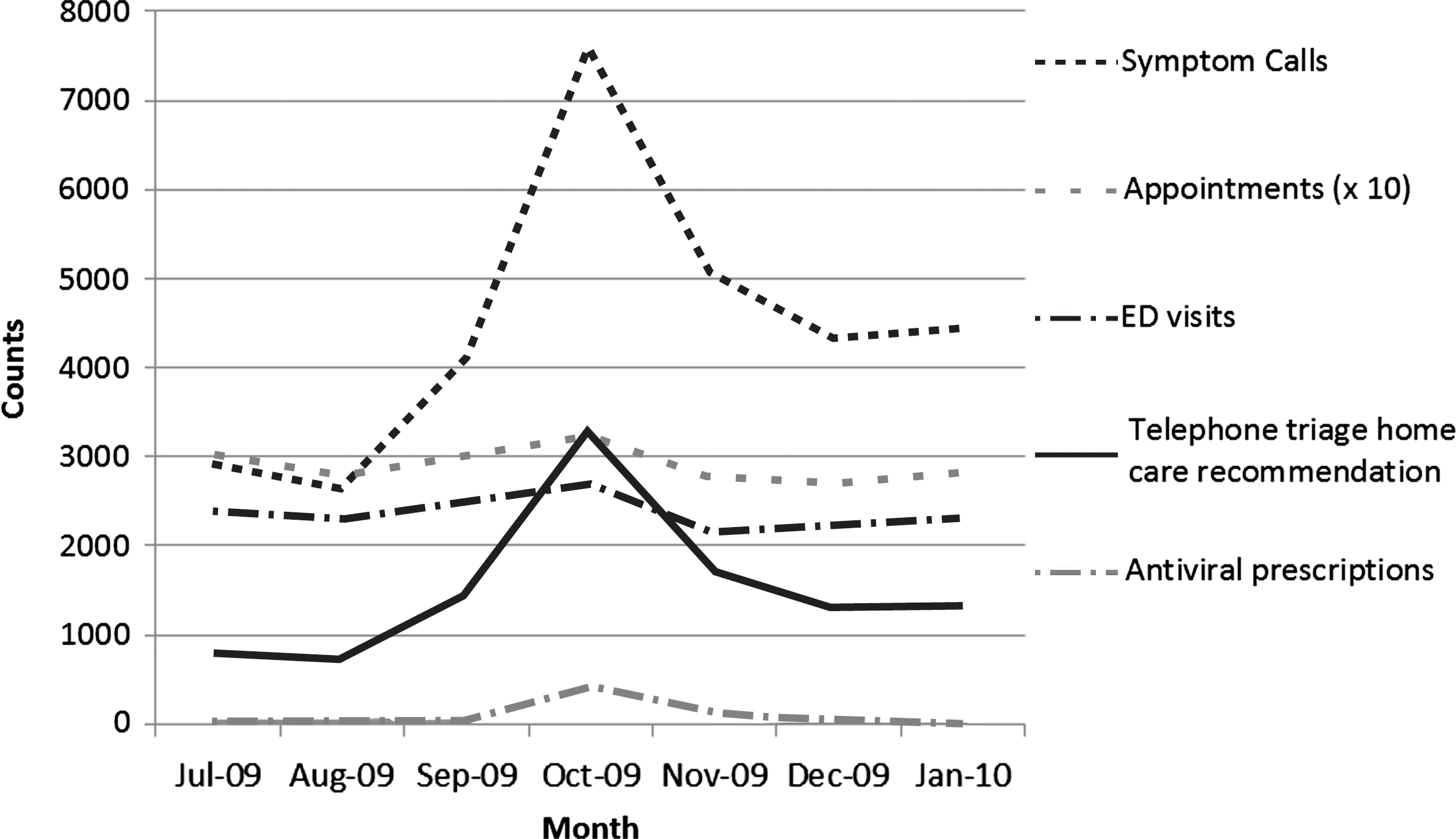
Counts of symptom calls, appointments, emergency department (ED) visits, telephone triage home care recommendations, and telephone antiviral prescriptions before, during, and after H1N1 influenza A pandemic.
Table 1 quantitatively shows the month-by-month surge and decline of calls from August 2009 through January 2010. Appointment demand from calls indicated by callers' preferences reached its peak at 6,071 in October. This represented in a 98% increase from the nonpeak monthly average of 3,066 (p < 0.001). If the October 2009 caller expectations had been satisfied by filling appointments, this would have resulted in using 17% appointment capacity.
Call and Appointment Counts by Month (Percent Increase or Decrease from Previous Month)
In September, October, and November, telephone triage nurses provided 588 prescriptions for antivirals from of a total of 604 prescriptions (97%) extending from August 2009 (zero antiviral prescriptions) through January 2010 (three antiviral prescriptions). Antiviral prescriptions by telephone in October accounted for 5.4% of the symptom calls and 39% of all protocol-generated telephonic prescriptions. With 412 antiviral prescriptions given in October by telephone protocol, 1.1% appointment capacity was preserved.
Triage nurses recommended home treatment (home care or prescription medication) for 2,129 calls per month during peak months compared to 1,017 calls per month for the nonpeak months (p < 0.001). In October, triage nurses suggested 3,250 of the 7,593 (43%) callers stay home; in comparison, 1,522 (20%) callers originally intended to stay at home for their care, before telephone triage. With an appointment capacity of 35,126 visit slots, a potential 5% capacity was preserved for October.
The proportion of calls triaged to antiviral home treatment or home care rose significantly from 28% (confidence intervals [CI] 95%; 27%–29%) during nonpeak months to 38% (CI 95%; 37%–39%) in peak months. For the peak month of October, 43% (CI 95%; 42%–44%) of the calls were triaged to antiviral home treatment or home care.
ED visits for primary care paneled patients went from an average of 2,289 visits per month on the nonpeak months, to 2,432 during peak months. This amounted to only a 6% increase in average ED visits for the peak months of the pandemic.
Discussion
Despite a dramatic increase in the number of symptom calls (Fig. 1) and associated appointment demand (Table 1) during the H1N1 pandemic, we were able to keep our appointment fill rates below 100%. Our ED utilization data also suggest that patient demands for access were not being substantially shifted to the ED. To our knowledge, there are no other published studies that quantitatively examine the potential impact of telemedicine on an acute surge in demand for services such as occurred with the 2009 H1N1 pandemic.
Our experience during the H1N1 pandemic highlights how a telephonic response can be used as a way to control healthcare utilization and at the same time provide a useful public health service. During the pandemic there was a major increase in demand for medical services. If the demand for services during the pandemic could not be managed, we were at risk of being overwhelmed by influenza patients while turning away patients who had other urgent medical needs. In that scenario, patient care would be shifted to the ED, causing ED overcrowding as well. Beyond medical services demand, there was an information demand. In the midst of a relative shortage of vaccine, patients were wondering about their risk for disease and whether they fit the priority criteria for vaccination. In addition, there were questions about adverse reactions to the H1N1 vaccine. 9 Patients needed reliable information about such questions and in a well-coordinated and uniform way. As patients became ill with influenza-like symptoms, they wanted to know if they should be treated and with what. From an influenza containment standpoint, having patients with influenza symptoms packed into doctor's offices was something to be avoided. We were able to address these issues by telephonic means, using software to guide nurses' decision making and incorporating CDC recommendations into the logic.
In addition to the direct benefits of a telemedicine response for the increased demand on medical care during the H1N1 epidemic, there are less tangible benefits that may be inferred. For example, we do not know the full impact of keeping potentially contagious H1N1 patients away from susceptible patients in waiting rooms. It is certainly possible that influenza infection was prevented by encouraging contagious patients to stay at home. Early treatment of influenza was another potential benefit from our telephonic response to the pandemic. 10 Our telephone protocol for osteltamivir for those with H1N1 symptoms allowed patients to rapidly initiate treatment and potentially reduce the burden of illness. Having a standardized and up-to-date telephone script about H1N1 across all primary care practices was likewise a benefit, but difficult to quantify. Rapidly shifting CDC recommendations and fluctuating vaccine supplies led to difficulty for physicians to deliver a consistent message to their patients. In fact, at the time of the H1N1 outbreak, 47% of Canadian family physicians thought their knowledge of the H1N1 vaccine was insufficient. 11 Having a uniform telephonic script that was aligned with CDC recommendations and showing a unified message and consistent approach to H1N1 across Mayo Clinic practices and sites may have played a role in keeping down even greater demands on medical access.
There have been some safety concerns about the use of telephone triage in the H1N1 pandemic. 12 We had no adverse events reported as a result of telephone triage for H1N1, but in general, assessing the safety of telephone triage may require much larger numbers than we have in this study. 13
Our results may not be generalized across practices. Although other primary care practices were able to gear up to meet the telemedicine challenges of H1N1, the challenges of internal communication across practice sites are considerable without the clinical decision support infrastructure available in our triage software. 14 Our response to the influenza pandemic was greatly enhanced by decision support software. Changes in CDC recommendations resulted in the need for several modifications to our telephone protocols over the course of the pandemic. Our turnaround time from protocol change to its implementation in software and dissemination across all sites was as short as a few hours. This across-practice standardization of protocols in the shared software meant that uniform information was delivered by all the triage nurses regardless of specialty or geographic location of the practice. Given the rapid changes in vaccine supply and prioritization during the peak of the pandemic, there was often a protocol du jour. Having paper protocols, which changed daily, would have been much more challenging both logistically and from a training perspective.
Our study had limitations. Although we used the intention of the caller as an estimate of what might have happened without telephonic triage availability, we do not know for certain what the individual caller outcomes were. We do know that callers often do not follow the advice given by telephone triage. 15 However, regardless of what the individual caller did, our ability to track appointments showed that the overall appointment fill rates changed much less than expected for the call volumes. We were also unable to do a more robust time series analysis of the data. We only had limited ability to capture counts of our symptom telephone calls until 2008. To adequately perform a time series analysis would take a few years of data to adjust for seasonal trends. 16 However, the extremely large changes in call volumes allowed us to show statistical significance in call and prescription counts without needing a more sensitive technique afforded by a formal time series analysis.
Our study demonstrates that telephone triage systems can assist with managing a surge in demand for medical access. At the peak of the pandemic, telephone triage nurses gave out antiviral prescriptions to over 5% of symptom callers in October and possibly deterred up to 600 appointments just for antivirals. On the basis of caller intent, the October appointment demand could have reached as much as 17% of capacity. Instead, actual appointments only rose by 6% from nonpeak to peak months. At the peak of the pandemic, the call volumes doubled while the calls triaged to stay home (antiviral or home care) went from 28% to 43%. Estimated preserved appointment capacity was 5%.
Telephone management of influenza symptoms proved to be an essential part of managing a large surge in demand with little evidence of overflow to other more expensive sources of care such as the ED. The H1N1 pandemic offered a short-term example of how telemedicine could help manage the demand for care without increasing capacity. Perhaps the H1N1 crisis can serve as an example for how a more chronic crisis in medical access could be managed. An aging population and a lack of primary care physicians are contributing factors to the shortage of primary care access, which already affects 65 million Americans. 17 Telephone triage has been suggested as a part of the solution to the shortage in primary care access. 18 Our study shows how telephone triage and telephonic treatment protocols can lower the demand for primary care access in a self-limited pandemic. However, to meet the year-round conditions of dwindling primary care resources, we need more innovative telemedicine solutions soon. To meet this challenge, further research is needed on the effect of telephone triage, telemonitoring, and e-health on healthcare access.
Footnotes
Disclosure Statement
No competing financial interests exist.