
Abstract
Introduction
Distance learning has become increasingly used as an efficient method of teaching and improving clinical outcomes. 1 –7 The use of various Web-based programs has greatly enhanced learning across disciplines in academic settings throughout the United States, especially in many nursing and medical programs. 8 –11 The implantable cardioverter defibrillator (ICD) is a device that was introduced in the 1980s for prevention of sudden cardiac death. ICDs are capable of detecting and terminating lethal ventricular arrhythmias by pacing or delivering an internal shock to the heart to restore a normal rhythm (Fig. 1). Randomized controlled trials have proved the survival benefit from ICD therapy in certain high-risk populations, and there has been steady growth in the spread of this technology. 12

A single lead implantable ICD (
Remote ICD monitoring is available from Medtronic, St. Jude, Boston Scientific, and Biotronik Inc. This advancement in technology allows for rapid data transfer from an individual's home via an in-home remote ICD unit that is placed over the ICD by the patient. Information from the ICD is then sent via the unit over the telephone to a secure clinical Web site for evaluation by the patient's healthcare provider. This mechanism has been used to closely monitor ICD battery and lead function, evaluate an individual's heart failure status by measuring changes in thoracic lead impedance (an indirect measure of fluid accumulation and heart failure status), and evaluate responses to changes in medications and lifestyle. Evaluation of ICD therapy delivered (whether appropriate or inappropriate) can be performed more rapidly rather than waiting for a patient to present for an in-person appointment.
Since patients who are living with ICDs seek medical attention, including noncardiac care, it becomes important for healthcare providers to have familiarity with how ICDs operate. In the case of medical centers such as ours, cardiology fellows and cardiac electrophysiology nurse practitioners receive training to perform device interrogations (i.e., data retrieval) under supervision from physician faculty members, and this requires a working knowledge of device programmers. There is no universal programmer or home monitoring method for reviewing and extracting information from different brands of ICDs. Each individual ICD vendor uses a unique programmer that is only compatible with their product. For example, the Medtronic programmer (Fig. 2) can only be used to extract information from Medtronic ICDs. Likewise, each ICD vendor uses a different in-home device to extract and send information to their own secured Web site.

Medtronic programmer used to retrieve ICD data. (Permission from Medtronic.)
ICD programmers allow the provider to view or extract telemetry data and change settings for a patient's ICD as directed. Thus, practitioners should not only learn the clinical concepts related to the safe care and management of an individual with an ICD but also become familiar with the programmer screens and able to navigate them to find information.
Knowledge of ICD programming is important to optimize medical care for patients who live with these devices. Given the busy daily schedule of our practitioners, we envisioned creating a Web-based educational e-learning module that could be assessed from home or while in the hospital to provide educational references for a practitioner caring for a person with an ICD.
The objective of this study was to design and evaluate an ICD e-learning module that would allow greater access to learning which could also occur at an individual's convenience outside the fast-paced clinical environment.
Materials and Methods
Development of the ICD E-Learning Module
To meet this goal of creating an ICD e-learning module, we established an interdisciplinary team comprising nursing, medicine, dentistry, public health, and experts in educational technology. The module we created covered the general principles a new student or practitioner would be taught in the clinical setting as part of a cardiac rotation or preceptorship. We categorized the key features related to each ICD programmer into universal chapters and created a mechanism whereby practitioners could view specific concepts related to a given vendor or by topic area. In addition, the screen interfaces for each vendor were presented to allow the practitioner to become familiar with the screen shots that they would encounter in the clinical setting, whereas audio details highlighted where and how to extract, view, reprogram, and download stored information from each of the three ICD vendors used at our center: Medtronic, St. Jude, and Boston Scientific. To highlight teaching points, a series of practical scenarios was presented while the screen and audio guided the practitioner through the necessary steps in locating the information or making changes via the programmer to an individual's ICD. Only experienced, specially trained clinicians or technicians should change device settings in collaboration with attending cardiologists or cardiac electrophysiologists. All information was written in a formal script, which followed a similar format that was then filmed for each vendor. A device capable of simulating multiple scenarios encountered in the clinical setting was employed (since it would not be feasible to have actual patients with ICD participate given the limited information per patient and the length of time involved in doing an actual live filming). Thus, having the programmer wand over the device that was pre-programmed with the various scenarios for presentation was more practical and uniform than having a series of actual patients with ICD participate in the “live filming” session.
Sessions of actual screen shots from three of the major vendors were filmed over the course of 2 days of filming using simulated clinical scenarios (i.e., common arrhythmias stored in the ICD that would need to be reviewed and downloaded for interpretation were used). The “live screens” that showed the actual screen shots a practitioner would look for in each device were presented in the filming to highlight where to find critical information and adjust settings under supervision. By viewing the actual screen shot, it was hoped that this would facilitate learning and improve the user's ability to locate necessary information in the future, by visually becoming familiar with the various tabs, colors, and drop-down menus encountered with each ICD programmer. Figure 3 depicts an example of the Boston Scientific programmer screen that clinicians would be required to interact with when caring for a patient with this type of ICD. The quality of the screen shots and audio was then reviewed and edited for all vendors, and those screen shots that were blurry or audio sound that was of poor quality were retaped on a separate film day and spliced into the original filmed segment.
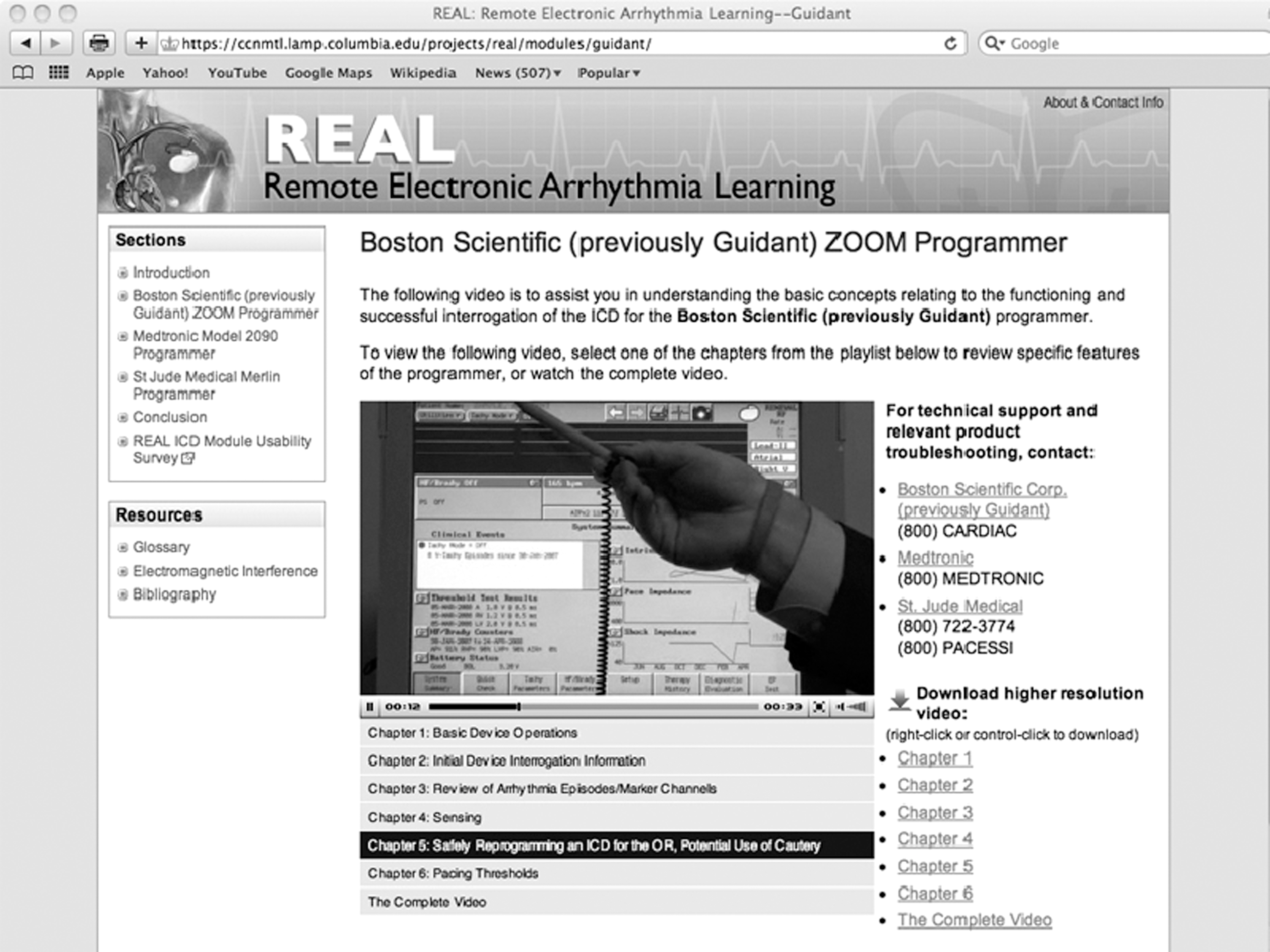
Screen shot demonstrating Boston Scientific ICD information.
Common terminology for all ICDs (i.e., lead impedance, sensitivity, etc.) was presented throughout the live filming and demonstrated for each ICD (utilizing their actual screen shots), and then the terms were summarized in a glossary (Fig. 4). Finally, information was arranged by device type with clear chapter headings where a practitioner could go and visually learn how these measures were obtained on each ICD in detail. Thus, practitioners could become more familiar with programmers from different vendors with which they had little experience. A bibliography with reference links to the landmark studies related to the ICD in the prevention of sudden cardiac death was also created for further reference (Fig. 5).
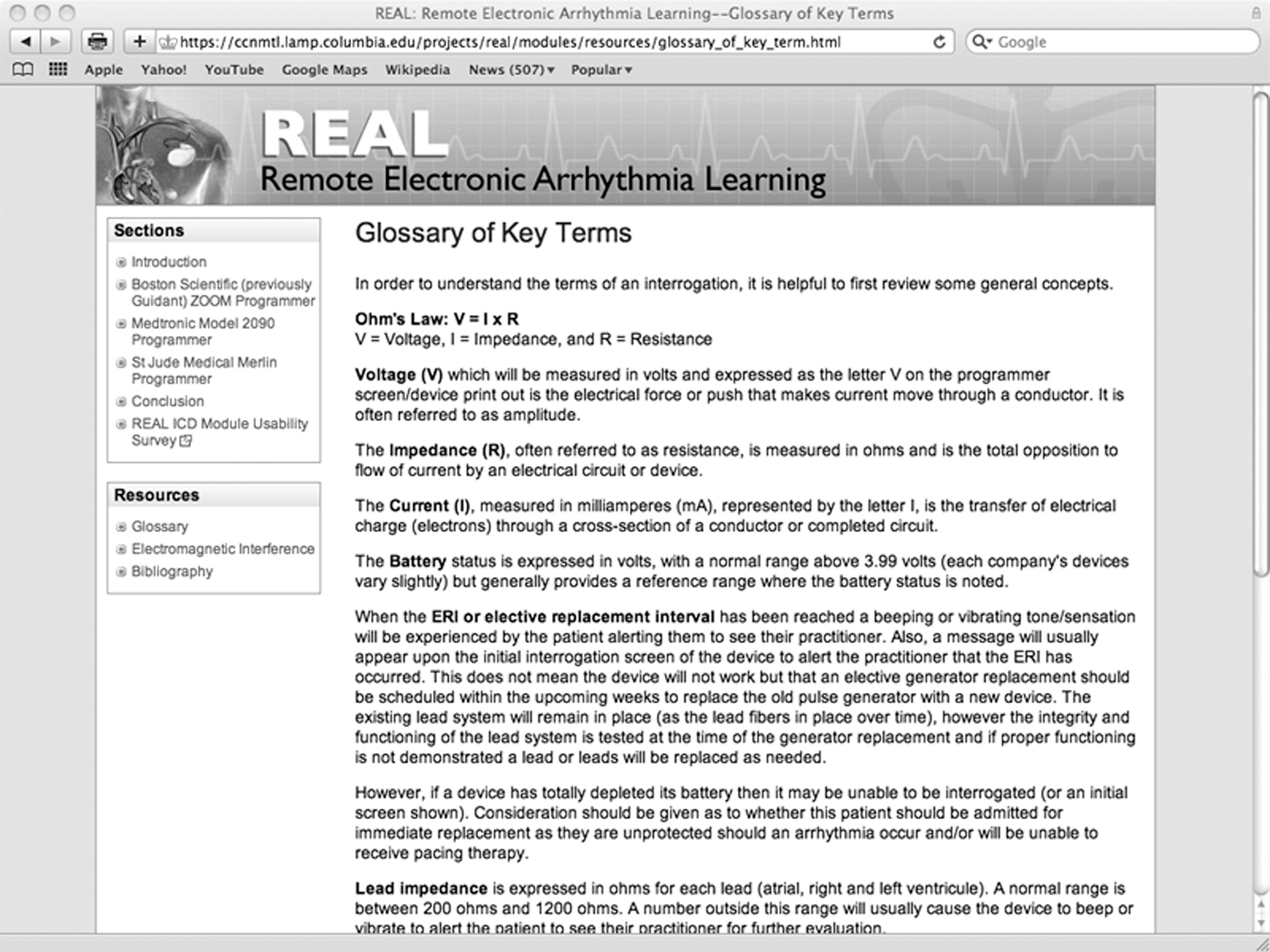
Glossary of key terms related to the ICD.

Bibliography of clinical trials related to ICDs.
The module allowed practitioners to become familiar with common features of each vendor and general terminology and principles related to safely caring for an individual with an ICD. These concepts could be applied to a remote or in-person ICD evaluation.
The e-learning module could be then remotely accessed (from home or in the hospital setting) via the Web by any Columbia University employee with an active and valid login to the general hospital system (Fig. 6).
REAL initial homepage that requires a Columbia University log-in for access.
Evaluation of the Module
After internal review board (IRB) approval, the module content was developed, and a team consisting of two electrophysiologists and two electrophysiology nurse practitioners evaluated the content for clarity and accuracy. Based on their critiques, modifications were made to the initial “script” to be covered during filming and the glossary of key terms that was included in the final product. To determine the usability of the ICD educational module, we asked those who utilized the Web site to complete a brief survey after completing the module. Survey questions were based on the Technology Acceptance Model and addressed perceived ease of use and usefulness of the module. 13
Results
To date, 26 practitioners visited the Web site and completed the survey. The majority (81%) rated the site as a useful resource for ICD learning. A majority (87%) of respondents considered the site as easy to navigate; whereas 77.8% reported the site provided clear practical information regarding how to safely reprogram an ICD for an operating room or outpatient procedure. A total of 86% of practitioners who used the site also reported that the overall basic ICD concepts and terms were presented in a clear and useful manner. Finally, 88% found the actual screen shots associated with each individual ICD very helpful for learning where to locate critical information associated with each ICD programmer. One would anticipate similar results when a module aimed at educating practitioners on the common screen shots and how to extract information via the Web from the three in-home remote ICD systems is developed.
Discussion
Most Web-based teaching material related to the ICD is extremely complex and provides the user with an enormous amount of detail, as it pertains to each individual device and vendor. However, the current Web-based content available from individual vendors lacks context that would provide familiarity with all systems and enable the practitioner to gain a working knowledge of the common functions of all ICD device types. This is largely due to the fact that each vendor provides its own individual training (i.e., via each individual company's Web site) focused on the features of its individual product. Also, each vendor designs its individual screens and location of critical information in a different fashion; thus, one concise format or screen does not exist. In fact, each individual ICD requires that the correct manufacturer's programmer be used for communication and retrieval of information. For example, a Medtronic device cannot be interrogated by a Boston Scientific programmer to acquire information and vice versa. This further complicates the matter in the clinical setting, as programmer incompatibility with a device will not allow for communication. The screens and location of critical information vary considerably between vendors, even though the ICD devices perform the same general functions. The new practitioner is challenged with first locating the information, then interpreting and applying the information to the individual scenario they are managing. The expertise of the team in the design and the layout of this pilot project guided the development of the critical terms to be presented. Creating an ICD e-learning module that included education across vendors presented new challenges. The ideal of an easily accessible, interesting, and stimulating format required an interdisciplinary approach between nursing, medicine, dentistry, and public health to develop a novel technology.
Potential future applications for our e-learning module include helping practitioners become familiar with home monitoring systems that have become available in the past several years. Currently, the major ICD vendors offer in-home remote monitoring systems with the capability of transmitting information from patients' ICDs such as arrhythmia burden and device status. For example, such features allow for detection of time spent in atrial fibrillation for those with a history of this arrhythmia. They also allow for the close monitoring of device leads that may be under an advisory and battery status for an individual who may have no underlying heart rhythm and who is completely dependent on their device. Such close remote monitoring provides a safe and effective mechanism that could serve to help guide treatment and management more efficiently.
In this way, closer follow up can be performed from within a patient's home, eliminating the need for frequent visits to the clinic, unless further evaluation is indicated. 14 In conjunction with sensor technologies available in some ICDs that measure heart rate variability or monitor intravascular volume status through thoracic impedance, these remote systems also provide the ability for enhanced management of chronic diseases such as congestive heart failure. 15 Highly skilled clinicians can download the clinical setting information for further evaluation and changes in the patient's treatment, or in-person adjustments to the ICD can be scheduled to allow for maximal therapeutic benefit. This process requires a clinical expert who is trained to interpret the data and decide on the medical management of the patient. The basic steps of downloading information from the vendors' remote systems can be further clarified in future module additions to remote electronic arrhythmia learning (REAL).
Although the construction of the initial tool required a considerable amount of time (1 year), the relevance and importance expressed across disciplines (nursing, cardiology, medicine, and dentistry) was evident from the inception to the initiation of the project, because of the growing prevalence of ICDs in the cardiac clinic as well as in the general population. Thus, more practitioners will be faced with caring for an individual with a device in the future.
This project was funded by an internal pilot grant and used to design and create a Web site for practitioners at Columbia University with the capability to view the most common actual “REAL” screen interfaces on three of the ICDs used in clinical practice, with simulation of a series of events most likely to be encountered in the clinical setting (i.e., downloading stored electrograms, reprogramming a device for the operating room setting, performance testing of pacing thresholds, and evaluating the battery status of the device). The module focused on providing users with the general and practical concepts and principles related to the care of an individual with an ICD and allowed them to visualize the actual “real-time screen shots” from the three most common vendors (Boston Scientific, Medtronic, and St. Jude), with critical audio details of where to find, extract, and reprogram ICDs when needed.
The study did not compare the ICD module with other learning strategies or demonstrate how the module contributed to actual practice. The development and evaluation occurred at a single institution. The generalizability to other large academic settings requires further investigation. Despite these limitations, the findings of this study support the promise of our approach.
The novel use of remote education can help provide critical education and provides a model for other cardiovascular topics in the future. This site will become part of the required basic training for nurse practitioners before a cardiac electrophysiology clinical rotation and for reference before caring for patients with an ICD. REAL is an example of a cardiac e-learning module developed and successfully utilized in the clinical setting to enhance learning.
Footnotes
Acknowledgments
The authors would like to especially thank Seonghyun Kim, Adult Nurse Practitioner and Maurita Baumeister, and Cecille Garcia Acute Care Nurse Practitioner (Division of Cardiac Electrophysiology) for pilot testing this site and Nitin Gumaste and the staff of The Center for New Media Teaching and Learning for overseeing the technical aspects and filming of this production. Special thanks also to Boston Scientific, Inc.: Ray Burbige (featured) and Nicole Cotteta; and Medtronic, Inc.: William Poutre (featured) and Robert Curran. This work was supported in part by a grant from The Glenda Garvey Teaching Academy at Columbia University.
Disclosure Statement
No competing financial interests exist.