
Abstract
Introduction
Diabetes is a debilitating chronic disease that afflicts large numbers of people throughout the world. Its incidence is increasing at an alarming rate, especially in the more developed world. 1 For instance, the World Health Organization reported about 171 million people in the world who suffered from diabetes in 2000. Over 33 million of them lived in Europe. The total number of patients with diabetes is projected to exceed 366 million in the year 2030. 2 In Poland, an estimated 2.5 million people suffer from diabetes, which constitutes over 6% of the whole population. The actual rate is likely to be much higher. 3,4 The incidence of prediabetes stages varies depending on the studied region, and it ranges from 7.2% to 26.1%. 5 –7
Diabetes is progressive in nature. In advanced stages, patients require ongoing monitoring and treatment. Because of its chronic nature and the high cost of professional treatment, patients with diabetes should be encouraged to manage their health as best they can to minimize complications and heavy dependence on the healthcare system. Indeed, there is strong evidence from scientific studies that demonstrates the beneficial effects of patient monitoring and education. 8 –12
Telehome care has been proposed as a solution to the challenges of providing effective and affordable care for patients with diabetes. 3,4,13 –19 In telehome care, patients are expected to occupy a prominent role in managing their disease. In effect, they are partners and active participants in their own care and in the medical decision making that affects them. They assume responsibility for monitoring their glucose levels and for transmitting these data to a designated health facility. They are also responsible for self medication as indicated by standardized protocols. Under these conditions, patients are accorded the benefits of managing their own care, including the adoption of healthy life styles to optimize their health status and quality of life. 15,19 –25
This study was aimed at evaluating the clinical and behavioral impact of a telehome monitoring system among patients with diabetes when compared with a conventional monitoring system in a primary care setting. The telehome system was designed to provide ongoing monitoring of glucose levels and other vital information as well as educational materials.
Methodology
Subjects
A total of 100 patients between the ages of 18 and 75 with type 2 diabetes, equally and purposefully divided between insulin and noninsulin requiring, was enrolled in the study. All were adults who had been regular patients of general practitioners in the Lower Silesia Region in Poland during the period between 2007 and 2009. After securing their informed consent, patients were randomly assigned to either experimental or control groups. The only requirement for the experimental group was having a personal computer (PC) at home with Internet access. The experimental group (n = 50) received an in-home wireless glucose monitor and transmitter, whereas the control group (n = 50) was instructed to follow the usual arrangement they had before the study. Patients with comorbid conditions, including advanced cardiovascular, neurologic, psychiatric, or terminal disease, were excluded from the study. Enrollment was continued until a total of 100 patients, equally divided between insulin requiring and nonrequiring, was secured. The selection process resulted in the following subgroups of experimental and control cases, each consisting of 25 patients:
IA. Insulin-requiring patients in telehome care.
IB. Noninsulin-requiring patients in telehome care.
IIA. Insulin-requiring patients in conventional (standard) care.
IIB. Noninsulin-requiring patients in conventional (standard) care.
Among insulin-requiring patients, 42 persons used insulin mixtures (basal NPH insulin + rapid-acting insulin) and 8 used mealtime insulin (rapid-acting insulin/rapid-acting insulin analog). Thirty-four patients used combination of insulin and oral medications (metformin/sulfonylurea treatment), and 16 used only insulin.
Among noninsulin-requiring patients, 43 were taking oral medications (metformin, sulfonylurea treatment, alpha-glucosidase inhibitors) and followed diet and physical activity regimen; the remaining 7 patients were only on diet regimen and regular exercise.
The Experimental Intervention: Telehome Monitoring
The telehome monitoring system consisted of two modules: a patient unit and a medical (or provider) unit, connected by a computer network (linked to a secure central server). The patient units included a PC with Internet access at home. Each patient in this group was required to download via infrared link (IrDA) his/her data from the blood glucose monitoring device into the PC and to send all results at least once a week via Internet to the doctor's office. The system offered tools for the providers and patients for data collection, data analysis, and decision support as well as software that included clinical protocols for flagging or identifying critical values and appropriate actions that should be followed. The technical configuration of the system is shown in Figure 1.

The technical configuration of the telehome care system.
Nurses provided training on the use of the system, including data entry, during the installation of the equipment and software. Training sessions lasted between 30 and 45 minutes. Additional training was provided for patients who needed more time. Clinical parameters were established for each patient, whereby a range of acceptable glucose values was individually set. Hence, values less than or exceeding that range (from 50 to 280 mg/dL for most patients) would trigger an audio-video alarm at the clinic, and they would also generate a text message to the cellular phone of the caregiver (mostly a general practitioner) to ensure the patient urgent medical attention, which may include titration of insulin dose, oral medications, diet, etc. Patients in the telehome care group had also the option of contacting their physicians by phone, as needed.
Patients in the control group were able to measure their blood glucose levels with the glucometer of their choice, and they were free to contact their physicians by telephone or visit them in their clinics if they thought their glucose values deviated from desired levels. Otherwise, they were scheduled to visit their physicians every 2 months. The total duration of the study was 6 months.
The telehome system software was selected for ease of use or user friendliness (AccuCheck 360°; Roche Diagnostics), and it enabled the doctor and the patient to: Enter the results of blood glucose monitoring, insulin dose, and information about specific events (exercise, food intake, stress, etc.); Get summaries of the transmitted data, including the number of blood glucose measurements during the selected period (e.g., a week, a month), mean blood glucose levels, number of tests above or below prespecified limits, blood glucose results after specific events, and frequency of hypoglycemic/hyperglycemic episodes; and Present trend data in summary form, in charts and graphs that show whether values are increasing or decreasing over time.
Outcome Measures
Several metabolic parameters were evaluated before, after 3 months, and at the end of the study period. Assessment of the effects of telehome diabetes monitoring and treatment was based on the following factors: Regular glucometry (at least 4–5 times a day in group IA and IIA, at least once a day in group IB and IIB, and also whenever the patient was not feeling well) Measurement of glycated hemoglobin (HbA1c) levels before and after the study Blood cell count, erythrocyte sedimentation rate Cholesterol balance, body mass index Creatinine concentration and urine analysis Blood serum electrolytes Blood pressure
Laboratory analysis was performed at a certified laboratory at Wroclaw Medical Center. A glucometer (Accu-Check Active; Roche Diagnostics) and test strips were provided to all patients free of charge during the 6-month study period. The telehome care group also received free infrared transmitters (Smart Pix; Roche Diagnostics) together with the appropriate application software.
All participants in the study were asked to complete a specially designed questionnaire, which included questions about quality of life, doctor–patient communication, and sense of control over the disease (see Appendix). It was administered before and after the treatment. The questionnaire also included specific questions regarding symptoms, hypo- and hyperglycemic event rates (glucose values ↓ 50 mg/dL and ↑ 280 mg/dL, respectively), personal feelings and experiences, and disease and system management. Questions about quality of life provided five-point response categories for the respondents' choice. Adherence with prescribed regimen was evaluated by the GP at the end of the intervention in the following categories: taking medications, insulin injections, diet regimen/physical activity, as well as overall assessment—graded on five levels, with level I meaning >90% adherence; II, 70%–90% adherence; III, 50%–70% adherence; IV, 30%–50% adherence; V, <30% adherence. Following doctor's orders in >70% cases was assessed as a good adherence (I + II level).
Data Analysis
The two groups were compared in terms of their average scores in addition to multiple regression analysis to identify the predictive variables. Significance of differences between means was estimated by t-test or F-test depending on the number of cases and the nature of the measurement involved.
The parameters of the multiple regression model were estimated by means of ridge regression with ridge parameter λ = 0.1. The selection of regression variables was performed using stepwise forward regression. Independence in contingency tables was assessed using χ 2 or exact Fisher test, depending on frequencies in table cells. The segments on the top of bar charts represent 95% confidence intervals. The tests were two sided. All statistical analyses were performed via Statistica v.6.0 software (Statsoft, Inc.) or with VassarStats software (Vassar College).
Results
A total of 95 patients with type 2 diabetes (of the 100 who were recruited into the experiment) completed the study. Three dropped out of the experimental group. One was insulin requiring and left the country after 1 month from the start, and two were noninsulin requiring who lost interest and discontinued submitting the necessary information. Two dropped out of the control. One was insulin requiring who was admitted to the hospital after a car accident, and the other was noninsulin requiring who changed physicians and chose to not continue.
The total number of data transmissions in the telehome group was 1,850, averaging 1.64 transmissions per patient/week. The total number of telemedical interventions (e-mail service, telephone calls, SMS service) during the study period was 474, averaging 0.42 per patient/week. On the other hand, there were 143 medical consultations and 11 home visits in the traditional monitoring group. The point to be made here is the much higher frequency of contacts in the experimental group, which may account for some of the positive findings to be reported here.
A comparison between the composition of the experimental and control groups shows significant similarities in terms of demographic and metabolic parameters, as shown in Table 1.
Comparisons Between the Experimental and Control Groups at Baseline a
Data are means ± SD (%).
Glycemic Control
There was an overall reduction in glycated hemoglobin in both the experimental and control groups. Indeed, the overall difference between the two groups was not statistically significant. However, a significant difference in HbA1c values was observed among noninsulin-requiring patients only (from 6.95% ± 0.82% to 6.66% ± 0.86% in IB vs. 7.21% ± 2.02% to 7.2% ± 1.86% in IIB; p = 0.02), as shown in Figure 2. Compared with the control group, the experimental group reported considerably less hyperglycemic and hypoglycemic events (Table 2). In both groups, men presented significantly larger decline in HbA1c values (0.31 ± 0.92; p = 0.04 vs. 0.07 ± 0.91; p = 0.66). The severity, duration of the disease, and comorbidity had independent effects in both groups. No significant differences in blood glucose concentrations, cholesterol balance, creatinine, body mass index, and blood pressure values were observed between the two groups at the end of the study (Table 2).
Comparisons Between the Experimental and Control Groups in Terms of Metabolic Measures a
Data are means ± SD (%).
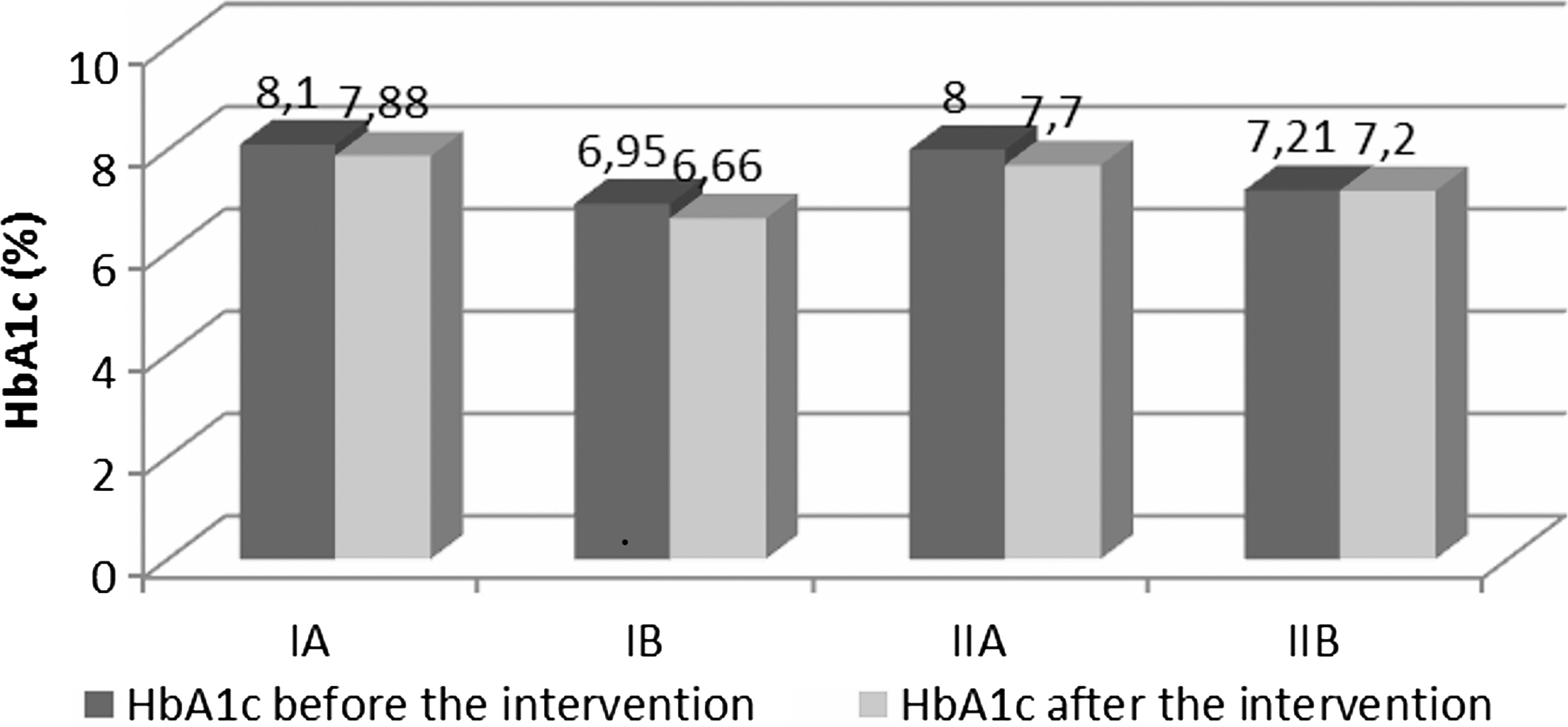
The concentration of HbA1c in study groups before and after the intervention.
Within the experimental group, education and age were positively associated with the decline of glycated hemoglobin (i.e., the more educated and the older patients showed a greater decline), when compared with their counterparts (p = 0.02 and 0.04, respectively). On the other hand, employment status had a negative correlation (i.e., the unemployed had a greater decline than the employed (p = 0.05). In the control group, there was no correlation between age, employment, and the decrease in glycated hemoglobin. Only education correlated negatively with the decline of HbA1c values (p = 0.005), having the opposite effect when compared with the experimental group.
Quality Of Life and Compliance
The telehome group (I) had higher overall scores on quality of life measures (personal interpretation of illness, satisfaction, self-reliance, and feeling of independence) when compared with the control group (see Appendix). However, the differences between the two groups were not statistically significant (overall score was 3.66 in group I vs. 3.41 in group II). The greatest improvement was observed among the insulin-requiring patients who received the experimental treatment (an increase of +0.79 in subgroup IA) when compared with those in the control group (an increase of +0.1 in IIA; p = 0.09), as shown in Figure 3.
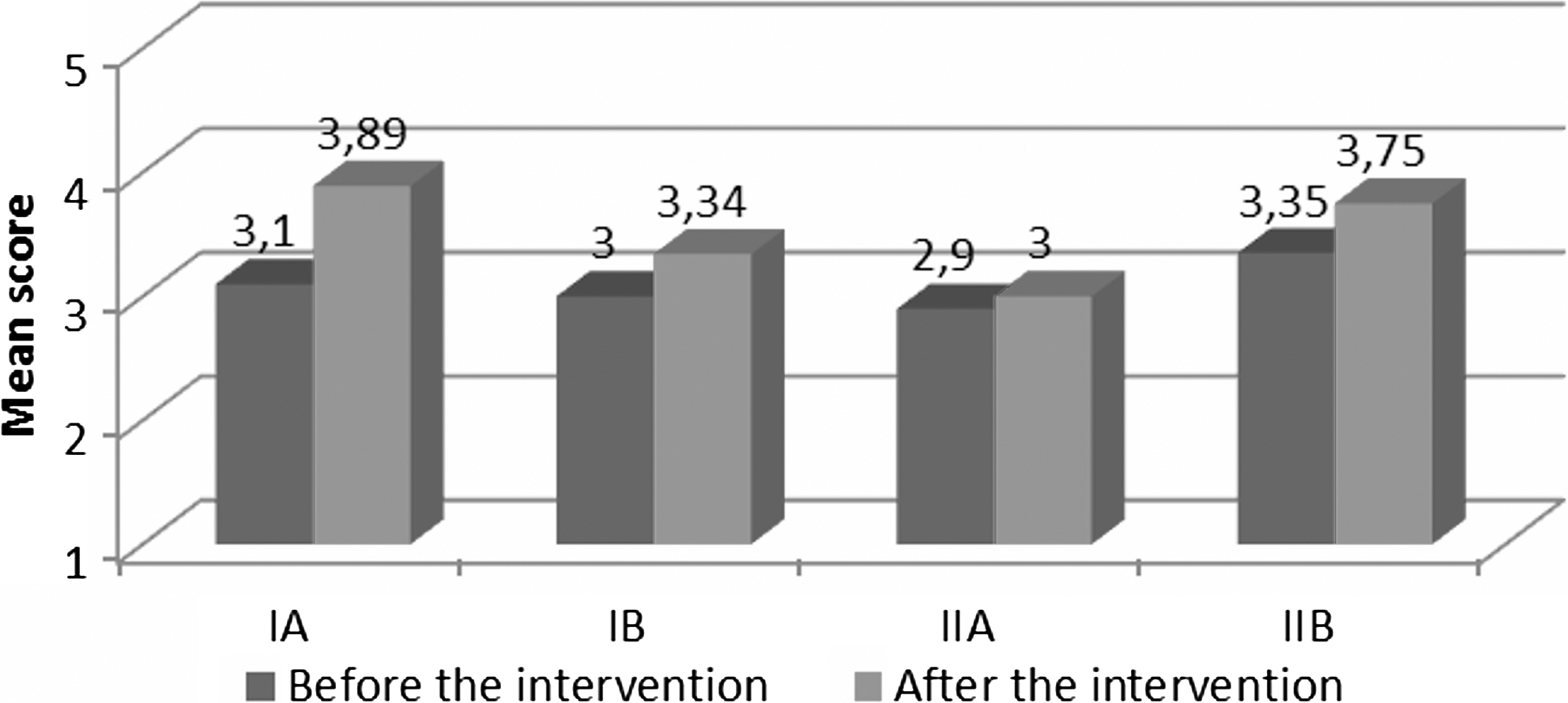
The quality of life in study groups (in 1–5-point scale; 1—very bad, 2—bad, 3—sufficient, 4—good, 5—very good).
The questionnaire included subjective assessments of the patients' perceived ability to control their blood glucose levels, diet, and diabetes in general. The experimental group showed significantly higher scores in terms of their sense of control over glucose levels and diabetes in general at the end of intervention when compared with the control group (p = 0.03 and p = 0.045, respectively), as shown in Figure 4.

Sense of control over diabetes (in 1–5 point scale).
We also included a few questions regarding mental health issues, such as feelings of depression, anxiety, fear, inability to control one's life, and complications related to diabetes. The telehome group reported less episodes of anxiety and depression and better mental health; however, the differences were not statistically significant (Table 3).
Subjective Pyschological Experience of Diabetes
The use of the equipment was not intuitive. Only 35% of patients in the experimental group reported being self-reliant in using the system, 24% required some family support, and 41% were unable to use the system alone and required constant family assistance and supervision. Interestingly, patients who operated the equipment with relative ease derived greater benefits from the system. There was a positive association between educational attainment and ability to use the system without help (p = 0.045). There was also a significant relationship between the quality of life and the intent to continue using the system beyond the termination of the study (p = 0.04).
In both main groups (I and II), adherence to physicians' recommendations was high, but only among noninsulin-requiring patients. In 43% patients (I + II level) in subgroup IB and 44% patients (I + II level) in subgroup IIB, general adherence was assessed as a good one. There was no significant difference between adherence categories in all studied groups; however, adherence in “taking medications” turned out to be the highest one, whereas adherence in “diet/physical activity” was evaluated the lowest one. Adherence among insulin-requiring patients was disappointing and significantly worse in both the experimental and control groups (p < 0.01 in both groups). Data are shown in Table 4.
Adherence to Physicians' Recommendations
Finally, a large majority of patients (74.5%) in the experimental group expressed an interest in continuing the telehome monitoring system. This was higher among noninsulin-requiring patients, 66% versus 83%. It seems that patients who had more reason to be concerned about being monitored were less sanguine about telehome care as compared to their counterparts, even though the majority of both groups favored this intervention. Interestingly, when asked whether they would want telehome care if available, a majority (56%) of patients in the control group said yes. These data are shown in Figure 5.
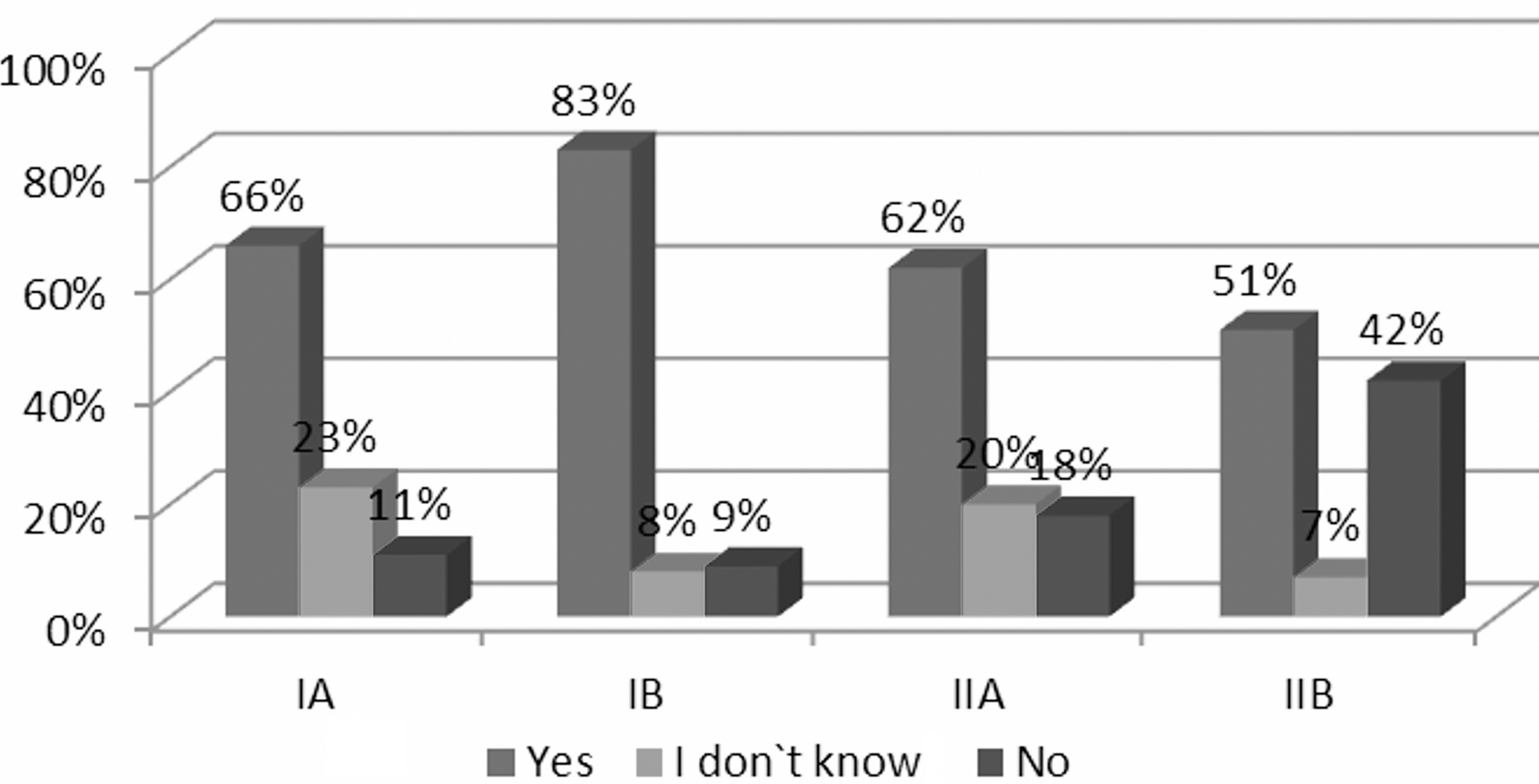
The will of continuation in study groups.
Discussion
The use of telehome care for regular monitoring of blood glucose levels and other diabetes-related information, using standardized clinical protocols, was shown to be a supportive tool in controlling type 2 diabetes in a primary care setting. This is consistent with other telehome research showing a significant decrease in HbA1c, a critical indicator of diabetes management. 14,15,22,26 –31 In the present study, an overall improvement in glycated hemoglobin was observed in both the telemonitoring and conventional groups. Similar results were reported by other researchers. 19,25,32 –34 This suggests the presence of a “Hawthorne effect” in the sense that awareness of participation in the study (together with the requirement of regular visits to the doctor’ s office) had an independent effect on the clinical outcomes measured here. Moreover, the short duration of the study period—6 months—was not sufficient either (1) to overcome the Hawthorne effect or (2) to reveal the lasting effects of telehome monitoring. Nonetheless, a significant decline in HbA1c was observed among noninsulin-requiring patients using telehome monitoring and also the highest levels of adherence with doctors' orders. Thus, this research provides further encouraging evidence regarding the merit of telehome monitoring in managing type 2 diabetes.
Better glycemic control was observed among men, those with higher levels of education, and those familiar with using the Internet and the SMS function of the mobile phone, when compared with their counterparts. 35 Education was positively correlated with the decline in glycated hemoglobin in the telemonitoring group, but it had the opposite effect in the control group. The reason for this difference is not clear.
One way to generalize from these findings is to profile the most effective user in terms of the patient who benefited the most from the telehome care intervention. This profile points to the older and more educated patient who had acquired the disease relatively recently (within the last 3 years) and who spends most of the time at home, likely a pensioner. We choose to refer to this profile as the “super-user.” It may also be worth mentioning who might not benefit from telehome care. It seems to be a younger working person with basic or vocational education who acquired diabetes some time ago. This person is probably not fully aware of the significance of this disease and its sequelae.
Telehome care seems to have a positive effect on patients' mental attitude and their sense of control over the disease. 15,18,19,30,35,36 More generally, there is growing evidence of the positive effects of telemedicine generally on the patient–physician relationship as well as satisfaction with care. 16,17,19,35,37 The tools of telemedicine and telehome care should be seen as necessary adjuncts in the quality of care. The ongoing two-way communication embodied in this study proved to be effective in helping patients achieve a sense of independence.
Some studies have demonstrated that positive motivation to use telehome care had a laudatory effect on the control of blood glucose levels. 35,38 In other words, patients who were most active in measuring and transferring glucose values had better outcomes than their counterparts. In the present study, patients who operated the equipment with relative ease derived greater benefits from the system when compared with their counterparts. This suggests that positive motivation and appropriate education to self-care are critical elements in achieving glycemic control. The observation seems particularly important when considering the effort and costs involved in establishing a telehome care program. A larger investment and much higher frequency of contacts in the experimental group may produce stronger results.
Familiarity with telemedical technology is still somewhat limited in the older generation. However, the situation is changing rapidly with advances in information and communication technology and decrease in price. The Internet and broadband are becoming ubiquitous and fast-becoming within the reach of the average person. For instance, studies in Poland reported that 67% of the Polish adult population used the Internet and 80% of them utilized it for health-related purposes in 2007. 39,40 This is compatible with the general European and world trends. 40 –43 The majority of the participants in this study would be willing to continue using the system if offered.
Conclusions
Telehome care presents a supportive model for monitoring patients with diabetes in their home environment while providing them with educational tools to manage their health. This can reduce visits to doctors' offices, emergency rooms, hospitalization, and length of stay. Although some of these benefits have been reported in the published literature, more definitive research is needed, especially research that relies on randomized clinical trials with large samples.
The findings reported in this article demonstrate the feasibility of telehome monitoring in a primary care setting as well as its potential benefits in patients with type 2 diabetes. The evidence presented here supports the use of this modality for the routine management of diabetes while enhancing patients' quality of life and their sense of independence and control over the disease.
However, telehome care may not be appropriate for all patients. Purpose selection, comprehensive education, and positive motivation are critical elements to its success. It seems that only those patients who were well aware of the significance of their disease and its sequelae and also wanted to participate actively in their treatment and in preventing complications would gain from the system.
Our limited resources did not permit us to apply power analysis to determine minimal sample size to detect actual effects of the intervention. This is especially significant when comparing subgroups within the sample. Hence, the small sample in this study mitigates our ability to declare any definitive finding. Among other factors, this is likely to await the definitive evidence from much larger randomized clinical trials in other settings and environments.
Footnotes
Acknowledgments
Glucometers and infrared transmitters together with appropriate application/software were supplied free of charge by Roche Diagnostics company. The authors express their appreciation to Professor Rashid Bashshur, Director of Telemedicine at the University of Michigan Health System, for reviewing the manuscript and offering suggestions for its improvement. The authors thank GPs/residents and nurses for their help in collecting the data and conducting the educational sessions for patients with diabetes.
Disclosure Statement
There is no conflict of interest for any of the authors. No financial and personal association exists or was provided by the company for this study or any other project with which the researches are associated.
Appendix
Questionnaire for Patients with Diabetes Studies the Quality of Their Lives, a Sense of Control Over the Disease, and the Communication Between Patient and Doctor
| Question | Answer | Score |
|---|---|---|
| Does your diabetes affect the quality of your life? | Diabetes is the biggest problem in my life, which is subordinated to all of my life. | 1 |
| Diabetes is certainly a serious problem for me, limits my daily activities, and forces me to change lifestyle. | 2 | |
| Diabetes is a major hassle for me and limits my daily activities. | 3 | |
| Diabetes is sometimes embarrassing for me. | 4 | |
| Diabetes is not a problem for me. | 5 | |
| Does diabetes raise your anxiety and triggers anxiety reactions? | Yes, always. | 1 |
| Yes, often. | 2 | |
| Yes, from time to time. | 3 | |
| Only exceptionally. | 4 | |
| No, never. | 5 | |
| Do you feel sad or depressed because of diabetes, often you want to cry, and activities of daily live tire and do not give any joy? | Yes, always. | 1 |
| Yes, often. | 2 | |
| Yes, from time to time. | 3 | |
| Only exceptionally. | 4 | |
| No, never. | 5 | |
| Does diabetes reduce your daily activities, such as travel, education, cleaning, shopping, cooking, etc.? | Yes, always. | 1 |
| Yes, often. | 2 | |
| Yes, from time to time. | 3 | |
| Only exceptionally. | 4 | |
| No, never. | 5 | |
| Did you have to give up some pleasures in last 3 months because of diabetes, such as a social event, meeting with friends, go on vacation, sport activities, etc.? | Yes | 1 |
| I don't remember. | 3 | |
| No | 5 | |
| Do you currently have a sense of control over blood sugar levels? | No, not at all. | 1 |
| No, only occasionally. | 2 | |
| Probably yes. | 3 | |
| Yes, in most cases. | 4 | |
| Definitely yes. | 5 | |
| Do you currently have a sense of control over your weight (body mass)? | No, not at all. | 1 |
| No, only occasionally. | 2 | |
| Probably yes. | 3 | |
| Yes, in most cases. | 4 | |
| Definitely yes. | 5 | |
| Do you currently have a sense of control over diabetes in general? | No, not at all. | 1 |
| No, only occasionally. | 2 | |
| Probably yes. | 3 | |
| Yes, in most cases. | 4 | |
| Definitely yes | 5 | |
| Do you currently need to use the assistance of a family or other close persons to establish and follow an appropriate diet? | Yes, always. | 1 |
| Yes, often. | 2 | |
| Yes, from time to time. | 3 | |
| Only exceptionally. | 4 | |
| No, never. | 5 | |
| Do you currently need to use the assistance of a family or other close persons to take prescribed medications? | Yes, always. | 1 |
| Yes, often. | 2 | |
| Yes, from time to time. | 3 | |
| Only exceptionally. | 4 | |
| No, never. | 5 | |
| Do you currently need to use the assistance of a family or other close persons to monitor of blood sugar levels (e.g., daily measurements of blood glucose levels by fingerstick)? | Yes, always. | 1 |
| Yes, often. | 2 | |
| Yes, from time to time. | 3 | |
| Only exceptionally. | 4 | |
| No, never. | 5 | |
| Are you satisfied with contact with your doctor? | I am not satisfied. | 1 |
| Probably not. | 2 | |
| Normally, I am satisfied. | 3 | |
| I am satisfied in most cases. | 4 | |
| Contact with my doctor gives me a great satisfaction. | 5 | |
| How do you describe a bond which unites you with your doctor (in the context of trust, being in contact with your doctor and revealing all frustrated you problems)? | I feel no bond with my doctor. | 1 |
| Weak bond. | 2 | |
| Fairly strong bond. | 3 | |
| Strong bond. | 4 | |
| Very strong bond. | 5 | |
| Do you feel that contact with your doctor, next to the awareness of being taken care of, gives you a sense of freedom and independence? | No | 1 |
| It is hard to say. | 3 | |
| Yes | 5 | |
| How generally do you evaluate your health at the moment? | Very bad | 1 |
| Bad | 2 | |
| Sufficient | 3 | |
| Good | 4 | |
| Very good | 5 |