
Abstract
Introduction
The benefits of face-to-face self-management (SM) education and support programs for individuals with chronic diseases are evident in the literature. 1 –11 Bandura's 12 –14 perceived self-efficacy construct provides the foundation for most SM programs 15 –24 and effectiveness of such programs has been demonstrated in an increasingly broad range of settings. An individualized rheumatoid arthritis (RA) SM program showed positive effects on pain, disability, health status, and quality of life (QOL). 25 Group-based interventions improved communication, personal control, coping, and QOL. 26 Generally, SM interventions for arthritis have been shown to have positive effects on pain, psychological wellbeing, QOL, functioning, 25,27 –32 satisfaction, 7 and utilization. 30,33
The Internet holds promise as a means to efficiently deliver SM programs. Consumer utilization of Internet services for daily applications, however, has far outpaced our understanding of the efficacy and effectiveness of e-health services. Intensive research is needed to understand ways in which clinic-based and e-health services can be complementary or used interchangeably. Although consumers readily seek health-related information from the Internet, 34 their willingness to forgo face-to-face services in favor of e-health services remains unclear.
E-health interventions can enhance social support and improve QOL. 35 Technology has the potential to expand the reach of health programs to new and broader audiences and reduce environmental barriers to healthcare. 36 “Low-tech,” telephone-based, counseling has been shown to decrease depressive symptoms and improve social participation 26,37,38 and treatment adherence. 39 “Virtual groups” or “online communities” can be used to connect people with similar health-related concerns and improve QOL, social connectedness, and health outcomes. 40,41
Enhancement and integration of health information using health information technology (HIT) offers avenues to improve quality and responsiveness of clinical care. Healthcare systems using HIT enhancements have received higher patient satisfaction ratings and treatment adherence. 42 –44 RA clinics have shown efficient patient–professional information transfer using online patient self-reports. 45 –47 The American College of Physicians' Medical Home Monograph describes physicians using HIT to offer seamless, coordinated, patient-centered care 48 and Wagner's Chronic Care Model provides a framework for future collaborative care system. 49
This article describes the design and development of an interactive online environment for use in populations with chronic illness. Using this site, we delivered a validated and empirically based, individualized SM program for RA (a chronic disease with an unpredictable disease course, pain, and disability) based on Wagner's Chronic Care Model. 49 The program simulates clinic-based services, augmenting them with regular clinician contact and a virtual community for ongoing peer support/modeling. The development and usage of this delivery method is examined in the context of a randomized, prospective trial for the efficacy of the program and its features.
Materials and Methods
Online SM Application Overview
An online SM (OSM) site and support “community” was created for individuals with RA.
50
The site, called
Conceptually, the OSM program has a private component (individualized SM program and leader support) and a group component (online “virtual” community). In addition to online features, members are provided with 1:1 leader support through phone contacts. The pros and cons of leader–member telephone contact versus “higher-tech” options (videoconferencing and video streaming) were carefully considered. Although, undoubtedly, the next generation of OSM users would possess a high level of comfort and familiarity with technology-based communication, telephone contacts were selected for the prototype as they are currently more familiar, have been found equally effective in similar circumstances, 43 and decrease the typing burden, which is particularly important for persons with RA. Further, telephone interactions have been found to closely resemble face-to-face interactions. 25
User Interface, Flow, and Process
Figure 1 shows a flow chart prototype of participants' interaction with RAHelp. Following baseline study questionnaires at the initial login, participants view a welcome statement, introduction to site features, security/privacy precautions, and expectations regarding online etiquette and research participation. Confidentiality of members is maintained by requesting participants to not share personally identifying information.
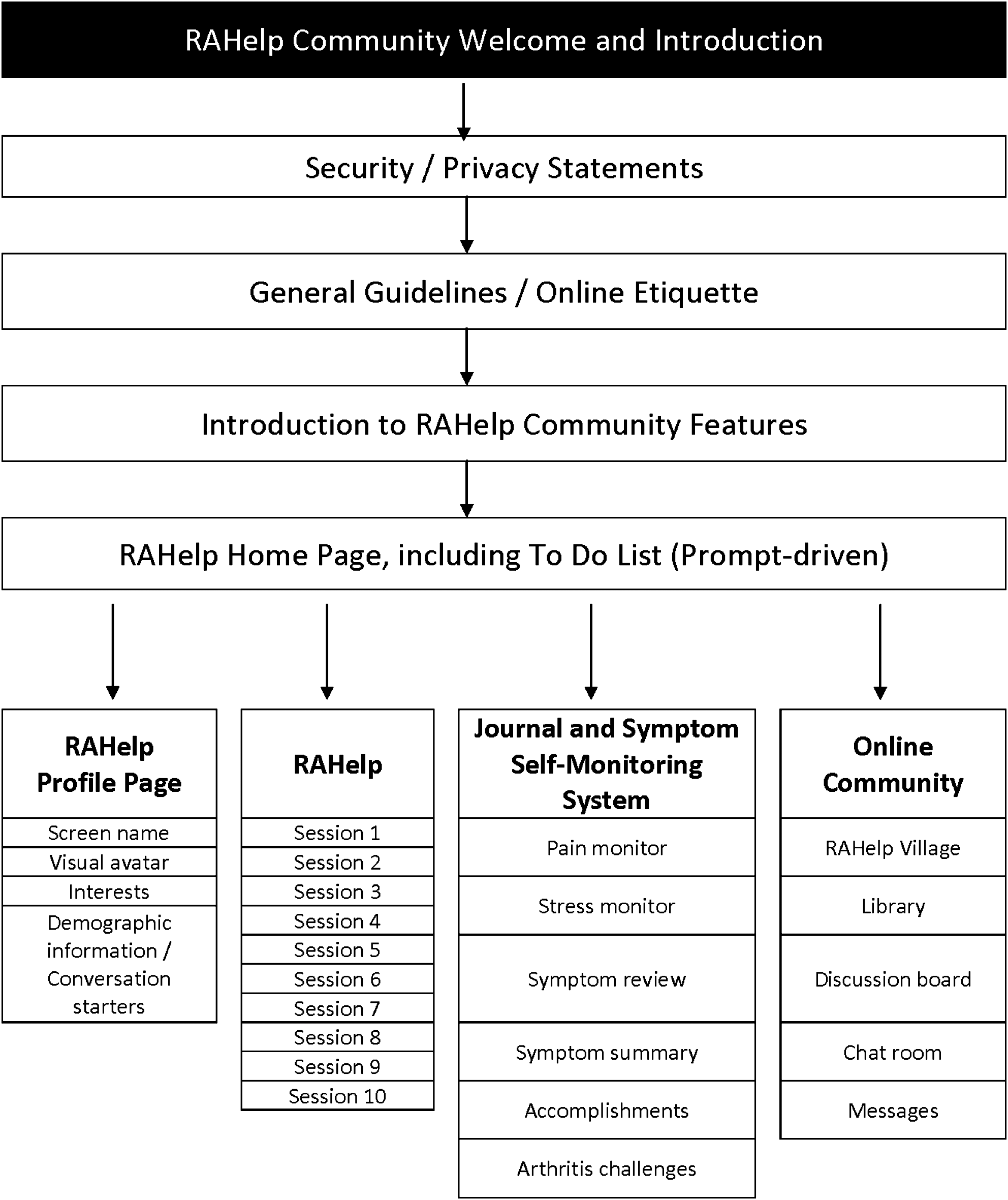
RAHelp prototype flow chart.
Subsequent logins take members to the RAHelp homepage, which contains icons for individualized and community component applications. Icons for general tools such as “Help,” “Settings” (personal display preferences), and “Centers” (information regarding researchers and project staff) also are provided.
After each login, members are instructed to access the “To Do List,” which prompts users with a personalized display of tasks and appointments. The To Do List guides users through a logical sequence for learning about application features and accessing the SM sessions. For example, following introductory procedures, first-time users are instructed to complete their community accessible profile page. Subsequently, the To Do List prompts users to complete the next SM session. When online assessments are assigned (i.e., after SM session), only the assessment questionnaires are available until they are completed. Members may choose to login at times between sessions and access areas of their choice.
Program Features
Member/leader interactions
The OSM intervention at
Members are prompted to complete SM skill-building learning modules presented through PowerPoint visuals and companion text. Also, leaders use an interactive administrative interface to monitor members' site activity and manage access to the SM modules. Members interact with the leader via an online text box, which is viewable using the leader interface, and via weekly follow-up phone calls. The goals of leader–member contacts are to address members' questions, accommodate individual learning styles, and facilitate the integration of new concepts with previously learned material.
Weekly homework assignments involve journaling and using features for pain and stress levels. These features document homework and are available to leaders, permitting them to review and remain updated on member-specific information to tailor weekly phone contacts. Leaders and members review summarized data over time, to discuss and facilitate members gaining insight into relationships between pain and stress and SM.
Virtual community interactions
Community-building features of the program are integrated into the learning modules and homework involves activities using these features. Weekly leader phone contacts frequently encourage community engagement as a means for skill building and developing positive coping. Per Preece, 51 participants are encouraged to enter optional profile information (i.e., gender, age, disease duration, state of residence, favorite color, pets, and hobbies/interests) that is made accessible to all community members. This information serves as a platform for members to initiate conversation and work toward building a strong sense of community, based on common points of interest.
Community members are encouraged to view themselves as “experts” in the daily management of their illness, and dynamic interactions, using synchronous and asynchronous communication modalities, are encouraged by the leaders. For example, members can search the “Discussion Board” archives for coping strategies targeting specific problems. The “Messaging” system allows for private communications among individual members, similar to conventional e-mail systems. There is also a “Chat” feature, which allows interactive communication similar to Instant Messaging. Full transcripts of the previous 20 chat communications are made available for review during regularly scheduled and impromptu chats.
Members are able to access shared resources (i.e., relaxation audio files, educational materials, and Web site links) made available through the library. Using a patient-centered approach, 49 leaders scan online community content and update library resources with topics and information that appear relevant to members. The “News” feature offers members current community and health-related updates.
OSM Administrative Interface: Clinical and Research Management
Leaders regularly monitor all individual and community activity and manage program content usage (i.e., members must access learning modules sequentially). Leaders also review member posts and journal entries and track the didactic content viewed by each member. To accomplish these and other tasks, the administrative interface contains the following features and functions:
Randomly generated member access codes and passwords;
Tracking system for all phone contacts;
Calendar to manage and schedule of appointments;
Documentation tools;
Tools to manage and review all SM features;
Tools to update News to maintain dynamic environment.
As clinicians, leaders are sensitive to safety issues and take precautions necessary to minimize risk to members. The leader's protocol outlines the following safety procedures:
Regular monitoring of all communications within the environment to ensure member safety (e.g., suicidal ideation and child/elder abuse) and constructive communication;
Documentation of actions and communications using “notes” features;
Provision of appropriate community referrals in the event “at-risk” content is identified;
Use of local emergency resources, when appropriate, if there is time delay with e-mail/phone messages.
In addition to clinically trained program leaders, administrative support staff can be given limited access to conduct system and program maintenance activities. For example, support personal can be provided with read-only administrative access to post new resource links, add/delete news items, and monitor completion of study questionnaires. For the purpose of research, the OSM application maintains an online database designed to record all member activity, such as sequence of pages viewed, time spent on pages, number of log-ins, number of postings, and e-mails. Data from surveys, questionnaires, and homework assignments are automatically stored.
Application Security Features
The prototype OSM program is fully compliant with the Health Insurance Portability and Accountability Act (HIPAA). No identifiers, as defined by HIPAA, are accessible by the public. Member anonymity is maintained through the use of an avatar (visual image) and a member-selected screen name. Members are explicitly discouraged from using their real name or divulging identifying information as well as encouraged to respect the confidentiality of other members.
Data from the Web site are secure, and access to the model application server is protected by a firewall. The application uses encryption to ensure the confidentiality of client/server transactions as they cross the Internet. The model application automatically logs out users after 30 min of inactivity to prevent unauthorized access. The only exception is the chat feature, which requires a separate log-in and log-off, thereby allowing members to keep the chat window open while engaging in other computer-based activities.
Technology Requirements
The hardware and software needed to access all features of the site are minimal. Members can access the OSM application using any modern computer with a conventional Web browser. The application may be used easily with either a dial-up modem or high-speed Internet access. Macromedia Flash may be used to access audio relaxation exercises or download results in an MP3 format, and Ajax (an application used by Google Maps for seamless interfaces) allows the chat feature to be fully integrated with the application. 4
Subjects and Recruitment
The Health Sciences Institutional Review Board of the University of Missouri approved the conduct of the OSM study at
Results: Usage Patterns and Findings
OSM Program Evaluation
Evaluation process
The OSM program was subject to several stages of planned evaluation. An area of strength of our development process was the heavy emphasis placed on preplanning, that is, defining and capturing the essential elements of the in-person treatment program and translating them to the online environment. System verification was then conducted by the research development team; each feature of the OSM application was tested independently to ensure that the system worked as designed. As much time was spent in the conceptualization phase, subsequent iterations of the beta program were not needed. Refinements were made on an as-needed basis and subject to system verification, to ensure that the functionality of all features was maintained. Pilot testing was undertaken, in which the standard protocol was followed for several weeks by program leaders and mock subjects to assess full system functionality. Feedback was obtained from participants in the pilot trials to identify areas for further system refinement. Following internal evaluations and final refinements of the OSM application, subjects were recruited for the study. Patterns of usage and interaction among the 33 active trial members and one leader are surveyed in this report as a pragmatic evaluation of practice as it happens in the clinical setting.
Online activity
At the time of this analysis, subjects had participated in
For the individual features, members made 9,679 clicks to read the 10 RAHelp learning modules (mean page length = 26; range: 20–37). The library feature was popular with 1,290 clicks of activity; topics were added based on discussion board content. News items were associated with 939 clicks to read or post (by leaders only).
The Chat feature appears to be the least utilized as designed, with many single chat postings occurring. We expect that at least one factor contributing to low participation was members' geographical dispersal across four mainland time zones (Eastern Standard: n = 8, Central Standard: n = 21, Mountain Standard: n = 2, and Pacific Standard: n = 2) and related difficulty with simultaneous availability. Overall, there were 1,235 clicks of activity surrounding a total of 757 “live” chat messages in a total of chat sessions. Because of the limited success of impromptu chats, biweekly scheduled events were initiated to see if this improved opportunities for members to participate in substantive group chat.
Administrative burden
Leaders in the present study were supported by grant funding. They were responsible for regular “clinical” activity that included weekly telephone contacts (10 weeks) during the initial skill-building phase, mailing relaxation tapes or compact discs, and monthly maintenance contacts for 8 months thereafter, for a total of 12 months.
Following participants' completion of each module, the leaders scheduled phone contacts that lasted 30 min, on average. Monthly maintenance follow-up contacts were shorter, averaging 15 min. Given these activities, the estimated minimum time burden associated with RAHelp was 7 h per member. The actual time burden for planned contacts was somewhat higher, however, because of inefficiencies such as rescheduling appointments, missed appointments, and playing “phone tag.”
In addition to planned contacts, leaders and administrative support staff provided responses to member questions regarding OSM application system, such as questions about initial log-in and difficulty/confusion regarding randomly generated password. Phone contacts addressing these questions generally required 5 min each or less. Messages/e-mail was used by many members to request assistance from leaders for problems such as asking arthritis-specific questions and technical difficulties. Qualitative review of the contacts with RAHelp staff suggests that members experienced little difficulty with navigation and usability of features on the site. 52 Overall, the administrative time burden associated with addressing technical or patient-specific problems outside of planned clinical contacts was small.
Leaders continually monitored site content for inappropriate posting. Evaluation revealed no inappropriate personal information being divulged or other inappropriate material posted (e.g., sexually explicit content, inflammatory responses). To date, the security code has not been broken because of safety concerns and there has been no reported unauthorized access to the OSM environment.
Member evaluation
Overall, members have been complementary regarding RAHelp application, educational content, and the support obtained throughout the OSM community. 52
Discussion
RAHelp AS A MODEL FOR CHRONIC ILLNESS SM
RA has been considered a prototypic chronic disease 53 and, as such, a logical basis for the development of models for chronic disease SM. The ability to demonstrate the efficacy and effectiveness of RAHelp represents a significant advancement in chronic illness treatment. As an increasing proportion of the nation becomes “wired,” the potential for reaching geographically broader audiences, those who are unable to travel because of disability and other underserved populations, also increases. Although vulnerable populations such as these may face slower rates of Internet penetration compared with the general population, it remains a viable and potentially preferable alternative for many.
RAHelp, a project of the Missouri Arthritis and Rehabilitation Research and Training Center, funded by the National Institute on Disability and Rehabilitation Research (NIDRR), has been designed to be patient-centered in both content and process. The site offers consumers easy access to scientifically sound programming, a supportive community, and resources. Learning modules are accessible at any time of day, allowing flexibility to accommodate busy lives and minimizing burden on both members and leaders. Additionally, the site contains easy-to-use self-monitoring tools, which can help both consumers and healthcare providers track important health information.
As is typical in SM programs, peers are viewed as “experts” in the RAHelp program. The application provides a number of integrated social exchange features to enable empathic and therapeutic interaction among members of the online community. 51 Our initial evaluation reveals that members are willing to demonstrate support for their peers by offering ideas and perspective in response to concerns such as making medication decisions, undergoing laboratory procedures, balancing fast-paced lifestyles and multiple responsibilities, pregnancy questions, pain management, and behavioral management strategies. 51 Thus, our objective of demonstrating a viable social support model in RAHelp has been met.
Access to RAHelp is restricted and requiring enrollment has had the distinct advantage of being able to screen volunteers for appropriateness prior to joining the community. Close monitoring of the site by arthritis professionals ensures content relevance as well as the ability to respond quickly to concerns as they arise. For instance, library resources identified by active members have been reviewed and added at the request of members, and discussion board postings have prompted links to sites to be identified and added to the library. To date, member-driven enhancements have addressed a wide variety of practical issues including travel concerns, beneficial footwear, the benefits of humor, Medicare questions, and arthritis-friendly handshakes.
The RAHelp model has been well received by participants, with anecdotal comments reflecting ease of use, enjoyment, appreciation of the SM program content and peer support, and the convenience of an online approach. Members have demonstrated willingness to take risks by performing online activities with which they have no previous experience; in fact, several members reported having no prior experience with an online community, online journaling, making discussion board posts, or using chat. Members report that the symptom-monitoring tools are useful in managing their RA and also for initiating discussion with their own healthcare providers. Many have expressed a desire for continued access to the Web site following the conclusion of the research study.
Limitations of the study include a small sample size, which artificially restricts maximal usage patterns and thus limits our ability to predict utilization of specific site features (i.e., chat). Further, the current prototype will certainly be surpassed by the next generation of environments as well as the technological sophistication of future users. Therefore, as users expect clinic-based healthcare to routinely be available via HIT, the next generation of environments will better meet the demands of both healthcare consumers and professionals.
From a clinical standpoint, start-up costs and costs associated with maintaining an online service may deter smaller healthcare organizations from experimenting with this mode of service delivery. We estimate that development costs, which would include professional Web environment design, selecting and posting online survey measures, and system testing, could reach ∼$60,000 and would take ∼1 year to complete. Annual maintenance costs, including Web hosting, back-up services, and technical support, are estimated at $4,000. Additional costs would include compensation for a trained clinician to serve as leader and any research personnel. Even among large healthcare organizations, sustainability of online health-related services will likely be contingent upon the extent to which such services are accepted into the mainstream, expected or demanded by the public, and/or available as a “prepackaged” service product (i.e., an online service vendor, working on an economy of scale, may efficiently develop and maintain an online service product for multiple healthcare providers or organizations). The most telling evidence of acceptance as well as the most likely predictor of sustainability, however, will be the qualification of online services for reimbursement by healthcare plans. Fortunately, several recent advancements bode well for healthcare online. These include the introduction of Level I Current Procedural Terminology codes for billing online evaluation and management services (not yet reimbursed by most payers); an American College of Physicians position paper supporting e-health; 54 announcements by Aetna and Cigna Corporations that they will reimburse physicians for online visits; 55 and the Federal Communications Commission's movement toward providing free wireless broadband in the United States. 56
Future Directions
The described OSM application fits under a larger umbrella of technologically based enhancement of health communication, frequently referred to as “telehealth” or “telemedicine.” The primary objective of incorporating telecommunication technology in chronic illness care, however, is not to change the care provided. Rather, it is to provide more options for service delivery as well as to enhance communication between healthcare providers and consumers and to connect consumers more efficiently with existing resources.
Despite high expectations and the inevitable growth of telehealth applications in clinical practice, only few works systematically evaluating the various technological advances and their impact on care or health outcomes have been published. 57,58 Further, major clinical and health policy issues remain unresolved or in question. In addition to reimbursement issues, examples include (1) identifying chronic health conditions best suited to online care delivery methods, (2) credentialing of clinicians across state lines, (3) examining the effect of technological advances on access to healthcare and health disparities, (4) evaluating whether telehealth approaches may effectively replace at least some aspects of clinic-based healthcare delivery, and (5) examining the effects of telemedicine on consumer–provider relationships and health outcomes.
Future applications of the RAHelp model will be useful in addressing both clinical and process questions. Short-term objectives should include adapting the model for management of other chronic conditions to fully test the platform usefulness, accessibility, and generalizability. The system demands flexibility and developers should be receptive and creative in incorporating new technology as it is introduced. Additionally, evaluating provider and consumer perceptions and preferences for using higher levels of technology in healthcare delivery would assist in tailoring such interventions and matching consumers with appropriate intervention modalities.
Footnotes
Acknowledgments
This research was supported by a grant from the NIDRR of the Department of Education (No. H133B031120). Support and facilities were also provided by the Harry S. Truman Memorial Veterans' Hospital. The authors acknowledge the assistance of Donna Billingsley, Kim Holtmeyer, Ran-Young Hong, Johnny Kidd, James Laffey, Katrina Rowland, and Chia-Chi Yang in the development of this article and execution of activities related to the
Disclaimer
The opinions in this publication are those of the grantee and do not necessarily reflect those of the Department of Education or the Department of Veterans' Affairs.
Disclosure Statement
None of the authors have financial conflict or other conflicts of interest that might potentially bias the reporting of these results.