
Abstract
Background
Telepresence programs were developed to provide specialized trauma and emergency care to patients in underserved areas and in prehospital settings. 1 Such programs are most widely used in the care of patients with trauma, with applications also for remote critical care consultations. Telepresence takes advantage of the telemedicine system to allow care providers to be present, from a distance and in real time, during encounters with patients. 2 In the current age of small portable computers, high-speed home and mobile networks, and flawless video and audio transmission over wireless networks, telepresence has endless potential in the case of emergency, trauma, and patients requiring critical care.
In 2006, the University of Arizona (UA) in Tucson established the Southern Arizona Telemedicine and Telepresence (SATT) Program, which provided teleconsultation between its trauma center and several rural hospitals in Southern Arizona. In 2007, UA established a program that linked the Emergency Department (ED) and Tucson Fire Department (TFD) ambulances called Emergency Room (ER)-Link. The hub for SATT and ER-Link is the private, nonprofit University Medical Center (UMC), which is a level I trauma center that sees 67,000 patients a year, including 5,000 patients with trauma. The ER-Link operates over a closed citywide wireless communications infrastructure, providing two-way audio and video communication between the UMC ED and TFD ambulances deployed around the city. SATT relies on a dedicated T1 network that links seven rural hospitals on the teletrauma network.
Using SATT and ER-Link, we have recently integrated a system that applies the principles of telepresence to prehospital and remote hospital airway management, with a focus on tracheal intubation. Although the GlideScope™ videolaryngoscope (Verathon, Bothell, WA) has become part of the anesthesia and emergency medicine armamentarium, its use in remote consultations has not been previously described. We believe that this novel approach adds another dimension to the management of airway in the emergency setting. The goal is to avoid multiple attempts at intubation, which can result in iatrogenic injuries such as airway edema, bleeding, aspiration, and hypoxic brain damage.
Methods
Our innovative SATT and ER-Link system at the UA facilitates tele-intubation, providing continuous two-way prehospital communication. In the ER-Link, we modified the videolaryngoscope most widely used today, the GlideScope by transmitting video signals to the computer via a Wi-Fi module (Fig. 1). The range of the transmitter is 500 ft, allowing us to monitor intubations done away from the ambulance and to transmit the video over our telemedicine network back to the hospital. The Wi-Fi module sends the signal to the ambulance, equipped with a Rosetta-VC (General Devices, Ridgefield, NJ), which then feeds the video over our ER-Link to our ED and to our Rosetta-VC and e-Bridge systems at UMC.
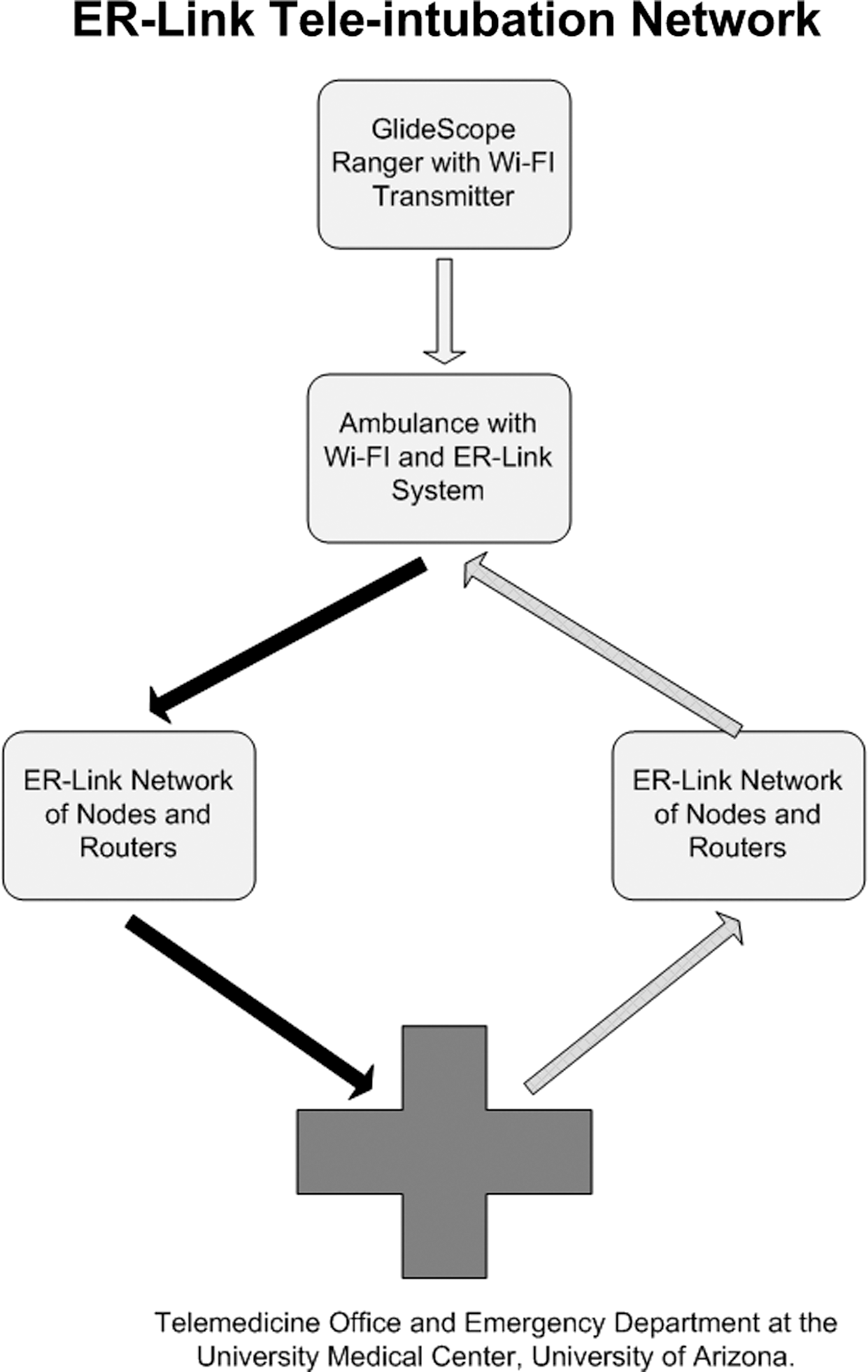
ER-Link tele-intubation network.
For assisting with remote rural hospital tele-intubations, we have attached standard GlideScope units to mobile telemedicine stations that can transmit live feeds from the GlideScope back to UMC. Currently, there are seven sites in rural Arizona on the SATT network, five of which have dedicated GlideScopes for tele-intubations (Figs. 2 and 3). These stations consist of a desktop computer, an overhead pan-tilt-zoom camera, and a T1 Internet connection wired into the UA's existing teletrauma network. We communicate tele-intubations performed with this system to UMC's Telemedicine Office. The physician who needs to perform the intubation can call for remote assistance by clicking on the communication link on the desktop application. The consulting physician on the receiving end can control the overhead camera remotely and toggle between video feeds from overhead and via the GlideScope. As with our ER-Link system, two-way communication is available with very minimal delay and very high quality.
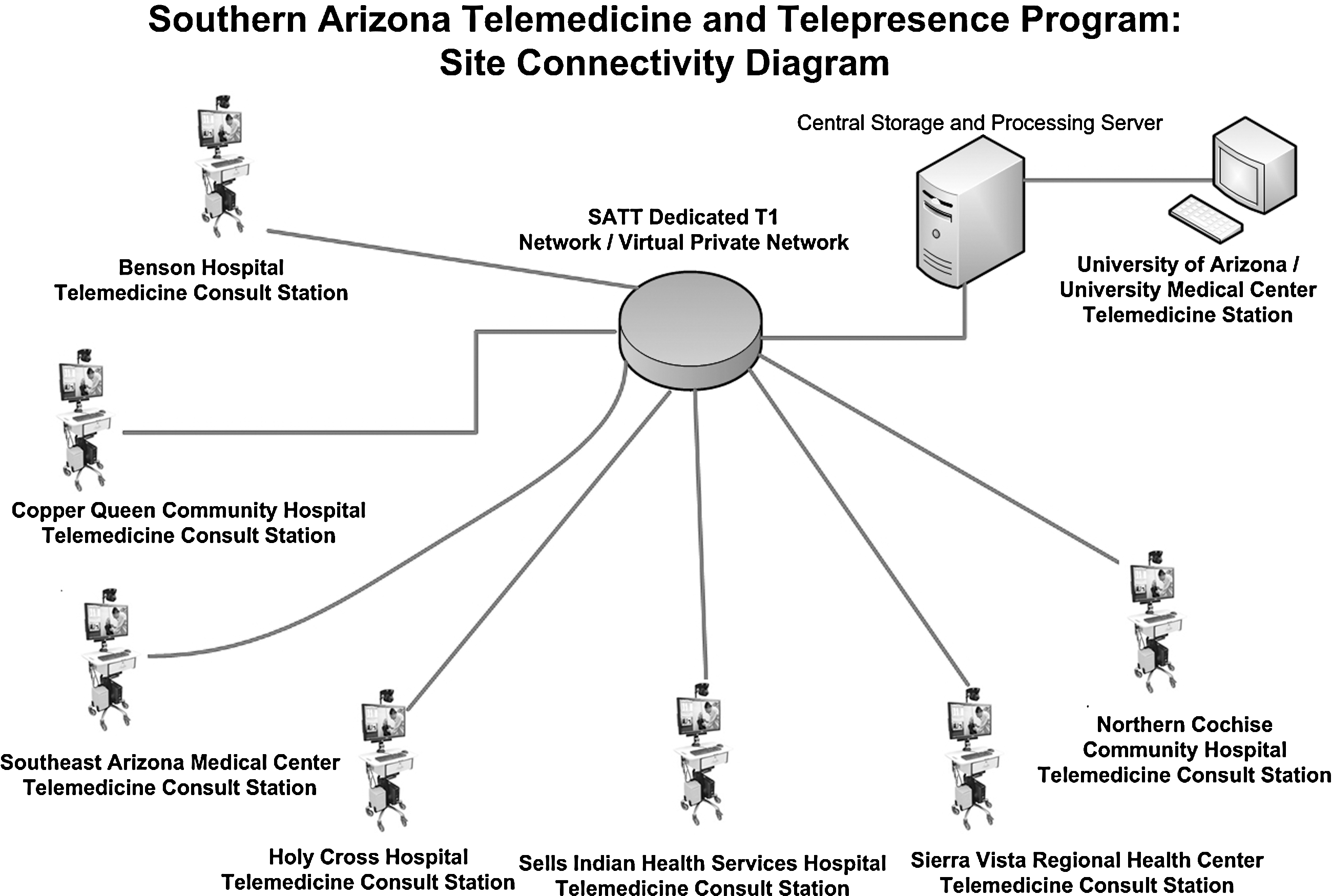
Southern Arizona teletrauma and telepresence connectivity diagram.

Southern Arizona teletrauma and telepresence airway management component.
Case Presentation
A 77-year-old woman presented to the ED of a rural hospital 87 miles outside of Tucson, AZ. She was suffering an acute exacerbation of chronic obstructive pulmonary disease. Due to worsening respiratory failure, at the rural hospital she was started on bilevel positive airway pressure, which only minimally improved her ventilatory status. Her mental status continued to deteriorate and ultimately it was decided that she would require emergent intubation. Her poor baseline oxygen saturations, coupled with some predictors for difficult intubation, made it critically important that she be intubated properly on the first attempt.
The physician on duty at the rural hospital called for the assistance of a physician with expertise in difficult airways (J.C.S.). Through remote assistance using the teletrauma system, the patient was successfully teleintubated on the first attempt using a GlideScope videolaryngoscope. A Cormack-Lehane “Grade I” view of the airway was easily achieved during videolaryngoscopy, and she was quickly intubated without complications. Figure 4 shows a still image captured from the video feed in UMC's Telemedicine Office. She was then flown to a larger facility with intensive care capabilities.

Tele-intubation photo.
Discussion
Prehospital airway management has been the subject of controversy. Although the first rule of any resuscitation is to secure a patient's airway, several large studies have shown an increase in mortality with prehospital intubations. Davis et al., 3 in 2003, found an increase in mortality of 9% and a decrease in “good outcomes” of almost 12%. Dunford et al., 4 also in 2003, reported an increase in hypoxia and bradycardia in patients with traumatic head injuries intubated in the field by paramedics; they noted that most of these patients had satisfactory oxygen saturation before their intubation attempts and that paramedics grossly underreported adverse events.
Cudnik et al., 5 in 2007, studied the effect of rapid sequence intubation and conventional or tracheal intubation on out-of-hospital transport times. They found an average increase in transport time of 10.7 min for patients intubated with rapid sequence intubation and 5.2 min for patients who underwent conventional intubation, as compared with noninvasive airway management. The next year, Cudnik et al. 6 investigated the effect of distance from the hospital and of endotracheal intubation on mortality. They found that intubation during helicopter transports was associated with an increased survival rate; however, for ground transports across all distances, the mortality rate increased for patients who were intubated. The highest mortality rate was seen in patients transported the shortest distances.
Davis et al., 7 in 2006, investigated predictors of intubation success in prehospital intubations by paramedics. They found that both noninvasive and invasive airway management strategies, along with confirmation using continuous end tidal CO2 monitors, improved oxygen saturation and decreased the number of esophageal intubations.
Warner et al., 8 in 2008, investigated the performance by paramedics of airway management in patients with difficult airways. Of 4,091 patients, 96.8% were successfully intubated in four or fewer attempts. Patients requiring more than four attempts comprised the difficult airway cohort. The difficult airway cohort included 130 patients (3.2%) whose airway management consisted of oral intubation after more than four attempts (46%), bag-valve-mask ventilation (33%), cricothyroidotomy (8%), retrograde intubation (5%), and digital intubation (1%). Procedural success rates ranged from 14% (digital intubation) to 91% (cricothyroidotomy). In nine patients (7%), airway management had failed: five of those nine were found in cardiac arrest. The overall mortality rate for patients with a difficult airway was 44%.
In 2009, the Cochrane group reviewed the literature and stated that it does not recommend extending prehospital intubation to patients in cardiac arrest, to patients with trauma, and to patients with pediatrics. 9 The group did, however, state that operator experience may be linked to success and recommended that more research be done.
Before videolaryngoscopy was available, Levitan et al., 10 in 2001, had demonstrated that in trainees in the operating room, simply watching a video recorded from the intubator's perspective improved success rates from 46.7% to 88.1%. Howard-Quijano et al. 11 in 2008, found a drastic improvement in intubation success rates and a decrease in esophageal intubation rates in novice anesthesiology trainees who reviewed a video of intubation.
Chung et al., 12 in 2007, performed remote instruction using wireless communication and constant video feed transmission in a simulation laboratory in two EDs. The intubation success rate increased from 63% in the control group to 94% in the videolaryngoscopy group. Additionally, in 2008, Sibert et al. 13 reported that the use of telepresence to relay videolaryngoscopy and ultrasound images in a mobile telemedicine unit may be possible, in the future, for mentoring intubation trainees.
Given the high number of intubations requiring more than one attempt and the high number of ultimately unsuccessful attempts (because of anterior airways, small mouths, cervical collars, or other difficulties), along with the dangers of extended transport times, videolaryngoscopy may prove to be a benefit. It is a relatively recent and novel approach to airway management. Unlike conventional direct laryngoscopy (which requires aligning the oral, tracheal, and pharyngeal axes to provide a view of the glottic inlet), videolaryngoscopy involves placement of a micro video camera on the undersurface of the laryngoscope blade—allowing the intubator to “look around the corner” and view the laryngeal inlet on a video monitor.
Our system of tele-intubation offers a wide range of possibilities for the future. Recently, we have installed GlideScope videolaryngoscopes at numerous rural hospitals, with the goal of providing assistance for patients with difficult airways. The physicians at such remote hospitals may not be comfortable with airway management. To date, we have tested the system on mannequins in many settings, both in the prehospital environment and in remote hospitals. Previously, Merrell and coworkers, 14 using a low-bandwidth satellite connection between remote sites in Ecuador and Richmond, Virginia, demonstrated successful remote anesthetic monitoring and successful remote management of preoperative patient evaluations, operative plans, video endotracheal intubations, electrocardiography, intraoperative decisions, and patient recovery.
We hope that our novel system of telemedicine and videolaryngoscopy will prove to be an invaluable resource to practitioners responsible for emergency airway management.
Conclusions
Emergency airway management is one of the most fundamental aspects of the care of patients in the prehospital and emergency setting. Unfortunately, many healthcare providers in these settings do not have an opportunity to practice the skill of emergency intubation often and, thus, may not feel comfortable performing the procedure. If they do attempt to perform an emergency intubation and have difficulty, there is usually no one to turn to for assistance due to the environmental limitations. The use of a telemedicine network and a videolaryngoscope has the potential to provide real-time assistance to healthcare providers that do not have the opportunity to intubate frequently. An airway expert not physically present at the site of intubation can effectively view the intubation real-time and provide audio assistance to the operator to help them properly complete the intubation. We believe that this has great potential for improving the success and minimizing the complications of remotely performed intubations. Tele-intubation is a novel concept and technique that has the potential to greatly improve patient care during emergency intubation. Further research is needed in this area.
Footnotes
Disclosure Statement
No competing financial interests exist.