
Abstract
Introduction
Engaging in mentally or socially stimulating activity may protect against dementia, suggesting that both social interaction and intellectual stimulation could play an important part in preserving mental function in the elderly. Conversely, several studies have found that inactive lifestyles are related to a higher risk of dementia. 1 Mental activities, including book/newspaper reading, writing, studying, working, painting, drawing, and doing crossword puzzles and mathematical tasks, form part of the mental training process, which is defined as “teaching theoretically motivated strategies and skills in order to optimize cognition functioning.” 2 Biochemical, physiological, and epidemiological data generated by several studies have demonstrated the effectiveness of cognitive training. 3 –5
Several studies have demonstrated that video games can improve perceptual and motor skills, cognitive function, task switching, working memory, visual short-term memory, and reasoning in the elderly. 6,7 Recent studies have shown better cognitive performance in people who use computer programs to practice mental training for an average of half an hour per day, 5 days per week, for a period of 8–10 weeks. 8
Alzheimer's disease (AD) is the most common form of dementia; it currently accounts for 70% of dementia cases. 9 In many cases, the onset of AD is preceded by a clinical condition called mild cognitive impairment (MCI). This term has been proposed to describe subjects who present moderate but significant cognitive alteration that may worsen within 2 years. Studies show that individuals with MCI are more likely to develop Alzheimer's-related dementia, with the risk of onset ranging from 1% to 25% per year of MCI development 10,11 and rising as high as 80% in the sixth year. In contrast, the risk among previously healthy individuals stands at 1%–2% per year. 12 It, therefore, seems plausible to suggest that halting the development of MCI could have a beneficial influence on the development of AD.
The aim of this article was to design a cognitive training system specifically for the elderly that will be employed primarily in users' homes. A communication channel connects users to a control center, through which medical staff can monitor progress, personalize training, and send messages of encouragement.
Materials and Methods
Proposed Brain-Fitness Model
Applications that use advanced visualization and interaction interfaces to improve cognitive training generally display problems for the user to solve in a very simple manner. In the system used in this study, the right-hand side of the screen shows the user number pad and indicates the action performed (Fig. 1).
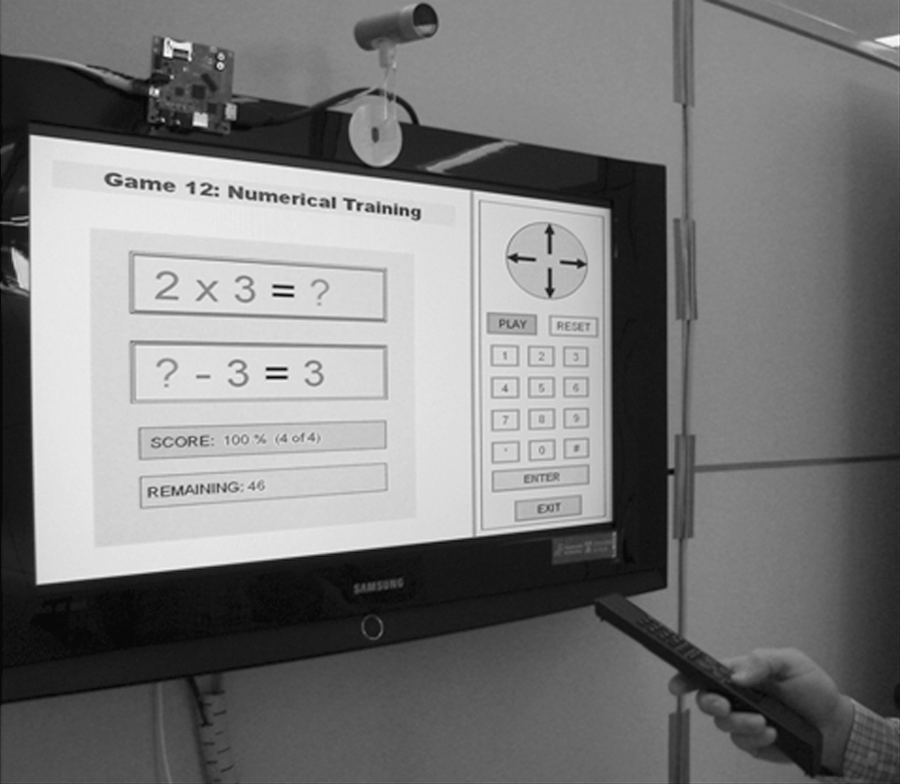
Image of the system in operation.
Applications are grouped into three types of cognitive activities (arithmetic, memory, and association of ideas). Each type of activity offers several games with different levels of difficulty to encourage users to improve on past performance. For example, memory-reinforcing applications have games that involve memorizing letters, numbers, and words (Fig. 2).

Detail of an alphabet rain game.
The system displays the game's basic results (number of right answers, pass or fail) to the user and sends more detailed data to the control center (response time, number of attempts, etc.). In the current version, the system automatically selects a game for the user on start-up, and there is no option to choose another. However, subsequent versions could include the option for users to select games via application menus.
The proposed brain-fitness model based on continuous user assessment needs to take into account the target population's initial cognitive state. The use of this system is aimed primarily at elderly people with no cognitive problems or MCI. Patients suffering from severe cognitive impairment or dementia should be excluded, because they do not benefit from this training.
From a clinical point of view, assessing the user's cognitive state before starting monitoring is essential to assess subsequent development and to determine whether the patient is able to maintain the initial values over time. Objective data about the initial cognitive state are useful in determining whether the subject is benefiting from daily training and in establishing the efficacy of drugs included as part of a clinical trial.
One of the simplest and most widespread tests used in daily clinical practice to assess baseline cognitive state is the Folstein Mini-Mental State Examination (MMSE). 13 Brain fitness is particularly suitable for apathetic or depressed subjects, because mental activity improves depressive mood, and, in elderly people, such depressive symptoms may be indicators of a preclinical phase of AD. 11
Before initiating the training program, and after an MMSE, users received practical instructions on how to use the system. Each subject learned how to log in, interpret messages from control center staff, start a different game, move through the various levels, and receive results, among other tasks.
With regard to game and task types, the system's designers took into account the fact that participation levels may decrease if users consider the training tasks boring or unpleasant, which may, in turn, have a negative effect on results.
Motivation and engagement levels are additional aspects that may influence training outcomes. Tasks that are too difficult or too easy lead to lower levels of motivation and poorer results. Conversely, motivation is higher and learning is more efficient when the tasks proposed are slightly above the subject's current capability. Therefore, staff at the control center should customize tasks according to user performance.
Various applications and games have been created in which users respond to prompts within a certain time limit (parameterizable). These activities are followed by evaluation of the results and user feedback (numerous examples have demonstrated that feedback is necessary for learning 6 ).
The system that we implemented comprised a series of tests, which can be broken down into the following three groups of cognitive activities: 1. Arithmetic (includes tests for sums, equations, and ordering of numbers). 2. Memory (includes tests for visual, verbal, and numerical memory and involves memorizing letters, numbers, and images). 3. Association of ideas (includes tests for word association, image recognition, and word-image association).
Subjects
Verification of the usability and accessibility of the proposed system was carried out using six healthy controls without any previous neurological or psychiatric pathology. The group's age range was 61–72 years, and the average and standard deviation of their ages were 67.83±4.07. None of the controls was taking any pharmacological treatment. All individuals had completed an MMSE and obtained a score equal to or above 30. All subjects also had ordinary mobility and visual capacity. Their technological knowledge was minimal (none of the volunteer owned a PC), but all the subjects owned a television (TV) and used it frequently at home.
Practical Implementation
Figure 3 shows the system implemented. To make it more economical and easier to use, the system adopted the user's TV set as the principal element of the user interface. The system replaces the TV set's standard remote control with a large purpose-designed unit with fewer keys intended to be more manageable for the target user group.

Hardware block diagram.
The system implemented comprised the following components: • • • 1. Audio and video management, with connection to the TV 2. Wi-Fi communications with the control center 3. ZigBee (IEEE 802.11.4) communications with the remote control 4. File system and applications management 5. Brain trainer updating • • •
Results
The reliability of the system was demonstrated with a stress test during 200 h uninterrupted operation. This test was carried out using a loop, through which it interacted with the system proposed by a microprocessor with ZigBee.
The level of accessibility and usability of the proposed system was verified using a survey. Through this survey, the six volunteers included in the study expressed their personal opinions after having used the system for 2 h each day for 3 consecutive days. Users received a 30-min training session before the first day of the trial. The survey consisted of five questions that were scored between 0 (low level) and 5 (highest level).
Discussion
Recent evidence has demonstrated that during cognitive training the brain should be conceived as a dynamic and context-dependent entity, with multiple neural networks operating simultaneously. 17 Cognitive training programs involving repetitive practice of basic cognitive skills, such as memory, reasoning, and speed of processing, have been shown to be effective in improving these skills and, to a lesser extent, in influencing the performance of nontrained tasks. 18
This article presents a simple cognitive training method based on these premises that was implemented in the form of a new brain-fitness system specially adapted for use by the elderly. The aim of this system was to create a daily brain-fitness regime that would be performed under the ongoing supervision of medical specialists. This daily brain-fitness regime could play an important role in delaying the onset of cognitive deterioration or slowing its development, which, in turn, could be highly beneficial to society.
The developed equipment has passed the stress test without incident. During the 200 h of continuous operation, the system did not have to be restarted or restored. The connectivity between different devices was not interrupted during this test.
Volunteers presented an average middle-high knowledge of the use of a TV (Q1=4.17±0.75; Table 1), which is consistent with the fact that TVs are completely integrated in current society. Widespread familiarity with TVs is one of the main reasons why an acceptable level of adaptability was reported by the users (Q2=3.66±0.52). According to these results, users' adaptation to the system was fast.
Accessibility and Usability Test of the Proposed System
ME, mean; SD, standard deviation.
After a trial period, all users concluded that the system was intuitive and clear (Q3=4.02±0.25). Since the visual system (TV) was familiar to the volunteers and all of them adjusted to it easily, the challenge was to provide a visual interface that allows quick and efficient accessibility. This requirement was fulfilled by the minimalist screen, the flexible design, the brain-fitness software, and the dimensions of the TV screen (32” panoramic); these factors allowed each user to accomplish each required action in a short time.
Moderate difficulty brain-fitness games were utilized in this study; consequently, users (MMSE score≥30) reported that the proposed exercises were of moderate difficulty (Q=2.47±0.63). This moderate level might be established as a reference, because a person who is not able to overcome these tests may present signs of cognitive damage. Further, these moderate-difficulty exercises could be used to set a minimum score that individuals should reach when executing brain-fitness applications.
A high motivation level (Q5=3.50±0.84) was reported by the users as a result of both the dynamic nature of the tests and the personal challenge that the exercises offered. The system presented each exercise as a mental game, and this factor was central in achieving such a high degree of motivation. A sample of healthy individuals was used in this study to verify the proper functioning of the system. Patients with MCI were excluded, because it would have been difficult to determine whether negative results were the result of the patient's cognitive condition or of poor system usability and accessibility.
Results about the adaptability (Q2) and content system (Q3) are similar than others systems that utilize the TV as a central element, interacting with seniors or elderly people. For example, the EASYLINE PLUS 19 project is a research that involves 9 elderly users where they value the usefulness with a score of 3.58 and the interface design with a score of 3.38. This allowed us to demonstrate the consistence of our study.
Conclusions
This article describes a system for implementing a cognitive training program in users' homes that was developed to be a low-cost tool with a high degree of user interactivity.
It should be noted that the results obtained in this preliminary study should be confirmed through further extensive studies. This further research should include cognitively impaired patients, as this is the group that this system addresses.
Footnotes
Acknowledgments
This research was funded by the University of Alcalá.
Disclosure Statement
No competing financial interests exist.