
Abstract
Introduction
Hungary has been a member of the European Union since 2004; however, its health system remains burdened by what it inherited from the pre-1989 regime. In the socialist period, the Hungarian healthcare system was run and financed by the state. Market forces were almost completely absent. Healthcare was characterized by excess capacities, decreasing service quality, growing inequalities in terms of access, and an increasingly widespread use of informal payments. 1 After 1990, various reform measures were introduced, and private service providers also appeared; however, the healthcare system remains predominantly state owned and state organized. It is financed by an insurance scheme, which is “principally a comprehensive, compulsory, employment-based national health insurance scheme that provides near universal coverage both in terms of treatment and in terms of population, with nearly all citizens receiving care whether or not they contribute.” 2 The overwhelming majority of hospitals are owned by the state or by municipalities. 3 Most health services are provided free of charge, but copayment is charged for several services deemed “extra.” Healthcare expenditures as a fraction of the gross domestic product have contracted in recent years from the peak of 8.3% in 2003 to 7.4% in 2007.
The level of health services and infrastructure differs widely among Hungarian hospitals and even between departments in the same hospital because of their uneven access to funds. By international comparison, Hungary's healthcare spending is one of the lowest in the Organization of Economic Cooperation and Development (OECD), but high compared with East Central European OECD members (Czech Republic, Hungary, Poland, and Slovakia). Private (financed by the individual) spending on health represents almost one fourth of the total, which is one of the highest in the OECD. Pharmaceutical spending in total healthcare spending is the highest in the OECD. The number of practicing physicians and nurses per 1,000 inhabitants is 2.8 and 6.1, respectively, which is among the lowest in the OECD. 4 These numbers are indicative of the numerous problems the Hungarian health system must cope with. Further growth in demand is backed by the fact that in the OECD comparison the utilization of the system is among the highest, yet the health indicators for the Hungarian population are among the worst. Telemedicine and related e-health services, although not a panacea, could play an important role in alleviating certain problems in Hungarian healthcare.
This study explores the present state and characteristics of telemedicine and related e-health services in Hungary as well as the main obstacles to their further development. The hypothesis was that limited financial resources, which are the main contributory factor to the low quality of information technology (IT) infrastructure, act as the main obstacle to further developments in telemedicine. Lack of IT skills, acceptance of new technology, and technical problems were also hypothesized as contributory factors.
Materials and Methods
The study relied on two main sources. The present state of Hungarian telemedicine and related e-health services by international comparison was analyzed through the available statistical data. As a second source, semistructured questionnaire-based personal interviews conducted with three employees of a given hospital (nurse or laboratory assistant, doctor, IT specialist) in August 2009 were utilized. Altogether, 90 interviews were conducted in 30 hospitals, which well represent the 140 hospitals in Hungary. Hospitals of various sizes were included from all seven regions of Hungary, representing different levels of development, and interviews were conducted in both “ordinary” and “focal” hospitals. (Priority/specialist or focal hospitals provide high-quality services for patients with serious or specific illnesses [e.g., treatment of malignant tumors and organ transplants]. They participate in regional-level capacity distribution procedures and compete for further contracted capacities across the country. Regional or ordinary hospitals provide general services. They have an important, intermediary role between priority hospitals and general practitioners' practices. For example, these hospitals are obliged to perform tonsillectomies, accommodate births, and operate on hernias or adenoids [source: Hungarian Ministry of Health].)
The questionnaire contained four distinct parts: general data from the hospital, data and opinions about hospital information systems, use of informatics and telemedicine in cure, as well as an open part asking for personal opinions about obstacles, trends in telemedicine, and e-Health both in general and in Hungary. Questionnaires addressing IT specialists, doctors, and nurses differed only partly to deal with the relevant problems of the respondents (see Appendix).
Results
There are various definitions of telemedicine. The concept is used here in a wide sense, as providing healthcare services with the use of IT when the patient and the healthcare worker or two healthcare workers are in different locations. It involves the secure transmission of health data and information in text, voice, picture, or another format, which is needed for prevention, diagnostics, treatment, and follow-up. 5 The e-health activities that are closely related to telemedicine were also analyzed.
Based on scarce data available, it is clear that telemedicine is in its initial stage in Hungary, in comparison with more developed countries. However, compared with other countries in the East Central European region, Hungary's position is significantly better. 6,7
E-health indicators can be used as a kind of indirect measure to determine the relative development of telemedicine. With respect to overall e-health indicators by international comparison, the Euro Health Consumer Index 2009 was used. 8 The index compares 27 European Union member states and six other countries. The second subdiscipline of the index refers to the relative level of development in e-health. Its measure is composed of the indices of electronic patient record penetration, e-transfer of medical data between professionals, laboratory results direct to patient via e-health, online booking of appointments, online access to personal care costs (by insurers), and e-prescriptions. In that index (Fig. 1), Hungary fares well, especially by regional comparison. Its score of 46 out of a total of 75 puts it in 12th–14th place out of 33 countries, together with Estonia and Switzerland. Of the new member states (NMS) of the European Union, this is the best score. (The new member states are Bulgaria, Cyprus, Czech Republic, Estonia, Hungary, Latvia, Lithuania, Malta, Poland, Romania, Slovakia, and Slovenia.) Interestingly enough, of the nonmembers in the region, Croatia and Macedonia have the best results at 54 and 50, respectively, which can be at least partly attributed to the telemedicine initiatives in the South East European region. 9

Euro Health Consumer Index e-health subdiscipline.
A similar scoreboard is compiled on e-health use in the European Union, 10 which consists of three main aggregates: electronic storage of patient data, computer use in consultation, and electronic transfer of patient data. Hungary with its 2.2 points is at 9th place out of 27 member states, and it is second behind Estonia in the NMS (Fig. 2). Although Hungary performs well in electronic storage of data and relatively well in computer use in consultation, it received very low scores in electronic transfer of patient data.
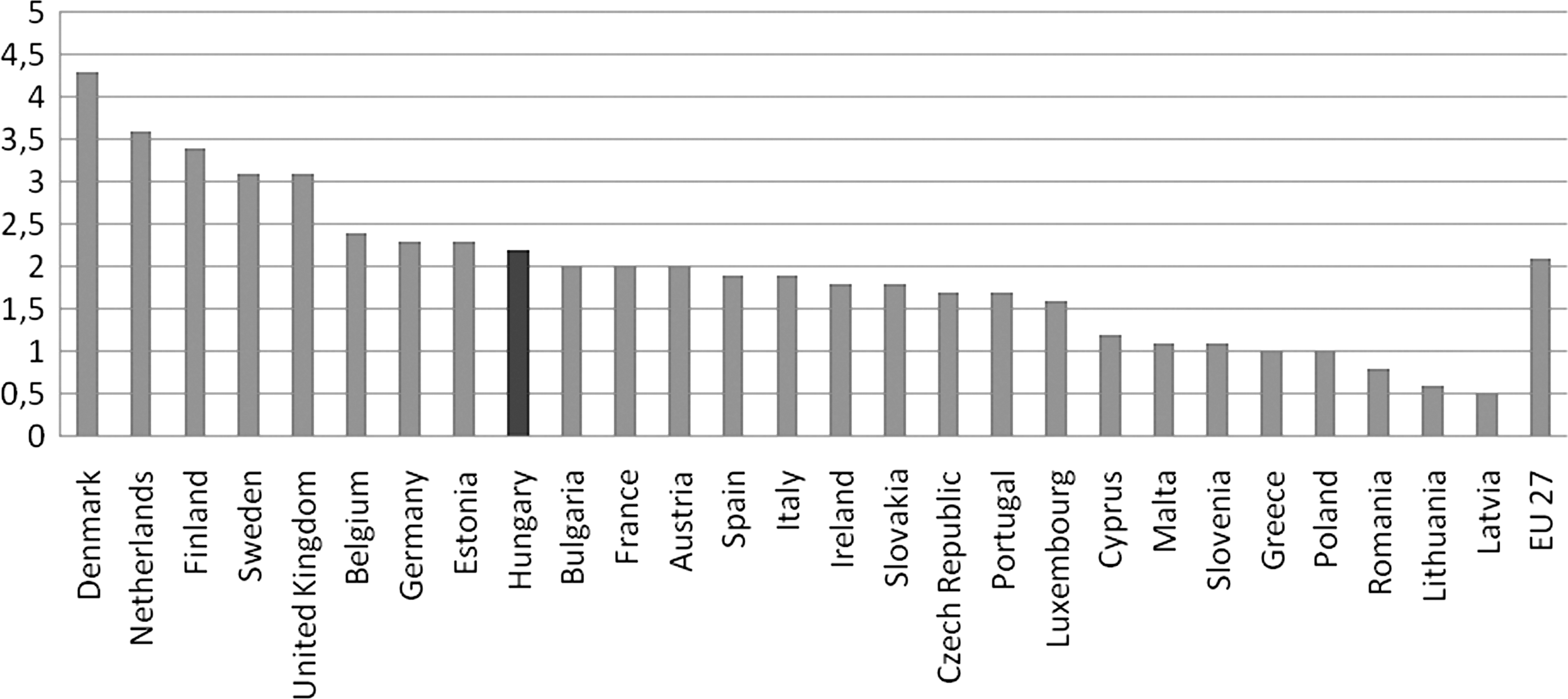
Indicator scoreboard average index score—patterns of e-health use in the EU.
From the point of view of telecare, it is also important to determine how well Hungary fares in digital literacy. According to Eurostat data, although the share of individuals who never used the Internet decreased significantly between 2005 and 2009, this still amounts to 36% of the population. This is worse than the EU-27 average of 30%, but it is slightly better than the average of the NMS (38%). This is certainly a disadvantage from the point of view of the wider use of e-health and telemedicine.
As far as the policy framework is concerned, on the basis of the fact that e-health was an integral component of the EU's i2010 policy framework, Hungary made an effort to improve its system. The main policy document is the National eHealth Strategy, which contains the detailed plan. In line with the European Union's e-Health Action Plan and as in other member states, a policy has been elaborated to expand the health professional portal to include e-prescription applications and other electronic transactions and, ultimately, to merge it with the portal for citizens, providing a solid background for the further development of e-health and telemedicine in Hungary. In the EU, priorities of e-health and telemedicine varied according to the culture and implemented activities of the country. For example, some countries give priority to the electronic health record system and electronic patient records, whereas others give priority to e-health networks, infrastructure, or e-cards. Hungary concentrates its efforts on a national health portal.
Based on the interviews, it was established that telemedicine is still in its initial stage in Hungary. However, the use of telemedicine differs widely in both telemedicine specialist areas and hospitals.
With regard to specialist areas, teleradiology is used most frequently (in almost two thirds of the hospitals where interviews were conducted), partly because of the fact that it can be operated with the existing equipment and instruments and partly because of the acute shortage of specialists. It is also important that radiology is of central importance for many other healthcare processes. Almost all interviewed doctors underlined the fact that skill shortages will become even more acute, especially in radiology, the negative consequences of which can be mitigated by the wider use of teleradiology. The main reason for this is the mobility of radiologists to more developed countries and the low prestige attached to being a radiologist in Hungary. Doctors also suggested that allowing telework for radiologists from home would be helpful, as they spend a great deal of time traveling from one hospital to another. More detailed scrutiny revealed that the use of teleradiology is in an early stage.
As for the other specialist areas of telemedicine and related e-health, laboratory findings are electronically stored and can be transmitted in more than half of the hospitals where interviews were conducted, pathology findings in more than one fourth, and neurology findings in less than one fifth. Telecardiology (e.g., wireless transmission of ECG or monitoring of patients) is used in one fourth; Internet-based consultation is available in one fifth of the hospitals, although predominantly within the hospital. Telemonitoring exists only in a very preliminary phase: in more than half of the hospitals, measuring devices are used by the patients at home, but these are not connected to the informatics system of the hospital. The patients “bring” the device into the hospital after the measurement has been taken and then data are fed into the informatics system. In the majority of cases, general practitioners are connected to the hospital system, but only to gain access to results, to make appointments, or to view laboratory findings.
The use of telemedicine and related e-health services is highly diverse among Hungarian hospitals. Twelve different telemedicine services were identified (teleradiology, telecardiology, telepathology, electronic storage of laboratory findings, teleneurology, Internet-based consultation, telemonitoring, online access for family doctors, use of mobile equipment, online appointments, online access to documents, and online access for patients). The average number of telemedicine services available in one hospital was 3.8. Three hospitals had none, and one hospital “boasted” of the highest number of nine. No connection was found between the location of the hospitals (in terms of more or less developed regions) and the number of available telemedicine services. In our opinion, the number depends, on the one hand, on the ambitions of the hospital management and, on the other hand, whether or not the hospital forms part of the Integrated Hospital Information System (IKIR) project described in detail later.
What are the main obstacles to the use of telemedicine? Based on the interviews, four factors were outlined: the level of IT infrastructure, lack of interoperability, lack of IT skills, and unresolved legal, technical, and other problems.
One reason for the relatively infrequent use of telemedicine is the low level of infrastructure. Statistical sources indicate a relatively high level of IT infrastructure inside hospitals in comparison with other European Union countries, but a low level of IT for telesolutions. 11 This picture was reinforced by the information gained from the interviews. Although personal computers and printers are available in all hospitals, their average age is 4.5 years, varying between 1 and 10 years. Laptops are available only for a small fraction of workers and usually for home use or for use in conferences. Point-of-care testing and mobile instruments are available in only 28% and 18%, respectively, of the hospitals where interviews were conducted. Moreover, not only the lack but also poor quality of available IT instruments, both in hospitals and at home (in the case of telework), acts as a main hindering factor, as the system requirements of certain telemedicine specialist areas are relatively high to achieve reliable results. Because of financial problems, the upgrading of IT instruments has been postponed in many hospitals. Further investment is also needed to have broadband Internet access installed, as slower Internet causes problems in the speed and quality of transmission of the information because of the large size of radiology and other files. Further investment is needed for software required for the operation of various telemedicine specialist areas. Thus, all the interviewed doctors underlined the problems of financing for infrastructure, broadband, and software as the most important hindering factor in the proliferation of telemedicine in Hungary.
Another problem stems from the lack of interoperability. Inside a hospital, laboratory findings are generally accessible, storable, and transmittable between departments, but this is quite rare between hospitals. The only hospitals that are able to gain access to information electronically from each other in a systematic way are those which form part of the IKIR. At the end of 2008, this amounted to 38 health institutions (more than 18% of the total), 15,000 healthcare employees (almost 8% of total), and 260 general practitioner practices (almost 4% of the total), and thus, it covers a relatively small part of the Hungarian healthcare system. Hospitals use different informatics systems, which in itself poses problems in data and file exchange. According to one of the interviewed doctors there are at least 20 different hospital informatics systems in use in Hungary's 140 hospitals. According to the findings, the 30 hospitals where interviews were conducted used 13 different, usually not compatible, information systems. In teleradiology, there are at least 10 different types of viewer software in use in Hungary. Further, incompatibility and lack of standards for the electronic format of laboratory and other findings also cause problems in the flow of information between hospitals and other healthcare institutes. This frequently results in the duplication of medical examinations. In conclusion, substantial savings could have been made by having central coordination and by the expansion of the IKIR system.
Another obstacle to the further spread of telemedicine could be the lack of IT skills. The findings show that this is an obstacle of secondary importance. However, medical workers have relatively narrow professional IT skills and knowledge, according to the results of the interviews. However, they are able to perform their tasks and use the hospital information system and other informatics tools that are necessary for their work. Older workers felt especially ill at ease with IT-supported systems. In our research, doctors and nurses were asked to evaluate their IT knowledge on a quartet scale. Doctors were usually satisfied with their IT skills, whereas nurses often admitted that they are only able to carry out their tasks, but do not have a wider IT knowledge and in some cases run into difficulties.
Training courses are available in all the examined hospitals, but they are usually very short and concentrate only on the most frequently carried out tasks. Hospital workers do not find the frequency and depth of training courses satisfactory and it is true that on average they are less frequent than in other European countries. 11 According to the results of the interviews, in a few cases, nurses and doctors are not even aware of the availability of certain telemedicine services in their hospital. Despite this, and contrary to initial expectations, the findings showed a positive attitude on the part of doctors, assistants, and nurses toward telemedicine and e-health. The overwhelming majority of the people interviewed claimed that telemedicine may potentially improve the quality and efficiency of the health service and decrease their workload. Despite previous bad experience or the present system, wherein IT-based and “paper-based” administrations are running parallel and result in a double workload on hospital workers, their overall attitude remained positive. Some reluctance was found on the part of doctors. They raised mainly professional problems such as unreliability of the evaluation of laboratory findings and the risk of misdiagnosis in the case of atypical diseases when there is no access to other findings with regard to the patient. Another group with a slightly negative attitude was composed of older workers.
Finally, there are many unresolved legal, technical, and other problems, which hinder the further proliferation of telemedicine in Hungary. The interviewed hospital workers were not experts on these issues and only cited those which they came across in their everyday work. For example, security of access and security of the informatics systems were deemed to be of vital importance, both of which require new hardware and software. The problems of data protection were also mentioned relatively frequently. Lack of regulation on digital signatures is also a hindering factor from the point of view of both doctors and patients. Because of regulatory and data protection problems, the wider use of IT and telemedicine has until now resulted in a higher administrative workload for nurses and doctors. Other technical problems related to the difficulty of integrating telemedicine into the existing national healthcare system were also mentioned. For example, integrating archives produced in the “old” system in radiology images into the new one is unresolved.
Discussion
In Hungary, telemedicine and related e-health services are in an initial phase but they are in relatively wide use by regional comparison, which may be explained by staff shortage and financing problems. This latter factor puts the emphasis on cost-saving solutions including telemedicine. Overall, there are major differences in the frequency of use of telemedicine among hospitals and among telemedicine specialist areas. Hospitals, which form part of the IKIR (an integrated hospital information system) and those with a more ambitious and active leadership excel. Teleradiology (in some cases in a reduced, “quasi” form) and electronic storage and transfer of laboratory findings are the most common, mainly because of staff shortages, the importance of these services in the overall healthcare process, and their cost-saving nature. There are many obstacles to the wider use of telemedicine, many of which are connected to a lack of central coordination and financing. Thus, problems with the quantity and quality of IT infrastructure, lack of interoperability, and unresolved legal and technical problems are the most important hindering factors. Lack of IT skills, although being a factor, is only of secondary importance. Moreover, there was no major acceptance problem of telemedicine among hospital workers.
Our recommendations are based on the most important obstacles identified by our research. First of all, a national strategy aimed at integrating telemedicine into the existing healthcare system, and one that takes into account the quality and quantity of both human and physical infrastructure, is indispensable. As some of the problems are connected to physical infrastructure, a high level of interoperability must be achieved. Second, as a major element of the national strategy, a list of unresolved technical, legal, and regulatory issues must be compiled and resolved. In our view, these technical problems must be resolved regardless of the type of the healthcare system's financing. Financing issues come to the fore in countries with centrally (state) financed healthcare systems. In these countries, additional resources are needed to finance the upgrading of physical and human infrastructure.
Footnotes
Acknowledgments
The authors express gratitude to the hospital workers who took part in the interviews and to Renata Anna Jaksa and two anonymous referees for their comments on a previous version of this article.
Disclosure Statement
No competing financial interests exist.