
Abstract
Introduction
With up to four comorbidities at the onset of dialysis and 40% of the patients developing a walking disability in the first year, 1 a large segment of the end-stage renal disease (ESRD) population is frail, disabled, and prone to illnesses requiring hospitalization. There have been significant advancements in the care of patients with ESRD, including improvement in dialysis, anemia management, 2 and bone and mineral metabolism, 3 yet there has been little overall change in the frequency of hospitalizations, particularly because of cardiac disease, pneumonia, septicemia, and soft tissue infections. 1 Many of these illnesses occur in the home setting, unrelated to the dialysis experience, and are potentially preventable. 4 At the present time, there are scant resources to equip the home environment with tools for prevention, such as self-monitoring equipment. The purpose of our research was to determine whether home-based interventions using telehealth technology can improve health outcomes and be economically sustainable to justify their use in the management of selected patients with chronic diseases who are frail and disabled. We are reporting the results of a pilot study comparing usual care (UC) with home monitoring via remote technology (RT) with remote care nurse (RCN) oversight.
Materials and Methods
Procedures
The study cohort was drawn from a population of patients with ESRD undergoing outpatient hemodialysis three times per week at a for-profit hemodialysis center (not affiliated with the Veteran's Administration). Patients were at least 21 years of age; had been on dialysis for at least 3 months; and lived at home with no additional services, such as home care, hospice, or community bathing/chore services. The Western Institutional Review Board and the Human Research Protection Office under the United States Army Medical Research and Materiel Command approved all human subject protocols.
The outpatient medical records of consented patients were reviewed to collect those data needed to calculate the risk score, a tool developed from earlier work. 5 Patients were stratified for risk of hospitalization in the ensuing 12 months. Patients with a risk score ≥1.2 were entered into a pool and assigned to one of two groups of the study by random selection.
Risk score=[(0.0018×age)+(0.2181, if peripheral vascular disease [PVD] present)+(0.3920, if albumin <3 g/dL)+1.1416 if Karnofsky score ≤60)].
A modified version of the Charlson comorbidity index, 6 a simple scale that predicts outcomes for patients with ESRD, 7 was calculated and has been included in the results because of its more common use in predicting future hospitalizations and mortality.
Description of Interventions
RT intervention utilized a commercial off-the-shelf home monitoring unit (VitelCare Turtle 500) that is Health Insurance Portability and Accountability Act (HIPAA) compliant and broadband enabled. Accessories included a blood pressure monitor, scale, pulse oximeter, glucose monitor, video camera, and headset. The video camera and headset provide videoconferencing capability (at arranged times) and is especially helpful in communicating with patients in rural areas. Trained personnel installed the equipment and provided instruction in the home until patients/caregivers were satisfied with the operation and reliability of the equipment. According to an individualized plan of care, patients captured their health measurements on nondialysis days (i.e., weight, blood pressure, oxygen saturation, and pulse rate). In addition, patients answered 10 health questions, subjectively rating their state of health and the functioning of their vascular access. Sample questions include the following: “Are you feeling sick today?”; “Is there a problem with your access/graft/fistula?”; “Are you having any new pain?”; and “Have you missed or skipped any medications?” The RCN reviewed all incoming data and contacted patients and caregivers via telephone if data were incomplete or outside of the range as determined by the plan of care. The RCN did not make home visits except to replace or troubleshoot malfunctioning equipment.
The UC group consisted of the usual dialysis care, including vascular access oversight, review of laboratory tests regarding adequacy of dialysis, and anemia management.
Measures
Objective measures
Data collected included the number of hospital and emergency room visits, the number of days in the hospital, and total charges for in-patient and emergency room services on all patients. All utilization variables are cumulative over an approximately 630-day period, although the period in the trial varied across patients.
Self-report measures
The medical outcomes survey 36-Item Short Form Health Survey (SF-36) measures quality of life (QOL) and has been validated in patients with ESRD. 8 The SF-36 is a multipurpose, short-form health survey consisting of 36 questions. It is an average of the mental health and physical health components. It was administered to all (both RT and UC) participants at baseline and at midpoint of the pilot study. The SF-36 score ranges from 1 to 100; QOL is deemed higher with increasing score.
Data Analysis Plan
The protocol was a randomized, nonblinded study with a per-protocol analysis of patient outcomes. Independent, one-tailed t-tests using SPSS version 18 were used to determine any significant mean difference between treatment and control groups (p<0.05).
Results
Demographics
Forty-four (44) patients were included in the analysis (19 RT patients and 25 UC patients) (Table 1). Of the 19 patients in the RT group, 7 were females and 12 were males. Of the 25 patients in the UC group, 11 were females and 14 were males. During the setup and training for utilization of RT, two patients could not master the technology and three others were not compliant with the protocol. These five patients were excluded from the study. The mean age was 57 for RT patients and 62 for the UC patients. Severity of illness as reflected by Karnofsky 9 assessment (RT 58.75, UC 57.5), modified Charlson comorbidity index 6 (RT 3.35, UC 4.8), and the risk score (RT 1.41, UC 1.35) was slightly higher in the RT group. Perceived QOL as measured by SF-36 scores (RT 63.9, UC 59.1) was also slightly higher. The total number of study days in the RT and UC groups was 6,711 and 8,352 days, respectively. The mean number of study days per patient was 353 for those in the RT group and 334 for those in the UC group.
Healthcare Resource Outcomes
Hemmelgarn et al.6
p<0.05.
ER, emergency room; SF-36, 36-Item Short Form Health Survey.
The frequency of hospitalizations (RT 0.0018 and UC 0.0056 per study day), the number of days in the hospital (RT 0.008 and UC 0.036 per study day), the number of emergency room visits (RT 0.0003 and UC 0.0019 per study day), and their associated charges (RT $114 and UC $322 per study day) were significantly less in the RT group. QOL, as measured by SF-36 scores, decreased slightly in the RT group (60.76) but remained the same in the UC group (59.5) from outset to midpoint of the study (6–9 months from the beginning of the intervention).
Patient–Clinician Interaction
The number of medical issues that required RCN-initiated contact for outlier clinical values or subjective changes in the clinical condition of patients in the RT group decreased from a total of 36 in the 1st month of participation to less than one episode at 21 months (mean=9.46 episodes per month) (Fig. 1). Medical issues represent positive responses to the 10 health questions patients answered as part of their RT intervention. Positive responses include outlier clinical values or subjective changes in patients' clinical conditions.
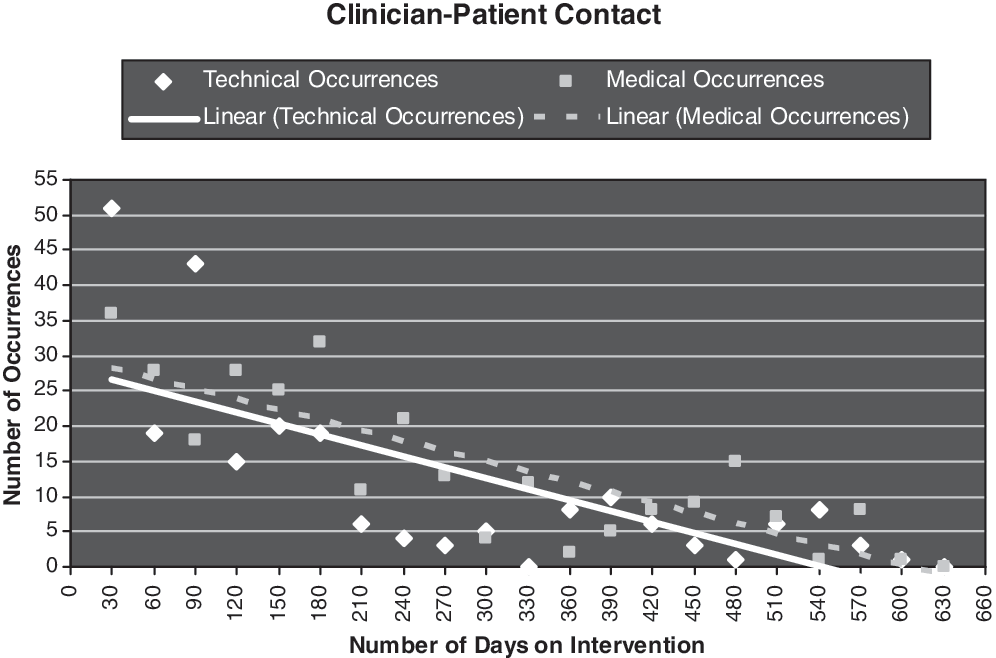
Clinician initiated contact with patients using home-based remote technology. Standardized coefficient for the relationship between the number of days in the study and technical occurrences is −0.717 (t-statistics=−4.484, p≤0.000). Standardized coefficient for the relationship between the number of days in the study and medical occurrences is −0.831 (t-statistics=−6.512, p−0.000).
The number of technical issues (usually involving the use of the remote monitors) for patients in the RT group decreased from 51 in the 1st month of participation to less than one episode at 21 months (mean=7.7 episodes per month) (Fig. 1).
As demonstrated in Figure 1, a comparison was made between the number of medical issues and the number of technical issues that occurred over a 21-month period. Both medical and technical occurrences decreased dramatically from the beginning of the intervention to the completion of the study.
Discussion
The results of this pilot study suggest that home-based RT with nurse–clinician (RCN) oversight can improve health outcomes with associated cost reductions in high-risk ESRD patients by reducing hospitalizations and emergency room visits. As 75% of Medicare dollars are expended on patients with chronic medical illnesses, the Centers for Medicare and Medicaid Services underwrote demonstration projects emphasizing chronic care coordination to best determine the pathway for improving quality of care and the efficiency of Medicare expenditures. A recent analysis of these programs found that the majority of these projects failed to meet the stated goals. 10 The few projects that showed promise featured personal contact between the patient and the care coordinator. The one program demonstrating cost reductions involved a group of patients who, at baseline, had the highest severity of chronic illness. 10
The patients in this pilot study were selected by a weighted formula including age, the presence of peripheral vascular disease, malnutrition, and a compromised ability to perform activities of daily living. The remote intervention program provided instant feedback of clinical measurements to the patient plus support and oversight from the RCN. The frequency of patient–nurse contacts for clinical issues decreased with time and was associated with an improvement in health outcomes when compared with the UC group. This suggests that the patients in the RT group may have assumed more responsibility and control of their health because of the intervention; however, the added dimension of nurse oversight should not be ignored. Further research on the effect of nurse–patient interaction on self-monitoring outcomes is warranted.
To be effective, chronic disease management programs must be tailored to the severity of illness and the needs of the patients. 10 For example, programs targeting patients with an asymptomatic single condition such as diabetes mellitus use clinical progression of disease as an outcome measurement. 11 These programs typically have a high patient-to-staff ratio and patients must be followed up for years to collect enough data to demonstrate a justifiable return on investment. We have targeted a different population with daily monitoring of clinical parameters and RCN follow-up for outlier values or subjective reporting of change in clinical wellbeing. The patients were projected to be at higher risk for hospitalization in the near term and considered to have limited skills for self-management of chronic illness. 12 Although beset by multiple comorbidities, the target population demonstrated the ability to change behavior and reduce serious unexpected medical events. We believe that patient empowerment was the result of the complex interaction gained from utilizing RT in conjunction with the clinical oversight and personal communication from the RCN. The improvement in outcomes was not reflected in the midstudy QOL survey. This finding is not surprising because the time period of the study may have been too short to measure change or, alternatively, the survey instrument (SF-36) may not ask the appropriate questions to measure the subjective impact of the intervention.
Limitations
A per-protocol analysis represents the best case scenario to determine whether the intervention had an effect. Patients randomized to the RT group were included in the analysis if they were capable and compliant with the protocol. The five patients in the RT group who dropped out or withdrew from the study may have represented a sicker subset of patients and introduced a bias in the analysis as a similar subset of patients remained in the UC group. However, the results of the intervention are compelling and warrant further study. Follow-up research should be conducted to allow intent-to-treat analysis of health outcomes and cost effectiveness, which we believe will demonstrate the value of RT with nurse–clinician oversight as an integral tool in the management of high-risk dialysis patients.
Footnotes
Acknowledgments
This work was supported by the Department of Defense U.S. Army Medical Research and Materiel Command Telemedicine and Advanced Technology Research Center under the award number W81XWH-07-2-0064. The U.S. Army Medical Research Acquisition Activity (Fort Detrick, MD) is the awarding and administering acquisition office. The authors are indebted to the cooperation and encouragement of Liberty Dialysis; The St. Francis Healthcare Foundation; Hawaii Medical Centers: Hawaii Pacific Health Hospitals; Queens Medical Center; and the unsung physician heroes: Drs. Rossini Botev, Randolph Chen, Shiuh-Feng Cheng, Jose Ganel, Leilani Kaanehe, Jim Musgrave, David Naai, Aaron Nada, Roland Ng, David Ono, Carmen Stanko, Jared Sugihara, Thomas Tasaki, and Eugene Wong. The authors are also most appreciative of the tireless work of Heather Thomas and Tamami Harada.
Disclaimer
The content of this research does not necessarily reflect the position or the policy of the Government, and no official endorsement should be inferred.
Disclosure Statement
No competing financial interests exist.