
Abstract
Introduction
The senior population in need of home care is growing. Healthcare institutions providing home care services currently have a hard time meeting the demand for such services. 1 In-home telerehabilitation, defined as the provision of remote rehabilitation services to individuals with persistent and significant disabilities through information technologies and telecommunications in their home, 2 is growing as a complementary or alternative intervention to traditional face-to-face therapy in home care and outpatient services. 3
In rehabilitation, teleconsultation between two healthcare services has been studied with patients requiring speech therapy, 2,4 –11 mental health, 12 and physical assessments such as for wounds, 13 –15 orthopedic, 16 –18 and neurologic conditions 19 and for assistive devices adjustment. 20 –22 Moreover, two studies investigated the accuracy of teleassessment in the field of telerehabilitation. 23,24
Few studies have been conducted in teletreatment between two healthcare services. Two studies in speech therapy for stroke disabilities compared teletreatment with face-to-face intervention. They both found no clinical difference in communication and language disorders. 25,26 In physiotherapy, a positive effect of teletreatment between healthcare and community services was observed in elderly with stroke 27 and knee pain. 28 No comparison group was included in those studies.
In-home teletreatment was performed in post-stroke rehabilitation, 29 –32 elderly with loss of functional autonomy, 33 elderly with mild or moderate dementia, 34 multiple sclerosis, 35 and total knee arthroplasty (TKA). 36 –39 The results of those exploratory studies without a control group support the feasibility of in-home teletreatment.
Until now, little is known about the satisfaction of the participants receiving teletreatment with physiotherapy and the health professionals delivering the services. Satisfaction is an important indicator of the degree of efficacy. 32 A high level of satisfaction increases the patient's motivation and improves treatment compliance. Some studies concerning patients' satisfaction with teletreatment already demonstrated that they were satisfied with the technology and with the way they received care. 3,40 More specifically, conventional physiotherapy and teletreatment have demonstrated comparable levels of satisfaction in the samples studied. 41 Similar conclusions were reached for telerehabilitation with a post-stroke population. 32
Lastly, a telerehabilitation study in a simulated in-home environment for post-knee arthroplasty patients demonstrated a high level of satisfaction with services and rehabilitation outcomes. Therapists were also satisfied with the outcome of treatments. 39 However, satisfaction was measured with nonstandardized or nontelerehabilitation-specific questionnaires. Indeed, none of these articles studied the different aspects influencing the satisfaction of users (healthcare professionals or patients) with the technology used or the care provided. These aspects include satisfaction with care provided, perception of telehealth, satisfaction with telemedicine services, and subjective appreciation of the technical quality.
In this context, the purpose of this study was to investigate the satisfaction of patients and health professionals with in-home teletreatment as an alternative to face-to-face therapy for individuals at home following discharge from an acute care hospital after TKA.
Methods
Sample
This study was embedded in a larger controlled trial on the efficacy of in-home teletreatment following TKA. 42 People who had TKA were recruited prior to discharge from two acute care hospitals: the University Hospital of Sherbrooke and the University Hospital of Quebec. These hospitals provide orthopedic services for a metropolitan (Quebec City and region) and an urban (Sherbrooke and region) area in the province of Quebec, Canada. The study was approved by the ethics committees of the two university hospitals.
Recruitment and Randomization
The design was a randomized trial. All the potential participants were first approached by their hospital physiotherapist in the postoperative unit to determine their interest in receiving information about a research project on in-home telerehabilitation after their discharge from hospital. Positive responses from potential participants were followed up by planned visits to their bedside by a research assistant to formally explain the project. With the candidate's permission, the availability of high-speed Internet access at their home was checked by a broker who was in contact with different regional Internet service providers. Once it was determined that high-speed broadband access was available, the candidate's informed consent to participate in the study was obtained. The participants were then randomly assigned to the telerehabilitation group (Tele group) or home care/outpatient clinic group (Comparison group).
For the Tele group participants, installation procedures to ensure high-speed Internet access in the home were coordinated with the Internet service providers and put in place in each home within 5 days of the patient's discharge from hospital. Following activation of the high-speed Internet connection, a research assistant went to the patient's home to install the telerehabilitation equipment and conduct tests to verify the quality of the Internet connection. It took about 1 h per home to complete the installation and conduct the communication tests. The telerehabilitation equipment was picked up by the research team at the end of the planned telerehabilitation period (2 months). For the Comparison group participants, they were referred by the institution to the usual home care/outpatient clinic services.
Technological Infrastructure for Telerehabilitation Services
Based on experience gained in a previous study, 43 a telerehabilitation platform consisting of two H264 videoconferencing CODECs (Tandberg 550 MXP) with integrated wide-angle view cameras, remote-controlled pan, tilt zoom (PTZ), 20-inch liquid crystal display (LCD) screens and a dedicated modular software interface for user-friendly control of videoconferencing connections, PTZ camera functions, and external devices was used. 44 The telerehabilitation platform and software interface for the clinician are illustrated in Figure 1. The platform was developed to ensure that interactions between clinicians and clients during the telerehabilitation sessions were not impeded by technology but facilitated with user-friendly interfaces. A special effort was made to provide a mouse-based interface to intuitively control, from a unique screen through point-and-click or area zoom, PTZ camera functions at both sites.
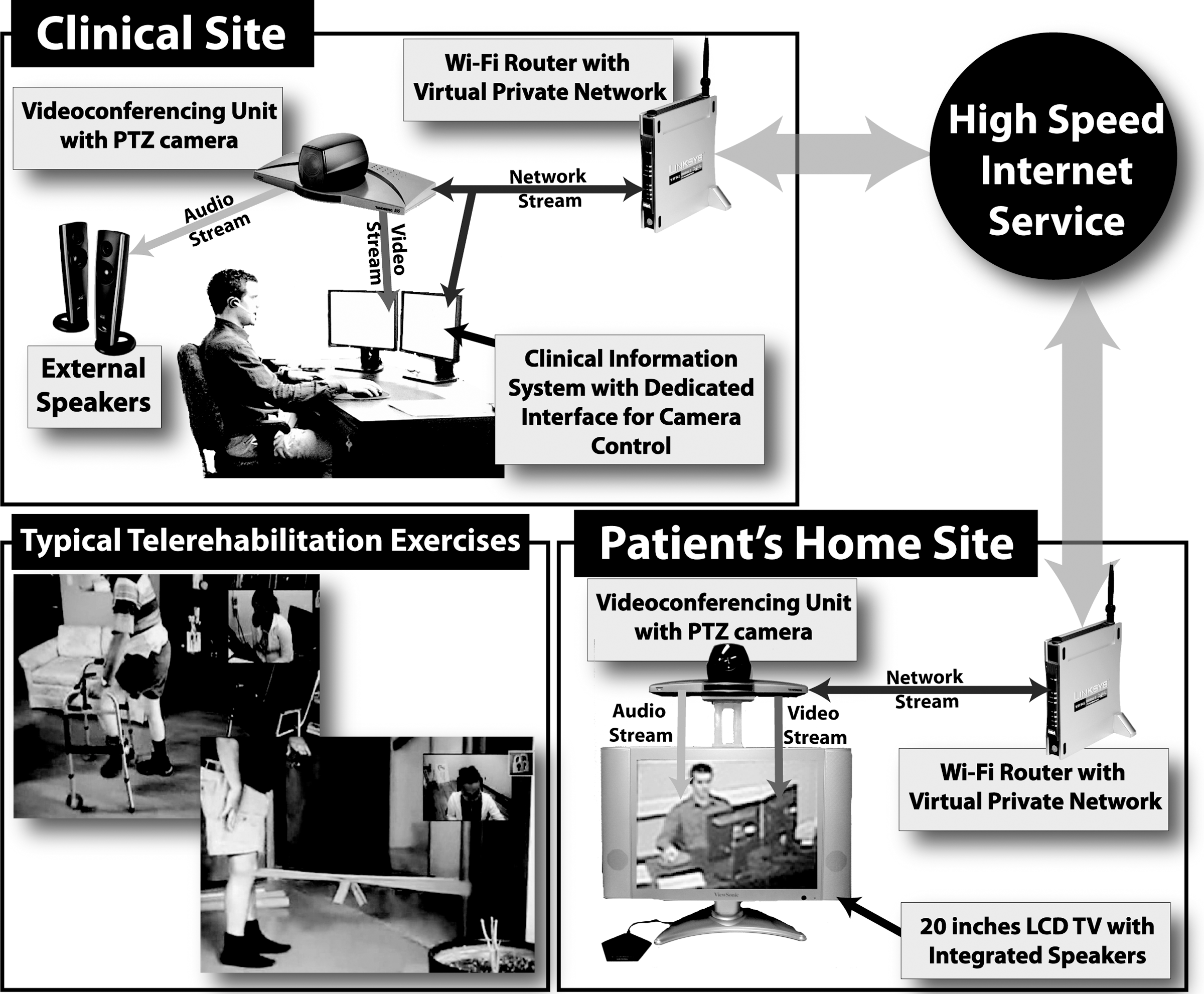
Technological infrastructure for telerehabilitation services.
Physiotherapy Intervention
Both interventions (teletreatment and home care/outpatient clinic) focused on functional rehabilitation. They were based on a functional approach to reduce disabilities and improve function in daily activities through progressive exercises building on the gains made by each patient. The mean duration of each therapy session was about 1 h of treatment (including treatment assessment and recommendations between treatments). The teletreatments were delivered to the participants at a rate of two sessions per week for 8 weeks (total of 16 sessions). The home visit/outpatient clinic treatments were delivered as usual over a period of 2 months on average, and the number of sessions was not controlled by research procedures but took place as usual in home care/outpatient clinic services. No change was made in frequency, duration, or exercises.
For the teletreatment group, someone was expected to be at the participant's home during teletreatment to ensure the patient's safety during transfers and locomotion as well as in case of emergency. This person could be a family member or friend who had received prior training on the implementation of the technology that had been installed, but not on the therapy.
Variables and Instruments
Patients' perception of telehealth
Patients' perception of in-home telehealth was assessed when the telerehabilitation equipment was installed and again when it was removed using the in-home telehealth patient's perception questionnaire. This questionnaire was known to have a high reliability test–retest and a good validity about patient's perception with telehealth services. For this study, French adaptation of the Telemedicine Perception Questionnaire was used. 45 It contains 17 questions on telerehabilitation perception and is answered on a 5-point Likert scale, wherein “1” represents “no opinion” and “5” represents “completely agree.” The total score is the sum of all the scores. The highest possible score is 85, which indicates a positive perception of telehealth services. This questionnaire can also be used to objectively assess the technical appreciation of telemedicine users to improve its application.
Patients' satisfaction with healthcare services received
Patients' satisfaction with healthcare services was assessed with the French version of the Healthcare Satisfaction Questionnaire. This questionnaire showed a good internal consistency (Cronbach's alpha coefficient of the overall scale=0.92). 46 Moreover, the multidimensionality nature of the concept of satisfaction was analyzed through the presence of three factors: satisfaction with the relationship with the healthcare professional, satisfaction with the services delivered, and satisfaction with the general healthcare organization. This questionnaire contains 26 questions answered on a four-point Likert scale, wherein “1” represents “not at all satisfied” and “4” represents “highly satisfied.” The total score can be computed as the mean overall satisfaction for the three factors. Higher scores indicate a higher level of satisfaction.
Health professionals' satisfaction with the technology
Satisfaction with the quality and performance of the technological platform was assessed with a technical quality subjective appreciation questionnaire. 47,48 This questionnaire showed a high reliability (Cronbach's alpha=0.80) and evidence of validity with respect to perceptions of telehomecare. 49 Physiotherapists completed this questionnaire at the end of each treatment session. The questionnaire comprises five items on the technical quality of teletreatment sessions. The first three items refer to the physiotherapist's observations concerning the difficulties experienced with the technology at the treatment site. The two last items relate to audio or video problems experienced by the patient. Answers are scored from 0 to 3, with “bad” (0) representing problems persisting during the whole therapy session and having a significant impact on quality of care, “insufficient” (1) representing significant technical problems that had an important impact on quality of care, “satisfactory” (2) representing occasional problems having a small impact on care quality during treatment sessions, and “good” (3) representing an absence of technical problems during the session. The score is computed as the sum of all the answers: a maximum score of 15 signifies an absence of technical problems during the session. Also, we added three questions to the original questionnaire, each of which is answered on a scale from 0 to 10, with 10 being the highest level of satisfaction. The first two questions relate to the clinical assessment of the session according to treatment goal achievement and relationship quality. The last question is related to overall satisfaction with the treatment session.
Data Collection Procedure
Patients' satisfaction with the services received was assessed at the end of the intervention (T2) for both groups. For in-home telehealth perception, the questionnaire was completed at T1, performed in the first 5 days after hospital discharge (before the beginning of the intervention), and T2, but only for the Tele group. Healthcare professionals' satisfaction with the technological platform performance and quality was measured at the end of each treatment session.
Statistical Analysis
Descriptive statistics for each variable were produced to generate a profile of the sample studied. Telehealth perception change was computed with a Wilcoxon signed rank test for two dependent samples. The same test was used to compare the level of satisfaction with telemedicine between patients and physiotherapists. To compare satisfaction levels between intervention groups, Mann–Whitney U test for independent samples was used. Finally, proportions were also calculated for the quality assessment and technical performance questionnaires that were completed by the physiotherapists.
Results
Descriptive Statistics of the Sample
The original 48 participants were randomized into two groups: Tele and Comparison (Fig. 2). In the Tele group, two participants were lost during follow-up: one left immediately after randomization and one was excluded for medical reasons (vagal shock and unknown reason). In the Comparison group, four participants were lost: three decided to leave the study immediately after randomization (they had expressed a preference to be in the Tele group) and one had surgery for an aneurysm in the leg. It should be noted that the participant who had been dropped from the main study for a medical reason was kept for this study because he had received four teletreatments and every questionnaire at T1 and T2 had been completed. The analyses for the present study thus involved a total of 42 participants (mean age: 66.4±11.6). No difference was found between the participants in the two groups on variables potentially related to the outcome: age, schooling, and number of hospitalized days after surgery (Table 1).
Descriptive Statistics of the Sample
Mann–Whitney test for two independent samples.
SD, standard deviation.

Flow diagram of the study.
Telehealth Perception Change
Patient's perception of in-home teletreatment was positive when the equipment was installed (81.2%±7.2%) as well as when it was removed (83.4%±8.3%). This difference was not statistically significant (p=0.118).
Patients’ Satisfaction with Healthcare Services
Satisfaction with the healthcare services provided was also high for both groups (Table 2). No significant difference was observed between the Tele and Comparison groups for the total score or for each individual factor considered. The Tele group participants were thus as satisfied with the services received as the Comparison group.
Intergroup Comparison of Satisfaction with Services Received
Mann–Whitney test for two independent samples.
Health Professionals’ Satisfaction with the Technology
The quality and performance of the technological platform perceived by the professionals was calculated using the average of the ratings obtained, on a per question basis, for all the telerehabilitation sessions. Concerning the reliability of the technological environment, the physiotherapists found it satisfactory for 45.5% of the time and good for the rest of the time (54.5%). They also rated the voice/image synchronization as satisfactory for 13.6% of the time and as good for 86.4% of the time, the refresh rate of the images as satisfactory for 22.7% of the time and as good for 77.3% of the time, and the sound quality as satisfactory in 13.6% of the cases and as good in 86.4%. Finally, the operability of the peripherals was insufficient for 5% of the time, satisfactory for 13% of the time, and good for 82% of the time.
Discussion
The main goal of this embedded study was to investigate users' and physiotherapists' satisfaction with post-TKA in-home telerehabilitation. To our knowledge, this study is the only one to examine both patients' and physiotherapists' satisfaction while also evaluating the quality and performance of the technological platform used. Based on these results, we can now affirm with robust data that teletreatment is a suitable alternative in the continuum of care; it is no just a feeling, but an evidence-based statement. As a multidimensionality of the satisfaction was assessed, it appears to be useful for measuring and advancing knowledge about healthcare and services satisfaction.
One of the first characteristics studied was the patients' trust in telerehabilitation. Contrary to what was originally expected, the initial level of trust was very high when the technological platform was installed. It was so high that no significant difference was found in trust level between the time of installation and removal for these older adults. The timing of the questionnaire might also have influenced the results. As they completed the questionnaire during the technological platform installation, participants did not have to imagine what it would look like and might have been reassured by this knowledge, thus influencing their answers. Another factor that might have had a positive impact on the trust level was the close follow-up provided to the participants, right from the beginning. That being said, the fact that no significant difference was found in trust level when the equipment was removed shows that use of the technological platform did not change the patients' perception of and trust in telerehabilitation, which were very positive.
An important observation can be made regarding the patients' satisfaction levels. Three main aspects of patient satisfaction were covered by the questionnaire used: satisfaction with the relationship with the therapist, with the services delivered, and with the organization of services. The results show that although there was no direct contact between patient and physiotherapist in the telerehabilitation context, the levels of satisfaction were as high in the Tele group as in the Comparison group. These results agree with those of Piron et al. 32
Patient satisfaction is very important as it is related to motivation and treatment compliance. 32 However, for telerehabilitation to become mainstream in clinics, it is essential that healthcare professionals using the technology are satisfied with it. Even though this new treatment tool is very promising in terms of cost, time, and efficiency, if it does not meet all of their needs well, physiotherapists will never embrace the technology.
As Russel et al. 39 previously demonstrated, the present study again shows that physiotherapists' satisfaction with regard to goal achievement, patient–therapist relationship, overall session satisfaction, and quality and performance of the technological platform is high. This is promising for the future of this treatment alternative.
Certain biases may have affected the internal validity of the study and warrant discussion. First, the issue of selection must be addressed. Randomization allocates participants to create comparable groups based on clinical variables potentially related to recovery after surgery. However, patients who agreed to participate in this new way of delivering services may have been more favorable to using computers. Specifically, in this study on satisfaction, potential bias was not eliminated. Controlling computer use should be included in a future study.
Information bias was a big challenge. Indeed, standardization of independent assessors should have increased the validity of data collection. The same standardization was done for the two sites at the same time. Strength of this study was the use of standardized tools for most of the variables. Thus, we can be confident that it has good internal validity.
This article studied patients' satisfaction with a telerehabilitation alternative compared with standard face-to-face treatment. Results show that the patients' satisfaction was high with both the telerehabilitation itself and the technological platform used for that telerehabilitation. The level of satisfaction was as high as that of one of the patients receiving traditional physical therapy. The physiotherapists' satisfaction was also high. In addition, the proposed technological platform demonstrated both high quality and performance. At-home telerehabilitation thus seems to be a promising alternative to traditional face-to-face treatments. However, it would be interesting in future studies to compare the results obtained in this study about the health professionals' satisfaction with teletreatment with their satisfaction with conventional therapy.
Footnotes
Acknowledgments
The authors thank all participants for their contribution to this project. This research was supported in part by a grant received from the Fonds de la Recherche en Santé du Québec (FRSQ)-SAAQ-AHQ-AÉRDPQ.
Disclosure Statement
No competing financial interests exist.