
Abstract
Introduction
According to the National Center for Health Statistics, one in four deaths in the United States is due to cancer. 1 In the arsenal of treatment modalities used to manage the disease, proton radiation therapy is a relatively new weapon. Because the technology involved in producing and delivering protons is quite complex, the cost of developing multiroom proton therapy centers is significant (anywhere between $150 and $250 million dollars depending on the number of gantries deployed). At the time of writing this article, there were only nine centers in the United States offering comprehensive proton radiotherapy.
Through public law, a partnership was established in 2004 between the hospital at the University of Pennsylvania (UPenn) (Roberts Proton Therapy Center) and the Walter Reed Army Medical Center (WRAMC) (Department of Radiology–Radiation Oncology Service) to engage in several areas of research as it pertains to the delivery of proton radiation therapy. One of the goals of this grant was the development of a robust remote proton radiotherapy treatment planning system to (1) facilitate the determination of protocol eligibility and enrollment at the local level, (2) eliminate duplicate consultations by different radiation oncologists, duplicate tumor board reviews, and duplicate image staging, and (3) significantly reduce the patient's time away from work and family by performing the entire treatment planning process remotely (i.e., simulation, fabrication of immobilization devices, contouring, plan creation, dose calculation, and plan approval and prescription). Although the field of radiation oncology has used telemedicine in the recent past, 2 –6,34 and more specifically, as it applies to both Department of Defense (DoD) and Veterans Affairs beneficiaries, 7,8 we believe our solution pushes a new frontier.
Materials and Methods
Building upon our experience with the “Remote Proton Radiation Therapy over Internet2” prototype, 9 our research program has developed a hybrid telemedicine solution that offers the following functionalities to the remote cancer-care provider: (1) ability to conduct both planned or ad-hoc high-definition audio-videoconferences with one or more sites, (2) ability to upload treatment plans to a shared folder via a secure virtual private network (VPN) connection, (3) sharing of treatment planning applications with authorized users for the purpose of optimizing/validating prescriptions, and (4) seamless integration of the hybrid design with existing multipoint control units (MCU) for calls involving more than two sites.
This hybrid solution merges a high-definition video teleconferencing (VTC) unit configured over an integrated services digital network (ISDN), 10,11 with an internet protocol (IP) 12 CITRIX client. Before selecting a desktop VTC unit, our research program looked at all available models from both Polycom and Tandberg. Demonstrations at the American Telemedicine Association Annual Meeting (Nashville, 2007 and Seattle, 2008) and in-house (Directorate of Information Management) confirmed that all units would meet our requirements in terms of connectivity (IP) and quality (minimum of 640 by 480 pixels). Our engineers seemed to have a slight preference for the Tandberg models, for both their Joint Interoperability Test Command (JITC) certification and their substantial use within the DoD network. Once confronted with the option of going either SD (standard definition or 480i max resolution) or HD (high definition or 1080i/720p max resolution), we opted for the latter, anticipating that future improvements in network capabilities would result in improved visual content for the users.
Our choice was the Tandberg 1700 MXP, a 20-inch widescreen LCD with a high-definition audio-videoconferencing unit equipped with a built-in HD camera. Of the four units we initially purchased, two had the embedded multisite functionality, thus turning them into a portable MCU for up to four sites. The Tandberg further gave the ability to place calls up to 2 megabits-per-second with H.235 encryption. With true CD-quality audio, protection against network interruptions for point-to-point calls, and superior video quality (H.264 standard), the 1700 MXP seemed like a very robust desktop HD VTC solution. Finally, the 1700 could also serve as a PC monitor, thus doubling the virtual workspace of physicians.
Three of these hardware codecs were initially purchased for evaluation, at a cost of $8,000 per unit. Two were placed at the WRAMC (Radiation Oncology Service) and one at the UPenn (Department of Radiation Oncology). The three units were configured over their respective networks (MEDNET and UPHS).
For the two Walter Reed units, connectivity was achieved via an IP connection from the endpoint itself to a Tandberg Codian gateway. Both were assigned phone numbers by the United States Army Medical Information Technology Center (USAMITC); calls placed from these units are therefore IP pre-gateway and ISDN post-gateway. UPenn is using a similar setup at their end, having their endpoint connected via IP to their Polycom RMX 2000 bridge and also registered with their gatekeeper/gateway for ISDN calls.
Our current setup (Figs. 1 and 2) pairs a Tandberg 1700 MXP with a standard 21-inch flat-screen liquid crystal display linked to a clinical computer. For its application-sharing function, our research program initially selected Defense Connect Online (DCO), an Adobe Connect product developed for the DoD. We tested both the DoD version and the commercial version of the core product. Both of those allowed us to evaluate window management (note, chat, attendee list, camera, share), as well as application sharing. DCO, based on the professional version of Adobe Connect, also offered additional functionalities, but those were of no particular benefit to our program (meeting recordings, administration and reporting, large events and polling, etc.).
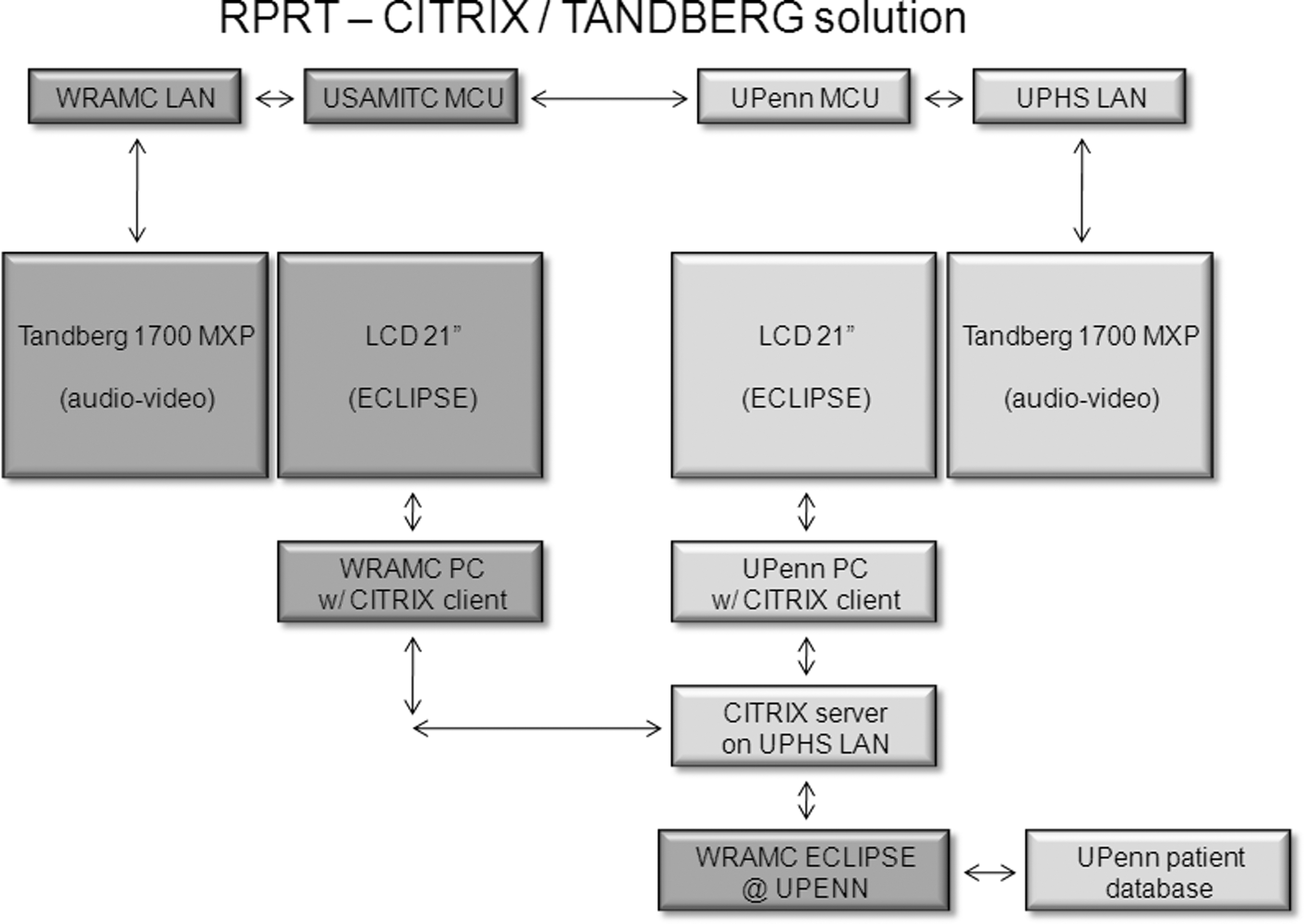
Schematics of the hybrid solution (part 1).
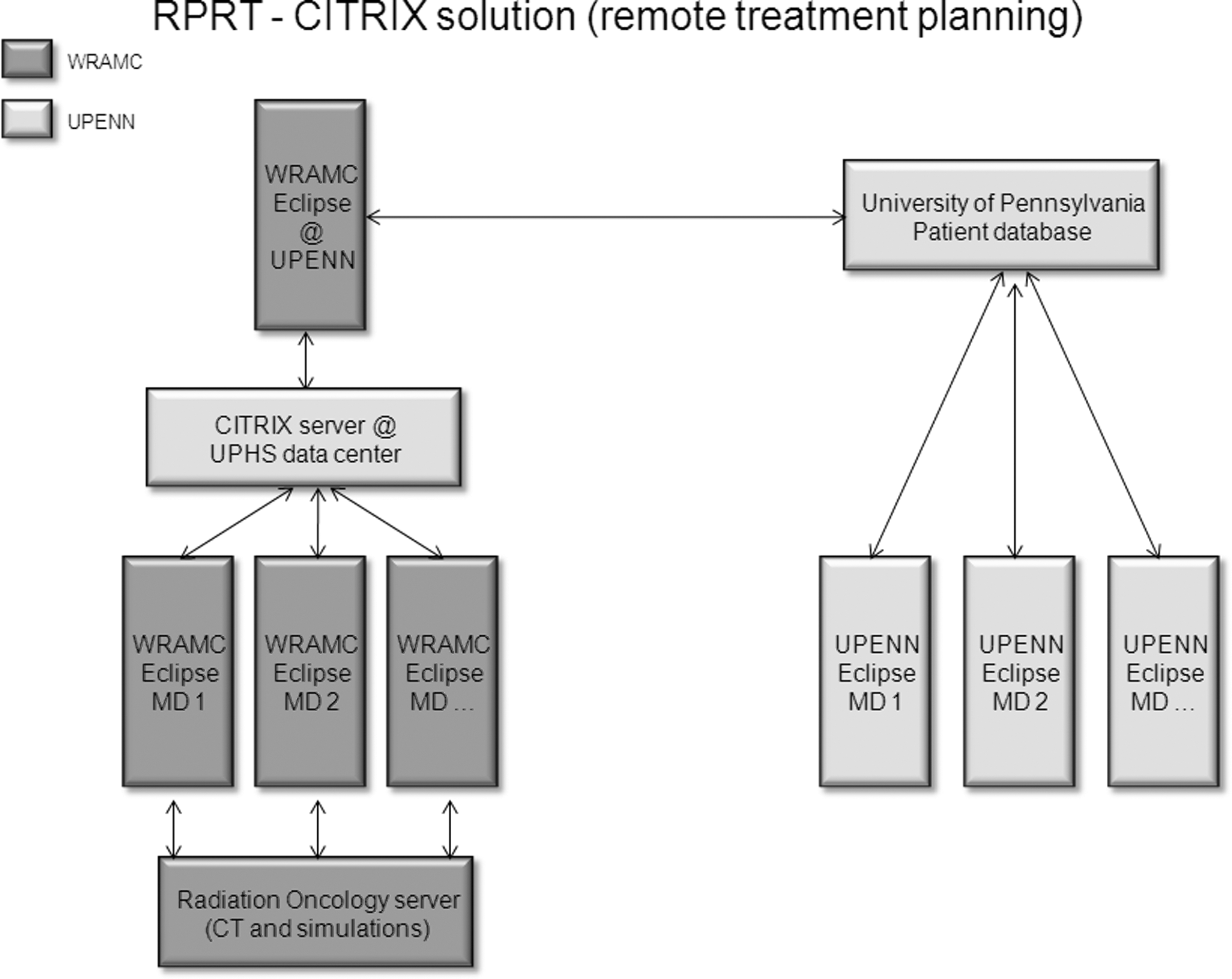
Schematics of the hybrid solution (part 2).
Although free, DCO came with several drawbacks: (1) only individuals affiliated with the DoD can create an account and therefore open a room for data collaboration and (2) calls have the potential to be recorded and subsequently reviewed by staff who did not receive Health Insurance Portability and Accountability Act (HIPAA) certification. Because the risk of compromising a patient's protected health information was very real, our program decided to abandon this platform to focus instead on a CITRIX client for both the secure transfer of patient files and the sharing of the treatment planning application.
CITRIX is a powerful application granting users not only the ability to transfer files securely from their local workstation to a remote site, but also take control of an application remotely. In addition, the “shadowing” function allows the far user to also take part in any remote session, thus offering the ability to collaborate dynamically in real time. CITRIX is not only endorsed by the DoD, but also certified to meet all current HIPAA requirements. The application being accessed via CITRIX is an Eclipse treatment planning platform (Varian Medical Systems), enabled for both photon and proton calculations.
A CITRIX server was purchased by the research program and subsequently configured on the UPHS network; 20 licenses were also acquired for our users. The evaluation itself was performed on a UPenn system temporarily dedicated for DoD use (ultimately, a Walter Reed Eclipse workstation has to be transferred to the UPenn as part of this comprehensive solution).
Results
As the solution was being designed, our program developed a standard operating procedure (SOP) to account for the inclusion of telemedicine equipment for both communication and treatment planning purposes. Tests were conducted over a period of a year and a half to ascertain the robustness of the solution. Although the SOP offers two alternative ways of conducting proton treatment planning, our evaluation focused on “remote planning on Penn server from DoD MTF” (Fig. 3), which we feel provides the greatest benefit to the telemedicine community.

Standard operation procedure (SOP) flowchart for the use of this solution in radiation therapy.
The testing of the VTC link itself took about 12 months, as connectivity problems persisted despite numerous software refreshes and reconfigurations. Although both Tandberg and Polycom equipments are intended to follow industry standards, compatibility issues prevented us from achieving full bilateral connectivity (failure by UPenn to receive video) until the Tandberg development team was able to replicate and test our setup in their own laboratory. Once the issue had been identified and corrected, a patch was applied to the Codian gateway, the Tandberg device that integrates ISDN and IP networks. Since then, our two sites have been able to enjoy full bilateral connectivity (audio and video).
The feedback from users has been overwhelmingly positive. Time delay, a limit of both hardware and bandwidth, 13,14 is a problem often reported by users of telemedicine systems. Our solution offers not only real-time feedback, 15,16 but also fluidity of motion and optimal resolution 17 for treatment planning.
Patient selection and enrollment occurs either on-site (weekly rotation of DoD radiation oncologists to UPenn) or remotely (telemedicine solution). Once enrolled into a proton radiotherapy course of treatment, the DoD patient is scanned at Walter Reed and the CT sets acquired are subsequently transferred from the servers to the local drive of the user's treatment planning workstation.
The CITRIX application itself is launched through a small “executable” (CITRIX Secure Access Client). Once the connection is established, users can then access the UPenn Intranet (UPHSNET) and, subsequently, the treatment planning application. The CITRIX encryption technology (AES 256-bit) guarantees the integrity of any protected health information being transmitted over the Internet, as required by HIPAA. The UPenn Health System created a specific “user group” with rights to access the treatment planning package. Each user within that group (radiation oncologists, medical physicists, and dosimetrists) was assigned a specific login and password combination for both CITRIX and Eclipse access, further strengthening security.
Once the user has taken control of the workstation located at the UPenn (used to contour normal structures/targets and design treatment plans), the mapped “C:” drive allows the user to seamlessly import these files into the Eclipse software; the treatment plan subsequently generated is automatically saved on the UPenn patient server (i.e., no manual transfer of files required).
Any issues arising during the planning process, or the treatment itself, give rise to an ad-hoc call using the Tandberg 1700 MXP audio-videoconferencing units to examine and troubleshoot the issue dynamically.
This hybrid solution not only ensures the involvement of a DoD radiation oncologist in the proton planning of his or her patients, but also prevents a certain degree of redundancy, such as rescanning of patients (a time saving of up to several weeks) or restaging (identical immobilization devices at both sites).
Although our tests relied on three units (two of which had the multisite functionality), this SOP assumes that all caregivers involved in remote proton planning will be equipped with both a high-definition desktop VTC unit (Tandberg 1700 MXP or Polycom 4000 HDX) and a CITRIX client on their treatment planning workstation.
Discussion
As network and computing capabilities improve, telemedicine is increasingly moving away from the now relatively trivial transfer of static images 18 –20 to more complex clinical activities, such as telesurgery 21 or, in our case, dynamic treatment planning.
As reported in our previous publication, our initial prototype did not move past the testing phase, but we hope that satellite institutions will still view the Polycom PVX software solution as a cost-effective and worthwhile solution to conduct point-to-point (and multipoint, should a bridge be available as a resource) VGA-quality audio-videoconferences. In addition, its data collaboration features, whether those take the form of sharing a desktop (still images) or an application (dynamic collaboration), can greatly enhance the experience of far-site physicians seeking increased “involvement” in the treatment of their patients. In particular, we did welcome the capabilities of PVX to integrate with existing MCUs to accommodate desktop-driven conferences for more than two participants. For the field of radiation oncology, this product could provide main hospitals and their satellite institutions with a cost-effective platform to conduct both virtual tumor boards and dosimetry conferences with participating institutions. 22 –25 Although this prototype solution was not adopted by our program, the lessons learned enabled us to develop the vastly superior system we have now (Fig. 4).

Strengths and weaknesses of both solutions.
The choice to go with a hybrid system, one relying on ISDN and IP rather than IP alone, was guided by the fact that a DoD-run network exists to run audio-videoconferencing (MEDNET VLAN). We were further assured by the Walter Reed Directorate of Information Management that conducting VTCs over an ISDN line was a much more robust and secure approach. 26 Respecting patient privacy, and data security as a whole, we went by the guidelines offered to us and therefore went for an ISDN videoconferencing solution.
Our hybrid remote proton therapy treatment planning solution not only improves access to a scarce treatment modality 27,28 for both patient and provider, as a telemedicine solution, but also has the potential to bring the cumulative expertise of all oncology specialties (gynecological, medical, pediatric, surgical, and radiation) to extend collaboration and education among the cancer-care community. 29 –32
Although the cost of the hardware may present a budgetary challenge for smaller clinics, 33 the approach we propose will naturally scale upward as network capacities are expanding, giving users the ability to see and hear in high definition, while engaging in the real-time remote manipulation of complex treatment plans. The solution also gives users the ability to seamlessly interact, as if working side by side. The benefit to our patient community is also very real and quantifiable, as their time relocating to Philadelphia for treatment will be minimized because of the existence of this telemedicine solution (needlessness of repeating scans, simulations, and planning of treatment); in routine cases, the net time savings associated with this solution is estimated to be between 1 and 3 weeks per patient.
Conclusions
Our robust remote treatment planning telemedicine solution offers a path toward greater integration of military treatment facilities, or satellite clinics, into regional proton therapy centers.
Footnotes
Acknowledgments
This work was supported by the US Army Medical Research and Material Command (DAMD17W81XWH-04-2-0022 and W81XWH0720121). Our research program further recognizes the contributions of the following individuals for their efforts: Lew Harvey, Nyere Hollingsworth, Desire Duckett, and Margaret Russell from WRAMC–Directorate of Information Management; and Brendten Eickstaedt, Scott Galper, Gary Robinson, Teresa Corbo, and Heathyr McNiece from the UPenn Health System. Mr. Chuck Martin (Varian Medical Systems) was also instrumental in helping to configure the CITRIX solution. Additionally, the authors thank COL(R) Michael Brazaitis, M.D., former chairman of the Department of Radiology at WRAMC, for the resources provided to further this work.
Disclaimer
The opinions, interpretations, conclusions, and recommendations in this article are those of the authors and are not necessarily endorsed by the US Army.
Disclosure Statement
No competing financial interests exist.