
Abstract
Introduction
Representing an increasingly prominent method of healthcare delivery, telemonitoring is generally defined as the remote collection of patient biologic data for management of chronic medical conditions, most notably heart failure, hypertension, diabetes, and chronic obstructive pulmonary disease. Medical providers will likely encounter increased utilization of telemonitoring, due both to a demographic increase in the aging population and as an alternative strategy to improve practice efficiency. 1
Increasing evidence attests to the clinical utility of home telemonitoring in chronic disease management. 2 In studies involving the use of home telemonitoring, a reduction in both mortality and hospitalizations has been demonstrated in patients with congestive heart failure, 3 as well as improvement in blood pressure and glycemic control in patients with diabetes mellitus. 2,4 Due to the high incidence of chronic disease in the elderly, as well as the aging of the population, it is critically important to understand elderly patients' feelings and perspectives toward telemonitoring to minimize any barriers to implementation.
Previous studies of patient satisfaction with home telemonitoring have generally demonstrated favorable results. In a group of younger patients with chronic heart failure (mean age of 60±11 years), compliance with telemonitoring was excellent. 5 A systematic review of telemonitoring studies concluded that the majority of patients are readily accepting the use of remote monitoring devices. 6 Satisfaction rates in more elderly populations with complex illnesses have not been comprehensively studied to date. In a Canadian pilot study of 22 older patients (mean age 73 years, range 60–88 years) with mixed chronic illnesses who underwent a qualitative focus group study of telemonitoring techniques, three patients discontinued the use of telemonitoring due to concerns with convenience. However, the consensus opinion was positive; with most patients feeling home surveillance monitoring may preclude office visits. 7
We performed a qualitative telephone survey of 20 randomly selected patients currently participating in an ongoing randomized trial of telemonitoring in older adults with complex medical illnesses (Tele-ERA; registered clinical trial NCT01056640). 8,9 Enrollment criteria for the Tele-ERA study include age ≥60 years and scoring in the highest 10th percentile on the Mayo Clinic Elderly Risk Assessment Index; this index is derived from a composite score of previous hospitalizations, age, and significant comorbid medical conditions, with a higher score indicating advanced-risk health status. 10 A high Elderly Risk Assessment Index score was used as a criteria for inclusion into the study to target older adults with significant comorbid medical illnesses at high risk for hospitalization, emergency department visits, and death. Patients were randomized to either daily home telemonitoring or standard care for 1 year. Daily monitoring was done with the Intel Health Guide, which has the ability to monitor weight, blood pressure, heart rate, pulse oximetry, peak flow, and glucose values as well as ask questions on self-reported symptoms. Specific monitoring parameters are chosen based on individual patients' diagnoses. Review of the results of the daily monitoring was performed by dedicated nurses.
Medical issues that arise during telemonitoring are addressed by the monitoring nurse with input by a geriatric nurse practitioner or the patient's primary care provider when needed (Fig. 1). A scheduled video conference visit through the Intel Health Guide is performed within 1 week of enrolment to the study and after any hospital discharge. Additionally, videoconferencing is available on an as needed basis throughout the study to address health concerns. Patients are trained to use the monitoring system by a clinical assistant, who is then available throughout the course of the study for any questions that may arise in the use of the equipment. Patients interviewed for this survey had been enrolled in the study and used the monitoring equipment for a period of 8–17 weeks at the time of the survey.
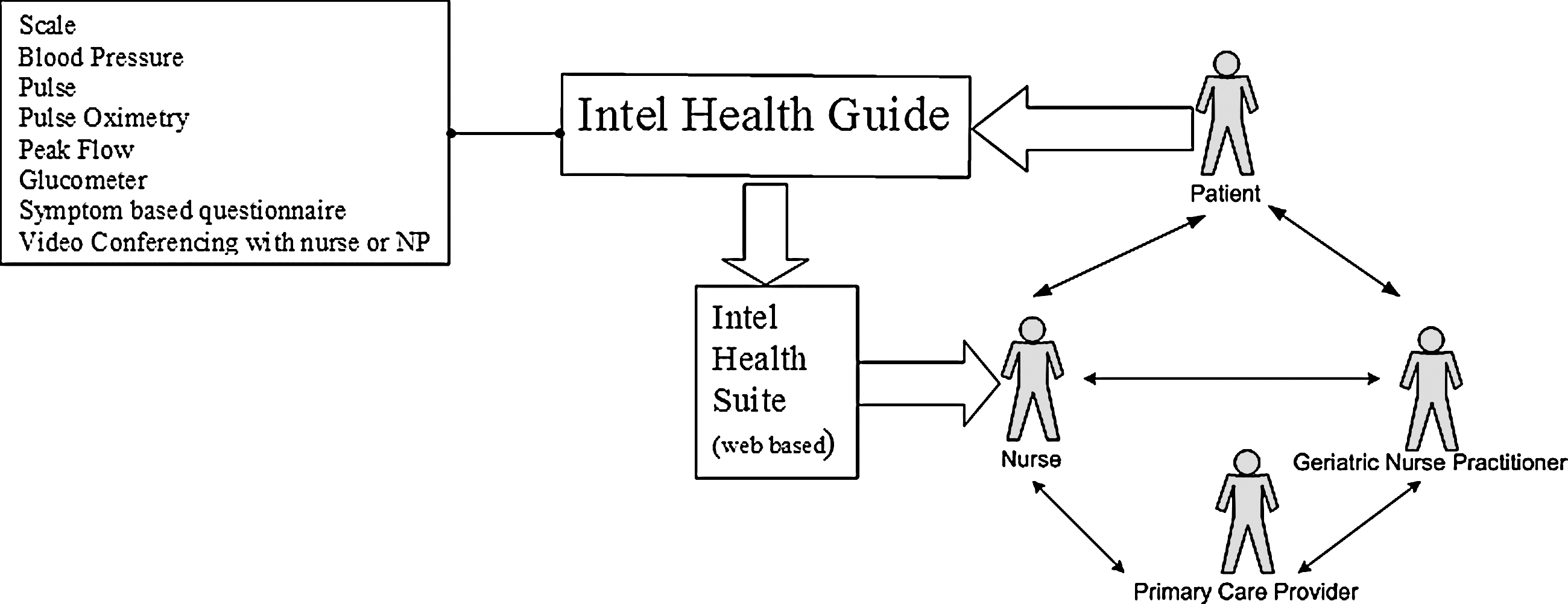
Schematic of daily telemonitoring.
Methods
Study Design
This is a qualitative study using a semi-structured phone survey of patients who had been selected to use a telemonitoring device to record daily health questions and biometric data. All patients were recruited from the Division of Primary Care Internal Medicine and the Department of Family Medicine. All patients gave verbal consent for the study, and HIPAA requirements were waived, as there were no questions pertaining to personal health. The study was reviewed and approved by the Mayo Clinic Institutional Review Board (IRB# 10-005212).
Population
Subjects were more than the age of 60 and resided in Olmsted County, MN. A total of 20 subjects were interviewed. The U.S. Census estimated Olmsted County's population to be 124,277 in 2000. 11
Inclusion Criteria
Subjects should have been enrolled in the telemonitoring study and should have received a telemonitoring device. The subjects should have used the device for at least 8 weeks but not >17 weeks.
Exclusion Criteria
Patients who had not received or used the telemonitoring device were excluded.
Randomization
Subjects were randomly selected for potential enrolment in the study. The study statistician generated a list of randomly selected names, and patients were contacted based on this randomized list.
Interviews
A total of 20 interviews were completed. Participant interviews were conducted by one of the authors (J.C.H.) who had substantial experience in conducting qualitative interviews with medical patients participating in behavioral interventions and was not involved in the participants' clinical care. The semi-structured interview script follows guidelines for minimizing bias and increasing the reliability and validity of interview data. 12 –14 The primary questions used in the qualitative script are presented in Table 1. In addition to the qualitative interview questions, several Likert scale self-report rating items were developed for this study to assess very specific areas of patient opinion about telemonitoring, including use of the monitor for communicating with clinicians, quality of relationship with telemonitoring clinicians, acquisition of new information about medical condition or health management, and perceived burden associated with using the monitor (Table 2 for items). Additionally, patients completed a validated health literacy item 15 and self-reported years of education and comfort with technology. At the beginning of the interview, the participants were encouraged to give honest answers to the interview questions and were reminded that their healthcare professionals would not have access to their responses. Each participant interview was audiotaped and transcribed verbatim.
Questions Included in Qualitative Interview Script
Patient Ratings of Telemonitoring
Data Analysis
Predominant themes (i.e., issues, feelings, or opinions repeated/common across multiple participants) were identified, and a coding strategy was developed. Two investigators with experience in qualitative data analysis (J.C.H. and K.V.D.) independently coded all interviews using methods of content analysis (i.e., systematic process of sorting and coding information based on themes). (Neuendorf 2001, Patton, 1990). QSR's N6 (QSR, Doncaster, Victoria, Australia; Non-numerical Unstructured Data Indexing Searching and Theorizing; N6 2002) qualitative data software analysis program was used to aid in data analysis. Independent coding results were compared, and important themes and representative quotes were identified.
Results
Participant Characteristics
The average age of participants in our study was 81.5±7.1 years. Twelve of the patients studied were women, and eight were men. Nineteen participants were White/non-Hispanic, and one was African American. The average score on the Kokmen Short Test of Mental Status testing was 34.5±2.1 (out of a possible score of 38 and a high likelihood of dementia for scores 29 and below). Overall, patient compliance with the daily monitoring sessions was 89%. Technical problems encountered with monitoring consisted of dropped videoconferencing calls and freezing video associated with 3G connectivity. Table 3 presents patient self-reported health literacy, education, and comfort with technology ratings.
Patient Self-Reported Health Literacy, Education, and Comfort with Technology
Patient Ratings of Telemonitoring
As presented in Table 3, on an average, patients rated their experience with telemonitoring high in terms of communicating with clinicians, quality of relationship with telemonitoring clinicians, and confidence in using the monitor. Hassle associated with using the monitor was rated low, and using the monitor was rated moderately low for learning anything new about medical conditions or taking care of health.
Qualitative Analysis
Telemonitoring increases patient awareness of health
The vast majority of patients reported some increased awareness of their health through the use of telemonitoring. Table 4 presents representative patient quotes reflecting this theme. Patients viewed this increased awareness as helpful, with only one patient suggesting a potentially negative aspect of increased awareness. For this particular patient, increased awareness was somewhat anxiety provoking: Before I was concentrating on not thinking about my symptoms and so I think it has made me more aware, and sometimes that's not real good! I'm kind of a nervous Nellie sometimes (Female, age 82).
Several patients explained that the increased awareness resulting from telemonitoring helped them recognize patterns in their monitored health data and also a connection between their behavior and the resulting health data (e.g., change in blood pressure; Table 4). A few patients described being somewhat surprised by the telemonitoring data. For example, this Female, age 73: The variations in things like blood sugar will vary throughout a day depending on the time of the day. And I always knew that but it's more than I thought.
Primary Theme: The Use of Telemonitoring Increases Patient Awareness of Health
Telemonitoring prompts action
Another predominant theme within the qualitative data is that the patient information collected through telemonitoring can prompt action (Table 5). Although occasionally this action is patient-initiated behavior change (e.g., dietary change), often it is clinician-initiated action (e.g., clinician initiates telephone call to patient, arranges medical appointment). A few patients suggested that the clinician-initiated action motivated them toward a clinic visit sooner than if they were deciding on their own to call in or schedule a visit. One female patient, age 75, explains: The nurses called me and they referred me to my primary physician, otherwise I wouldn't have gone. COPD is terminal and I know I am slipping fast. Otherwise, I would have just suffered through and said this is the way it goes.
Use of Telemonitoring Prompts Action
Telemonitoring provides peace of mind
Several patients describe the positive impact of telemonitoring on what we have termed “peace of mind” (Table 6). This theme captures perceptions of safety, security, less worry, and confidence due to telemonitoring, in general, and more specifically, due to clinician involvement.
Use of Telemonitoring Provides Peace of Mind
Other patient opinions
Although not a prominent theme across interviews, there was some suggestion that the telemonitoring data and associated clinician contact reduced clinic visits and telephone calls for some patients. There was a suggestion that this reduces hassle and is more convenient for patients. Male, age 75: It keeps me from running back and forth to the ER and whenever I start to feel a little queasy, it's about my heart, I take my blood pressure which is so convenient instead of running to the hospital. Female, age 90: I think it (telemonitoring) has lowered my concerns because I feel that I will get help. I don't have to go into the clinic for help. Female, age 66: I don't have to call the clinic all the time. I don't call them at all anymore! I let (telemonitoring nurse) do that.
Patients were asked what they disliked about telemonitoring, and no patients described significant dissatisfaction with the equipment or process. A few patients mentioned that the telemonitoring addresses some of their medical concerns but that other important medical conditions or concerns are not specifically monitored. Female, age 82: It is geared pretty much toward my heart situation and I have other things going on and unless I call the nurse because I want to know more, you know. Male, age 84: I have other problems other than the ones they ask me about on the computer or the telemachine. For instance, I thought I had a little infection on my leg and I didn't. Also, I went over to the clinic because I was having some trouble with my hands and maybe I should have talked to the nurse then. Currently, it just looks at what my current problem is—chronic bronchitis. Male, age 78: The thing about it is if the computer could also monitor my INR, then I could go ahead and adjust my diet on a daily basis.
Patients did not describe excessive difficulty or hassle in using the equipment or process, and a few described ease of use (Female, age 85: “Easy to use. I just do it every day because it's here and easy to use.” Female, age 85: “It isn't a hassle. It only takes 5–6 min time”; Female, age 82: “It's quite clear and simple.” Male, age 85: “It's fast.”)
Discussion
A potential concern with telemonitoring in the elderly population is that the technological aspects of the interaction may fundamentally detract from the perceived patient-provider relationship. Nevertheless, patients in this study rated the quality of their interaction with healthcare providers through the monitoring equipment very high, indicating remote interaction to be a satisfying and positive experience. Ease-of-use of monitoring equipment and the ability to sustain a relationship with their healthcare provider, even when interacting remotely, would be expected to be of paramount importance in influencing acceptance of remote monitoring in the elderly. The patients in our study rated both these qualities very high.
One proposed benefit of home telemonitoring is earlier detection of a decline in health status that would allow intervention at an earlier stage of illness with prevention of severe decompensation and consequent requirement for hospitalization. Patients in our study felt that telemonitoring led to earlier evaluation and intervention than they would have sought on their own initiative.
Possible obstacles to acceptance of telemonitoring in the elderly population include difficulty in equipment operation, a lack of confidence with using the equipment, and/or suboptimal perceived interactions with and difficulty communicating with healthcare personnel through remote monitoring devices. This study was designed to specifically assess these concerns in a group of elderly patients enrolled in the telemonitored arm of the Tele-ERA trial.
Our cohort of patients identified their overall comfort with technology as moderate. However, despite this attitude, they rated their confidence with the telemonitoring equipment as very high, indicating that they did not find using the actual equipment to be overly difficult. The home monitor used in our study has a large, touch-screen interactive display as well as oversized buttons on the monitor designed specifically for the elderly population; these specific features may have contributed to the practical ease of use of the equipment.
Elderly patients often suffer from concordant hearing and vision deficits, making verbal and visual interaction potentially more challenging. Difficulties with communication might be expected to be magnified when using remote monitoring equipment; however, patients in this study rated the monitor as very useful for communicating with their healthcare providers.
Previous studies have found that telemonitoring appears to promote an increase in patient knowledge about their medical conditions 6 ; however, on an average, our patients reported only a moderate increase in their knowledge of their medical conditions. One possible explanation for this is that our study population may have been previously exposed to health information regarding their chronic disease. Additionally, our study design did not include any formal scheduled or routine health education as part of the telemonitoring experience. Patients in our study did indicate, however, that the telemonitoring experience increased their personal awareness of their health status. This increase in attentiveness has the potential to lead to behavioral changes that could affect overall health status.
Other strengths of home telemonitoring identified by our study patients included a sense of comfort in the knowledge that their individual health parameters were being followed closely through telemonitoring. The importance of peace of mind cannot be overlooked in this and other populations. Although difficult to objectively quantify, this increased sense of safety could lead to improved general quality of life. Additionally, when patients feel like they are followed, they may be less likely to seek care in urgent care or in emergency rooms.
Conclusion
Our study found a high degree of acceptance and satisfaction of telemonitoring in elderly patients with chronic disease conditions. This patient population reports a high degree of confidence and only minimal inconvenience with remote monitoring and found that it led to earlier detection and evaluation of changes in their health status than would have occurred without telemonitoring. Telemonitoring improved patients' sense of comfort and safety as well as increased their awareness of their personal health status.
Footnotes
Disclosure Statement
The authors of the study received funding of this study through Intel and GE Healthcare through donations of the Intel Health Guide and support of the device. All authors are employed by Mayo Clinic, who provided the support for this study.