
Abstract
Introduction
Communication technologies are rapidly spreading to the developing world, with the most notable effects seen in the access to mobile phones. 1 Botswana is approaching full mobile phone coverage in all inhabited areas and has 1.49 million mobile phone users, which represents almost 90% of the domestic population. 1 Despite increases in Internet usage over the last decade, only 6% of Batswana have Internet access. 1 This means that even in major city centers, like Gaborone, many healthcare workers continue to have limited Internet access in clinic. Mobile telemedicine allows medical knowledge to reach rural areas of the developing world, where mobile phone coverage extends beyond computer networks.
Currently, the University of Pennsylvania, in partnership with other organizations, has begun to develop a mobile telemedicine network that is rapidly expanding access to telemedicine services in Botswana.
2
This service enables clinicians in more remote regions to submit telemedicine consultations through mobile phones. These clinicians are enthusiastic about being able to connect with and send referrals to specialists; however, they still feel isolated without ready access to the latest medical information and treatment guidelines.
2
In order to meet this need, the following two services were developed: • txt2MEDLINE enables Botswana healthcare workers to query MEDLINE/PubMed and to read abstracts using cellular phones.
3
Depending on the capacity of their personal mobile phone, healthcare workers can use a purely short messaging service (SMS)–based method of query or a more user-friendly JAVA-based interface that transmits data through SMS. • A searchable database of SMS-optimized, clinical guidelines provides practitioners with the ability to search, via text messaging, country-specific treatment guidelines for general medical care, human immunodeficiency virus/tuberculosis (TB) treatment, and the treatment of skin diseases.
Google Text is the only comparable tool available; however, it focuses more on access to general knowledge via text messaging as opposed to specific medical knowledge and literature (
Materials and Methods
An SMS gateway was created using a local server at the University of Botswana. This allows clinicians to send queries and receive results via local (in-country) SMS text messaging on any type of cellular phone (Fig. 1). The search queries are transmitted to the National Library of Medicine (NLM) via the server, and the abstract results are returned to the cellular phone as an abbreviated the bottom line (TBL) summary. The users also have the option to have the full abstract e-mailed to them. Researchers at the NLM had previously developed txt2MEDLINE, a search tool for PubMed that can be accessed using text messaging (Fig. 2, left).
3
For this project, they further developed a JAVA-enabled interface for the PubMed query that is more user friendly and allows mobile phone users to enter the query information into text boxes (Fig. 2, right). They are as follows: 1. medical condition, for example, acute appendicitis 2. intervention, for example, morphine 3. compared with another intervention (optional) 4. outcome (optional), for example, diagnosis 5. select type of publication, for example, randomized control trial 6. send a copy to e-mail (yes/no) 7. limit number of abstracts, for example, two 8. phone number
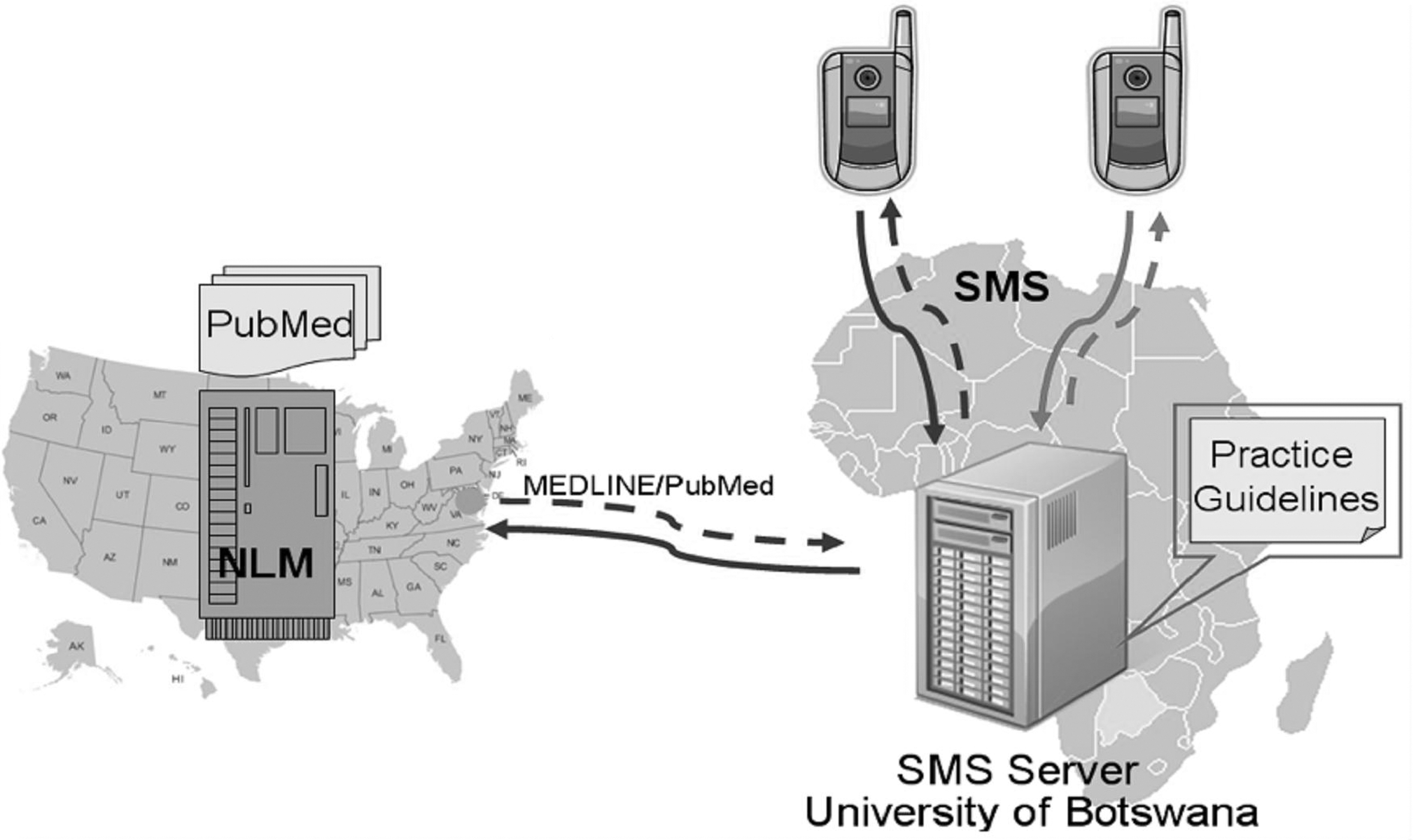
Schematic of the SMS gateway/server established at the University of Botswana. SMS, short messaging service; NLM, National Library of Medicine.

A sample PubMed search using the standard txt2MEDLINE (left) or JAVA-enabled interface (right).
The information entered into the JAVA-enabled interface is then transmitted via text messaging (SMS). The 2007 Botswana Treatment Guide developed by the Ministry of Health National Standing Committee on Drugs was also converted into a format that can be queried by SMS. When possible, the response to treatment queries was limited to 300 characters, the equivalent of two text messages.
Faculty at the University of Botswana Medical School recruited medical students, internal medicine and pediatric residents, doctors in the community, and researchers from the university to participate in evaluating the project after full disclosure. All healthcare workers in the medical community were eligible for this study. People who did not have a cellular phone were not able to participate. Participation was completely voluntary. The only benefit of participating was access to this new service.
The participants were placed into focus groups and were introduced to and trained to use txt2MEDLINE and the SMS-optimized Botswana Clinical Guidelines on their mobile phones. Focus groups were led by our Mobile Telemedicine Programs Manager (R.L.Q.), who is an expert in mobile technology and therefore able to troubleshoot any problems as they arose. At the end of the training session, each participant completed a survey that consisted of multiple choice and open-ended questions. The survey assessed the need and desire to query PubMed and Botswana National Treatment Guidelines using cellular phones. All participants were trained to query PubMed using SMS text messaging either through standard messaging platform or via a JAVA-enabled user-friendly platform. Then, each participant chose one of the two methods of submitting queries, depending on the capability of their cellular phones.
In the next phase, participants were given 4 weeks to test these two new services in the field. The usefulness of these resources was evaluated objectively by tracking and logging access to txt2MEDLINE and the Botswana Clinical Guidelines. The frequency, the time when searches were conducted, and topics that were searched were tracked. At the end of the 4 weeks, users were contacted to elicit informal feedback regarding their use of the technology and suggestions for improvement. This subjective evaluation of service utility will enable us to refine and tailor the technology to the users for which it is intended.
Results
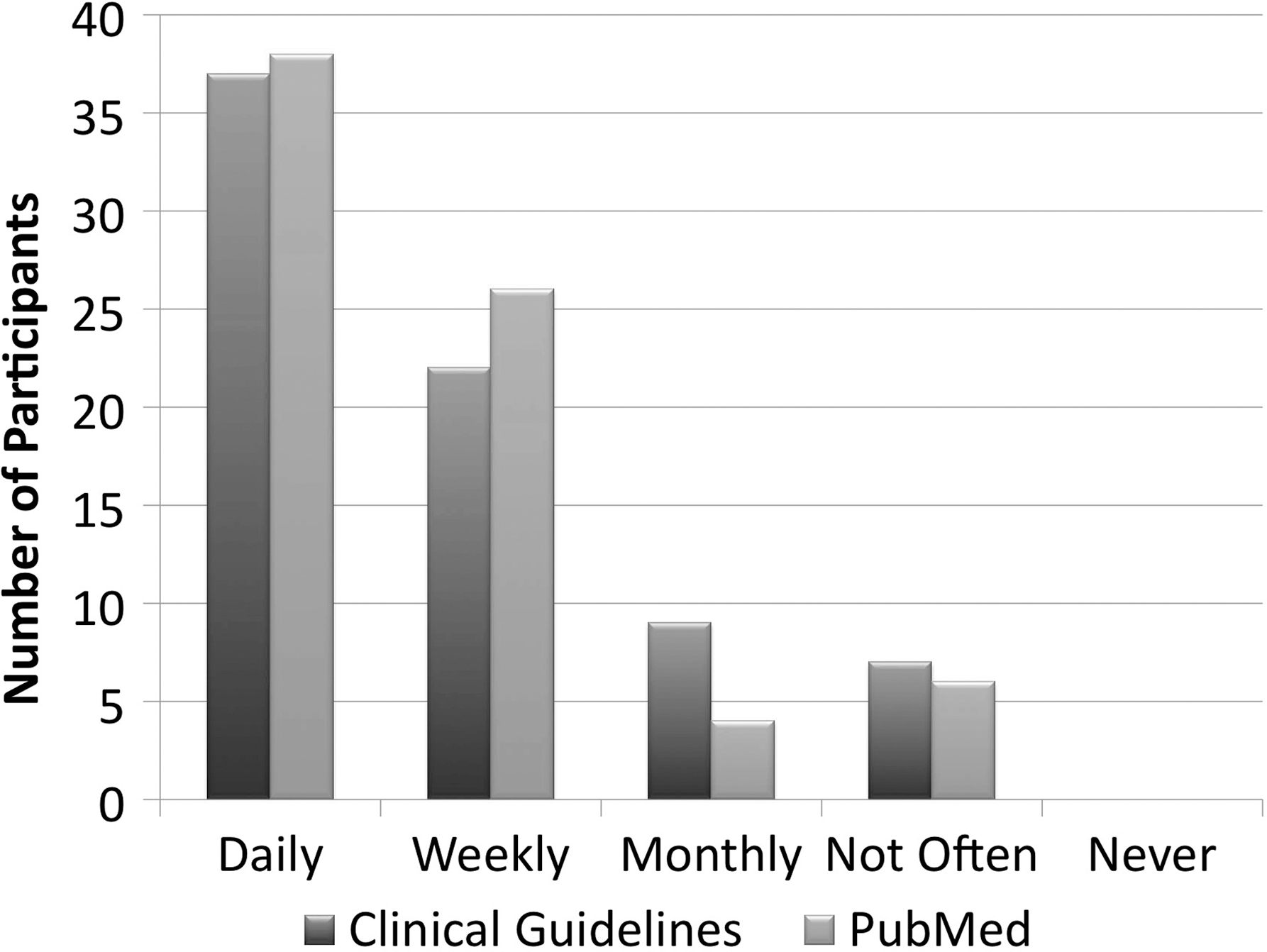
In total, 81 individuals attended one of the four focus groups held in Gaborone, Bobonong, Maun, and Francistown. Participants included 20 doctors, 18 nurses, 17 medical students, 10 professors of medicine, 7 residents, 2 medical officers, 1 dietician, and 6 other healthcare workers. Of those 81 participants, only 76 individuals completed the survey. Eighty-six percent of participants spend the majority of their time providing patient care, and 53% were familiar with PubMed. The majority of participants (83%) reported using text messaging daily for general communication. Approximately half of the participants have access to the Internet in clinic, though some commented that it was often slow and unreliable. Forty percent have no access. Of those familiar with PubMed, 59% said they did not use PubMed often (≤monthly) (Fig. 3). Only one participant had a mobile phone capable of loading the user-friendly JAVA-enabled interface. All other participants used SMS to access txt2MEDLINE and SMS-optimized clinical guidelines.

Current frequency of PubMed use among participants familiar with the search engine.
Perceived Use of txt2MEDLINE and SMS-Optimized Clinical Guidelines
During the initial training session, most participants said they would use the services daily or weekly, 86% and 79% for txt2MEDLINE and SMS-optimized clinical guidelines, respectively. Participants thought that access to both txt2MEDLINE and SMS-optimized clinical guidelines would be equally helpful (Fig. 4).
Perceived utility of txt2MEDLINE and SMS-optimized clinical guidelines.
Actual Use of txt2MEDLINE and SMS-Optimized Clinical Guidelines
In the 4-week trial period, participants only used the services for the first few days after training, and then only sporadically after that. Feedback included the following criticisms: • It was difficult to remember the commands (e.g., users enter “S?” before searching a term) needed to run searches using phones that were not JAVA enabled. Most users did not have JAVA-enabled phones. • Abbreviations make TBLs difficult to read. • The clinical guidelines require exact search term as indicated in the SMS-enabled guidelines, or else an answer is not returned.
Although participants only briefly used the service and several criticisms were given, some positive feedback was also received. Participants embraced the idea of being able to access medical information using cellular phones, particularly if the platform was easier to use. All participants had their own phones and were willing to use them to access updated medical literature and clinical guidelines, particularly because this type of information is not readily available at the point of care.
Discussion
Cost and Penetration
In Botswana, broadband Internet continues to be expensive (11.54% of monthly GNI per capita in 2009) and inconsistent. It is rarely available in hospitals or medical clinics. Mobile phone coverage is much more affordable and penetration approaches 100%. 1 The SMS gateway at the University of Botswana allows users to access the PubMed/MEDLINE database via local text messages, avoiding the costs of international text messages or Internet usage. The majority of participants had prepaid plans that charge 0.25 Pula or $0.04 cent/sent text message. There is no charge for receiving text messages.
Tele-Education
Sub-Saharan Africa confronts many challenges including poverty, a disproportionate burden of disease, and a shortage of skilled human resources. Botswana has 40 physicians per 100,000 populations, compared to 230 and 160 physicians per 100,000 populations in the United States and Canada, respectively. 5 This direct comparison highlights the extent of under servicing that exists in Botswana. The future remains hopeful as Botswana opened the doors of its first medical school in August 2009 at the University of Botswana, in Gaborone. The university will train at least 50 new doctors each year; however, many of these new doctors will be practicing in remote areas of Botswana, where access to information is even more difficult. Mobile telemedicine can help build capacity using information and communication technologies for continuing professional development. 6 These students and young doctors can also learn evidence-based medicine and have a point-of-care tool through the use of txt2MEDLINE and SMS-based clinical guidelines.
In addition, medical practitioners tend to live in urban areas whereas 60% of Africa's population is rural. 5 Telemedicine offers the potential to overcome this misdistribution and improves access to scarce medical specialists.
Lessons Learned
This project has uncovered key issues in design that prevent the current adoption of these services. Currently, the technology is being modified by the NLM to solve these problems. The TBL abbreviations will be discarded, and the abstract summaries will be more easily readable. Partial term searching now allows users to retrieve results regardless of whether the full term is input. For example, searching “candida,” which is not an exact search term, will now return “Esophageal Candida Adult.” The result of the partial search term will always default to the adult guideline unless the word “child” is included in the partial search term. Software will be developed for the SMS-enabled clinical guidelines that allow queries to return the closest search results regardless of whether or not the exact term is input.
Coexisting programs at the University of Botswana will result in more medical students and residents having access to a JAVA-enabled phone. This will eliminate the problem of difficult-to-remember commands in a population who would be well served by these applications. The initial enthusiasm of participants and perceived use suggests that once these improvements are made, the technology will be more widely adopted.
The NLM only controls the abstracts, provided by the publishers themselves. The full text papers remain with the journal publishers. Therefore, users with an individual or university subscription can access the full journal article of interest online. Users without subscriptions are unable to do so. This is one limitation of the service.
In the future, researchers will concentrate on retraining individuals in the district hospitals on the updated, more user-friendly clinical guidelines. This updated version does not require the input of any commands. A user simply sends a text message containing the disease of interest (e.g., TB) to the clinical guideline phone number provided. In return, the user receives the Botswana-specific treatment standard for that disease. During this process, the participants will be resurveyed to evaluate whether the change in format has increased the usefulness of the application and the use of this service will be tracked by the NLM.
Conclusions
Accessing clinical guidelines and PubMed/MEDLINE queries via text messaging represents an optimal method of evidence-based knowledge communication in countries where mobile phone coverage surpasses PC-based computer networks. Most surveyed healthcare workers in this study had previously used PubMed as a clinical tool whenever they could access the Internet; however, many had no Internet access or experienced unreliable Internet connections at the point of care, which prevented them from accessing current medical literature and guidelines.
This service fulfills an unmet need for clinicians in developing countries, and will prove advantageous in other populations with similar circumstances of limited Internet access in clinics, and already have widespread adoption and familiarity with text messaging. This program strives to improve medical care in resource-limited and remote settings by providing clinicians with convenient access to evidence-based medicine during clinical practice.
Footnotes
Acknowledgments
The authors would like to thank Click Diagnostics for their assistance in creating the mobile phone JAVA application. The authors would like to thank the University of Botswana Information Technology group for their help in setting up the server. The authors are also appreciative of the SIM card donation from Orange Botswana.
Disclosure Statement
No competing financial interests exist.