
Abstract
China has been implementing regional collaborative medical service (also known as e-health) for >5 years, but is still facing the challenges of bridging different community health information systems (CHISs). The fact that different communities have different systems makes it difficult to share information and data between different CHISs. To explore a solution for addressing this problem, we constructed a demonstration CHIS in Beijing's Dongcheng District. This system is based on the Software-as-a-Service model, in which a central data center is used to store users' health records and to provide different services. This system provides a comprehensive platform combining disease prevention, health protection, medical care, rehabilitation, health education, and family planning. In this article, we first show the challenge of implementing e-health–oriented CHIS in China, then we briefly introduce our solution, and finally we share our experience learned from the modern CHIS implementation practice.
Introduction
In the practice of implementing a regional collaborative medical service (RCMS), we found particular difficulty in conducting medical information sharing for communities, because different communities have different health information systems. To conquer the problems brought by the heterogeneity of these systems, we have constructed a community health system based on the Software-as-a-Service (SaaS) model. 1 SaaS, an innovative software application model that began to emerge in the 21st century, uses the latest trends of the scientific and technological development of software. In the past, because of the restraints of the network bandwidth and communications technology, SaaS model could only be adopted by the kind of applications with lower requirements on bandwidth and data security. Nevertheless, with the rapid development of the Internet and the continuous improvement of the network bandwidth, SaaS model has begun to penetrate various fields, including medical system informationization and regional medical information sharing. 2
To meet the requirement that “everyone enjoys basic medical care service” put forward in China's New Medical Reform, 3 we need to establish a health model that combines disease prevention, health protection, medical care, rehabilitation, health education, and family planning. 4,5 To actually realize a people-oriented community health management and set up life-long health records for residents, 6 we have to construct a comprehensive community public health management model that serves individuals, families, groups, and districts in a point-to-area manner.
The community health information system (CHIS) studied in this article covers a permanent population of near 600,000 in 126 communities distributed in 10 streets. It realizes full-time and full-process supervision of the medical operation work flow and precise health management and service for the residents. This mode provides an economical, practical, reliable means for exchanging medical information and to improve the CHIS in RCMS. In this article, we will first analyze the demands and challenges of implementing RCMS-oriented CHIS from the perspective of RCMS and then show what we learned from our practice.
Demands and Challenges
The original intention to construct the CHIS is for the convenience of patients, including patients' easy access to medical treatment, convenient follow-up tracking, and rehabilitation guidance. Its intention is also for supervisors' convenient management and supervision and for effective maternity and child care. The specific demands on the CHIS could be divided into the following four categories. 7
Demands
Convenience to patients
The system should provide health cards for residents and provide them with a convenient, rapid medical service through the health cards. Health cards in one community can be recognized by other communities within the platform, and thus, a card holder could have medical treatment at any community health service stations within the platform. 8 The system has a unified control on medication to guarantee unified pharmacy resupply and no difference in pharmacy price among different community health service agencies within it. Further, the system must establish a two-way referral mechanism between community health service agencies and hospitals to realize sharing of information and resources between communities and hospitals. 9
Management and supervision
The system needs to set up a resident health records management system to collect and manage the information and resources on the health activities of residents throughout their life cycle. Based on the data mining of the information in health records, the system must be able to effectively reallocate and sort out the resources collected and create a dynamic diagram to reflect the basic health conditions of residents. It should support patients to make comment on the professional skills and service quality of the community service personnel (including general practitioners, general nurses, and practitioners for psychological consultation), enabling relevant supervision departments to analyze data with instruments provided by the system and obtain the performance appraisal results. Additionally, the system must support the collection, analyses, and report forms of clinic visit data and effectively monitor communicable disease and infectious disease of people in the same group. 10
Tracking and guidance
The system should provide general practitioners with a comprehensive management platform that is concerned with five kinds of chronic disease (malignancy, hypertension, diabetes, coronary heart disease, and cerebrovascular disorder) and should establish special case information for chronic patients in accordance with the kind of disease and draw up appropriate rehabilitation plans for them. The system must be able to make an objective evaluation of the disease of patients and determine the managerial class through a series of quantization tables, based on formulating visit plans and achieving full-process supervision of the rehabilitation of chronic patients. Further, the system ought to provide general practitioners with a management platform oriented toward the rehabilitation services for the disabled, which will help general practitioners conduct comprehensive management of the location and rehabilitation of the disabled in their responsible area. 11,12
Maternity and child care
The system must provide women of child-bearing age in the community with child-bearing health and care guidance, draw up prenatal period health plans, make commonly encountered disease screening for newborns, formulate debility child management plans based on the screening results, and take charge of immunization and vaccine management for newborns. 13,14
However, it is not easy to build a system that meets all these requirements.
Challenges
Lack of standard
The government did not realize the importance of making standards for the medical information systems and regulation of the vendors. So different vendors developed different systems and sold them to different communities. These companies did not sit down together to define the data format and make standards for the interfaces of their systems. Consequently, these systems could not communicate with each other at all.
Low data correlation
The goal of community health record is to improve the continuity and interaction of community health service. Community and community health service have to communicate to better conduct community diagnosis. This is not possible if those CHISs do not have a common data format and communication protocol. In currently bad cases, lots of CHISs even do not support importing their clinical data to their system, not to mention importing from or exporting to other systems. 15
Poor functionalities of the CHIS
Initially, these CHISs were only designed to replace the paper-based systems. The system vendors only focused on the business processing and assured the system stability. The vendors failed to think about the new opportunities introduced by those information systems, which cannot be achieved by paper-based systems, such as remote health monitoring, intercommunity information viewing/storing, and remote diagnosis.
Infrastructure construction lag
Besides computer hardware, software, and network, infrastructure construction also includes others such as law and policy and human resources (engineers, administrators, etc.). Although computer hardware, software, and network infrastructures have been greatly improved in these years because of the economic boost of China, the law and policy for medical information systems still greatly lag behind.
Our Solution
Based on the SaaS model, this system has one data center, and end users can access this data center from any terminal linked to the data center (Fig. 1). Most data are stored in the central database, including health records of residents, examination and appraisal information on medical staff, pharmacy resupply information, registration information of the disabled, etc. Doctors can log in the system at any place where a network connection to central server exists. After logging in, the clients dynamically load the desired modules, which are only stored in the server, and run them on the browser without any other preinstalled software.
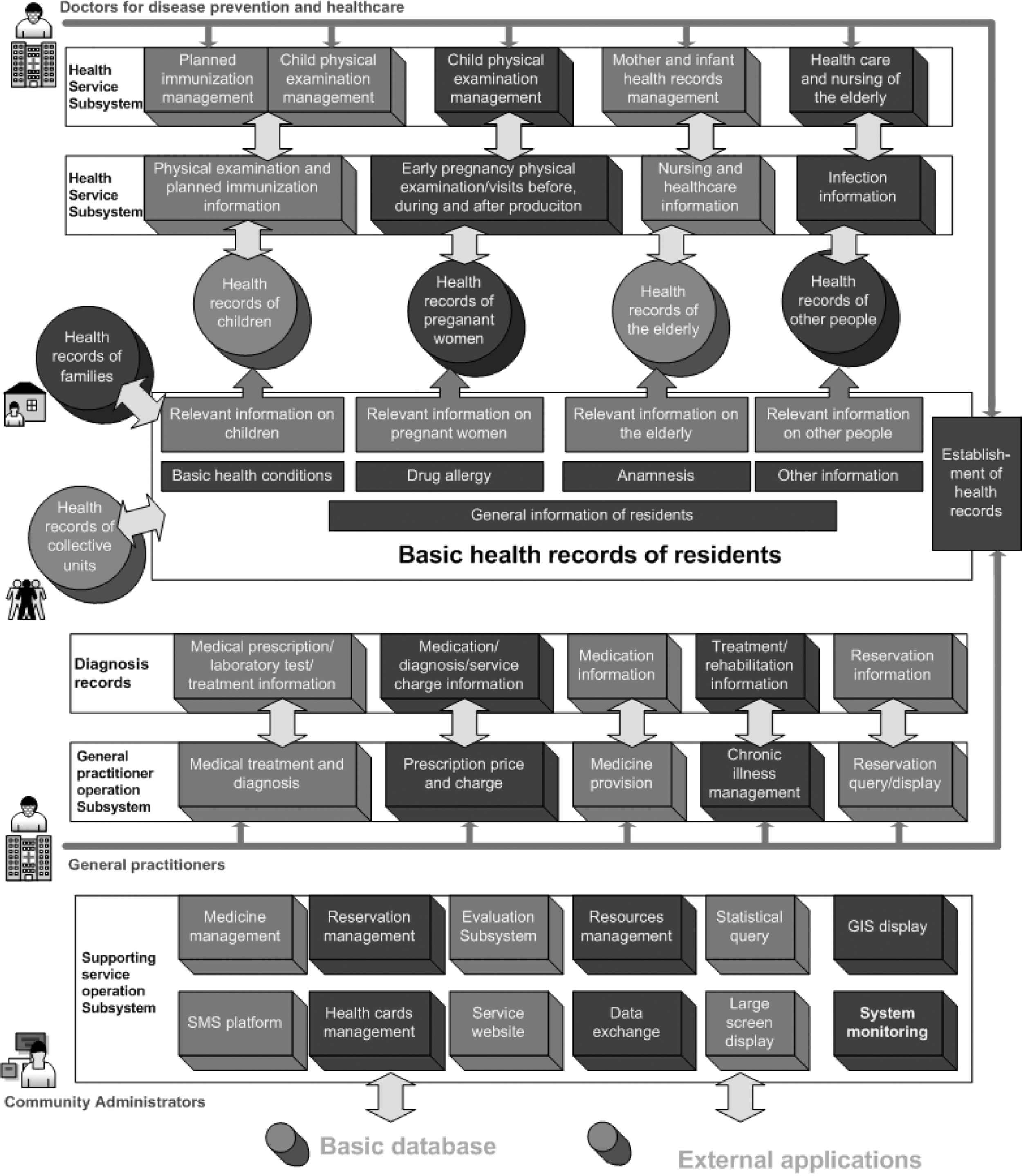
System architecture.
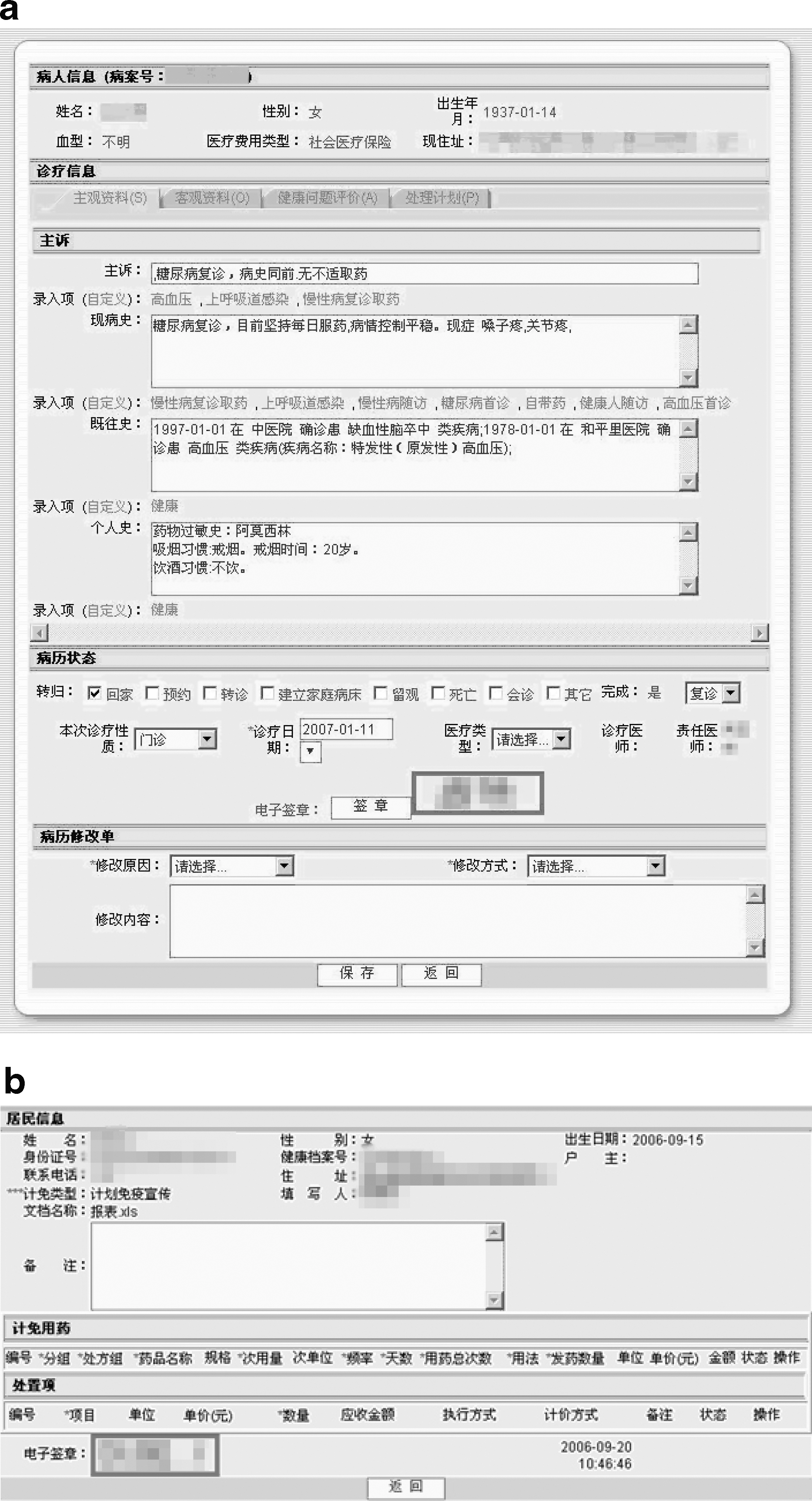
Health records of residents include their diagnosis records, that is, their electronic medical records, which serve as the core of system's database, as residents' health records bridge different kinds of operation and service systems. The data layer of the system is completely transparent to users, and users do not have to worry about whether the data are stored in the local servers or in a remote database. See Figure 2a to find a sample of the electronic health record.
Asnapshot of the system.
The service layer includes data service, operation service, security service, public health service, integration service, management service, operating environment service, subscription service, and information service. The information service and protocols make up the communication bus and the other parts constituting the general service. The general service and communication bus could be used to connect both internal operation applications and external operation applications.
The community health service information platform center stores the health records of residents, which accompany them for their whole lives. Both the general practitioner operation system and the healthcare system improve and expand the information on residents' health records through diagnosis records and healthcare information, establish relations between health records based on the information association on these records, monitor residents' health conditions through statistical analysis of the information on health records, and carry out supervision of the health service in the community. Other supporting service systems are for the purpose of maintaining and managing health records in a better manner and guaranteeing better running of the operation system. The following is the system architecture.
The overall community health service information system includes the health records management subsystem, general practitioner operation subsystem, disease prevention and healthcare operation subsystem, planned immunization operation subsystem, health education subsystem, medicine dispatching operation subsystem, evaluation and appraisal subsystem, and community health service management subsystem. See Fig. 2b to find a sample of Expanded Programme on Immunization (EPI) record.
Health Records Management Subsystem
This subsystem manages the basic health records, medical service information, and healthcare information of residents. The basic health records involve the general information, basic health conditions, anamnesis, allergic history, and health behavior. The medical service information includes the chronic illness management situation and diagnosis records. Healthcare information mainly refers to the healthcare process information of different groups of people.
General Practitioner Operation Subsystem
This subsystem is mainly responsible for the establishment of resident health records, completion of the input of medical treatment information, chronic management and referral service information, assumption of follow-up visits, traveling medical treatment, appointment and visit, rehabilitation management, charging and other tasks, and realization of doctor advice opening and implementation as well as relevant auxiliary functions.
Planned Immunization Operation Subsystem
This subsystem comprises vaccine management, vaccine inoculation management, collective unit management, and other functional modules. This mainly achieves unified vaccine control and dispatching and hierarchy management of the three kinds of vaccine inoculation groups: children, adults, and collective units.
Health Education Operation Subsystem
This subsytem is made up of health education plan management, leading group lists management, network service agency management, health education work registration management, and other modules.
Medicine Dispatching Subsystem
This subsystem includes warehouse entry management, delivery management, pricing management, inventory management, random medicine inspection, and other modules.
Evaluation and Appraisal Subsystem
This subsystem helps the management personnel of the community health service management center evaluate and appraise clinics, community health service stations, general practitioners, nurses, doctors for disease prevention and healthcare, doctors for mental illness prevention, and hospitals in the governed area. The system generates objective evaluation in accordance with different kinds of records through the internal evaluation system and in terms of the external appraisal system. The quality control personnel of the community health service management center can check the appraisal results at regular and irregular intervals. The final results are a combination of the internal evaluation and external appraisal.
Community Health Service Management Subsystem
This subsystem mainly comprises personnel management, organization management, comprehensive statistics, commanding and dispatching, and other modules. It provides comprehensive management of the community health service in the whole district with effective supports and helps.
Statistical Analysis Subsystem
This subsystem mainly involves the collection and analysis of evaluation and appraisal information, community health service quality information, and in-station medicine and consumptive material management information.
Results
Based on the SaaS model, this article considers the Beijing Dongcheng District Community Health Service Management Information System, which covers all residents in the district from various aspects. It also puts forward the assumption on reform in eight fields, including construction of a community health service platform through informationization network, restoration service and management process, and establishment of a supervision and an evaluation system. This system covers a 580,000 permanent population in 126 communities on 10 streets and realizes full-time and full-process supervision of the work flow and precise management and service for the health of residents.
The SaaS model provides the medical personnel with great convenience in their employment of this system. For example, as the system can be assessed at multiple points, when a doctor visits his patients, he can inquire and input the patient's health information through his laptop, which facilitates doctors for medical treatment and consultation of many inconvenienced patients.
Additionally, adoption of the SaaS model makes all service data stored in a central database, resolving the problem of the sharing and exchange of medical data. As the data of different community health service agencies are stored in the same place, access to data generated by other agencies is as simple as access to data of the local agency. Only with some operations at the service and access control layers, data sharing can be realized among different community health service agencies. Further, as storage of data from various communities is in one data center, unified control and backup provide great convenience to share regional information between community health information platforms and large hospitals. When a patient needs to carry out a referral between a community health service agency and a large hospital, exchange of his health record could be also easily achieved.
Experience
Standard is the Key
The major factor blocking the communication between communities and communities is lack of standard. A standard for data storing and communication interface should be developed before the vendors step into developing their systems. All products should be compatible with the same standard; otherwise, the product should not be used by any communities.
Government and Business Cooperation
Standard is critical, but is also difficult to be made. System vendors tend to promote their system as standard, so the government should play the role as standard committee, because government is the market regulator.
Privacy Protection is Difficult but very Important
One factor that slows down the process of e-health is that users are afraid of privacy leak under “open” systems. To make this system accepted by people, a strong access control system should be developed for protecting users' data so that it will not be easily accessed and even modified. All records stored in the data center cannot be deleted. In other words, modifying a record actually creates a revision of the record, and all revisions of this record are kept so the modification chain can be traced in anytime.
Legislation and Policy Should Be Discussed as Early as Possible, or they Will Lag the Process
Although developed by engineers, this kind of systems will not be popularized until the legal professionals participate and produce some results. Legislation usually means a long process, so a timely policy is very important for doing research or conducting some demonstration projects, such as the case in this article.
Conclusions
This article puts forward a solution to construct an RCMS-oriented community health information management system and introduce the demonstration project in Dongcheng District, Beijing. Analysis of the experimental results demonstrates that this system brings more convenience to medical personnel, patients, and health administration and supervision departments. This system facilitates information sharing among different medical agencies, helps realizing regional collaborative healthcare, and thus, deserves to be promoted and popularized in more places for its practical guidance value. This system serves an economical, practical, reliable framework to enhance the CHIS in the informationization construction of RCMS and complies with the requirement that “everyone enjoys basic medical care service” put forward in the “New Medical Reform.”
Footnotes
Acknowledgments
The work described in this article has been funded by National Key Science and Technology R&D Program in the 11th Five-Year Plan of China (2006BAH02A28) and Beijing Natural Science Foundation of China (4083037); it has been supported by the Information Office and Health Bureau of the Government of Dongcheng District, Beijing, and Sinosoft Co., Ltd.
Disclosure Statement
No competing financial interests exist.