
Abstract
Introduction
The use of technology is increasing in nearly every field, and medicine is no exception. Telemedicine as a means of remote patient–physician interaction is growing. 1 This technology may improve patient access to care. 2 Telemedicine is being used in a variety of medical arenas, including psychiatric counseling, 3,4 home healthcare services, 5,6 intensive care units (ICUs), 7 and emergency stroke care. 8
Access to specialists who are limited in number may be a particularly valuable benefit of telemedicine. Joint teleconsultation with the general practitioner, specialist, and patient have recently become popular. Virtual consultations with specialists can eliminate “duplication of investigations and treatments.” 9 Overall cost for the patient or the provider may be greater or lower with the use of teleconsultations; however, all potential benefits of telemedicine should be considered, including patient satisfaction, efficiency, and timeliness of care. Joint teleconsultations with a general practitioner and specialist have produced higher patient satisfaction and increased the likelihood of follow-up care. 9,10
Telemedicine is also being used in follow-up care. Morgan et al. provided parents of children diagnosed with severe congenital heart disease with either home videoconferencing capabilities or telephone follow-up calls as a means to communicate with their physician postdischarge. All families provided with videoconferencing found it beneficial. 2 Salvador et al. showed that general practitioners can access home coagulometer INR results via electronic record to monitor Warfarin dose without requiring frequent visits to healthcare centers. 5
Rural communities may lack the most advanced technology or the specialists necessary in emergency situations. For example, rural hospitals in northern Ontario use videoconferencing between their referring physician and a neurologist at a specialized care center to aid in assessing patients' neurological symptoms in the setting of an acute stroke. 8 Telemedicine is also useful in ICU settings by enabling an intensivist, a critical care nurse, and a clerical person to round on patients and make critical decisions via an eICU equipped with bedside monitors and microphones. 7
Applications of Telehealth in Sleep Medicine
Obstructive sleep apnea (OSA) is “a condition characterized by repetitive obstructions of the upper airway often resulting in oxygen desaturation and arousals from sleep.” 11 Typical symptoms of OSA include snoring, restless sleep, and daytime sleepiness or fatigue. 12 Approximately 9% of women and 24% of men have undiagnosed moderately severe sleep-disordered breathing. 13 OSA has been associated with numerous cardiovascular complications including coronary heart disease, heart failure, hypertension, and stroke. 14 Predisposing factors for OSA include obesity, male gender, nasal obstruction, endocrine abnormalities, craniofacial abnormalities, and familial history.
OSA can be diagnosed using nocturnal polysomnography (PSG) in a sleep laboratory, home PSG, or more limited portable monitors. 15,16 Full PSGs are very expensive, whereas portable monitors can be more economical. The American Academy of Sleep Medicine recommends that portable monitors may be used in a lab or in a patient's home under strict guidelines, but that an in-laboratory PSG is the preferred option for most patients. 16
There are four main treatments for OSA: continuous positive airway pressure (CPAP), weight loss, oral appliances, and surgery. 17 –19 CPAP is the most widely accepted form of treatment; however, maximizing adherence is one of the most important challenges sleep specialists face. 17,20
OSA is under diagnosed. 13 The relatively limited supply of sleep specialists is likely to be a continued barrier to diagnosis. Telemedicine may be a very efficient way to allow greater access to care.
Telemedicine has been extensively used in the field of sleep medicine. Specifically, telemedicine can be used to transfer polysomnograms online from remote sites to larger facilities equipped with specialists capable of study interpretation. Kristo et al. reported that this is not only feasible but can even be cost-effective. 21 At-home sleep studies can be effectively conducted via home monitoring systems, eliminating the need for overnight sleep studies at a facility. Such studies can be conducted in real time or with portable monitoring that is later downloaded for interpretation. Sleep studies in real time can use video technology to connect the patient to a sleep technologist. 22
Additionally, telemedicine can be used to improve CPAP adherence. Smith et al. conducted a study in which telehealth units allowed nurses to view and educate patients in their homes. This study showed how a structured system of telecommunication with patients improved CPAP compliance. 6
To have sustainable telemedicine programs, there must be acceptance and understanding among patients and caregivers. Users must believe that telemedicine is useful and adds value to their medical care. 23 The study by Swinton et al. found that primary care physicians and patients alike expressed belief that telehealth is “an acceptable solution to the access to care problem in the treatment of depression in rural communities.” 24 Timmerberg et al. conducted a pilot study in which dieticians counseled diabetic patients via videoconference. Results showed patients were equally satisfied with counseling via videoconference and in person. Patients said they were comfortable talking via videoconference, found the lack of physical contact acceptable, generally found the encounter convenient, and had a satisfaction rating of 4.6 out of 5. 25 A second study using videoconferencing showed that 96% of psychiatric patients were comfortable communicating with an off-site clinician. In addition, a majority of the patients stated they would participate in videoconferencing again. 26
Although telemedicine has been explored in various ways, few studies have been conducted that use direct physician–patient videoconferencing in sleep medicine. This study was designed to compare the effectiveness of videoconferencing versus in-person interactions in sleep medicine with respect to patient satisfaction and sleep apnea treatment adherence. Patient satisfaction and adherence among sleep patients may differ from other fields, possibly because sleep visits are fairly history intensive and less dependent on physical examination, although examination is an essential component of the visit. If these two factors are similar between the two groups, sleep specialist physicians may be encouraged to apply telemedicine to increase patient access to specialty care.
Materials and Methods
The Illinois Neurological Institute (INI) Sleep Center has two locations, one in Peoria, IL, and one in Morton, IL. At both locations the patient is first seen by a nurse practitioner (NP) to obtain initial history, conduct a physical examination, and enter this information and an initial impression and plan in the electronic medical record (EMR). The patient is then seen by a sleep physician, either in person or by videoconference. If the patient is at the Morton center and the sleep physician is at the Peoria center at that time, the NP calls the sleep physician in Peoria by telephone to present and discuss the patient. During that conversation, the sleep physician reviews the information entered into the EMR and makes changes based on the discussion with the NP if appropriate. The Polycom communication system is activated, which allows for videoconferencing between the patient in Morton and the physician in Peoria. The patient and physician hear and see one another in real time. The physician reviews the history and examination, discusses the assessment and plan with the patient, and provides patient education, making appropriate changes to the EMR as indicated based on the videoconference interaction.
Patient Satisfaction
A prospective survey analysis determined patient satisfaction. A patient satisfaction survey developed by the US Department of Health and Human Services Health Resources and Services Administration was administered to all new patients upon check out from the INI Sleep Center–Morton (Sleep Center).
The survey included three specific questions that pertained to satisfaction with the “Provider”: • Listens to you • Takes enough time with you • Explains what you want to know
Each question was scored on a scale from 1 (lowest) to 5 (highest). The total patient satisfaction with provider score is the sum of the three questions regarding the provider, with a maximum score of 15. Inclusion criteria for the study include subjects ≥18 years of age at initial visit who were new patients at the Sleep Center and able to complete the survey. Exclusion criteria for the study include patients who were seen only by an NP and not the sleep specialist physician. Statistical analysis was performed using SAS 9.2 software.
Treatment Adherence
Treatment adherence was investigated with a retrospective cohort study comparing the CPAP adherence of patients seen by the sleep physician via videoconference to patients seen by the sleep physician in person. The retrospective chart review identified adult subjects seen at the Sleep Center between November 2007 and September 2009 using the patient database available at the sleep center. Inclusion criteria for the study include subjects ≥18 years of age at the initial visit subsequently diagnosed with OSA and prescribed CPAP. Exclusion criteria for the study include subjects who use CPAP brands other than ResMed (only one CPAP brand was selected for uniformity of reported adherence data) and those patients who were seen only by an NP and not the sleep specialist physician.
Subjects were divided into two groups: those who met the physician at their initial visit via videoconference and those who met the physician in person. Two variables were used to analyze CPAP adherence: percentage of nights CPAP was used for ≥4 h and the average number of minutes CPAP was used per night. The Mann–Whitney t-test was used to compare CPAP adherence between the groups over the most recent 14 consecutive days available. Statistical analysis was conducted using SAS 9.2 software.
Results
Patient Satisfaction
Surveys were collected from 98 subjects from July 2009 to March 2010. Eight subjects were excluded: three did not complete the question regarding whether they met the physician in person or via video, two did not see a physician, two did not answer the questions regarding provider satisfaction, and one was <18 years of age.
Ultimately, 90 surveys were analyzed (56 subjects seen in person; 34 subjects seen via videoconference). The two groups were similar in gender, age, and ethnicity. Descriptive statistics are provided in Table 1.
Descriptive Statistics—Patient Satisfaction
The mean patient satisfaction scores of the two groups were analyzed using a Mann–Whitney test. The null hypothesis states that the means of the two groups are the same, whereas the alternative hypothesis states that the two groups are different. The null hypothesis was not rejected. Therefore, there is no difference between groups. Results are displayed in Table 2 and Figure 1.
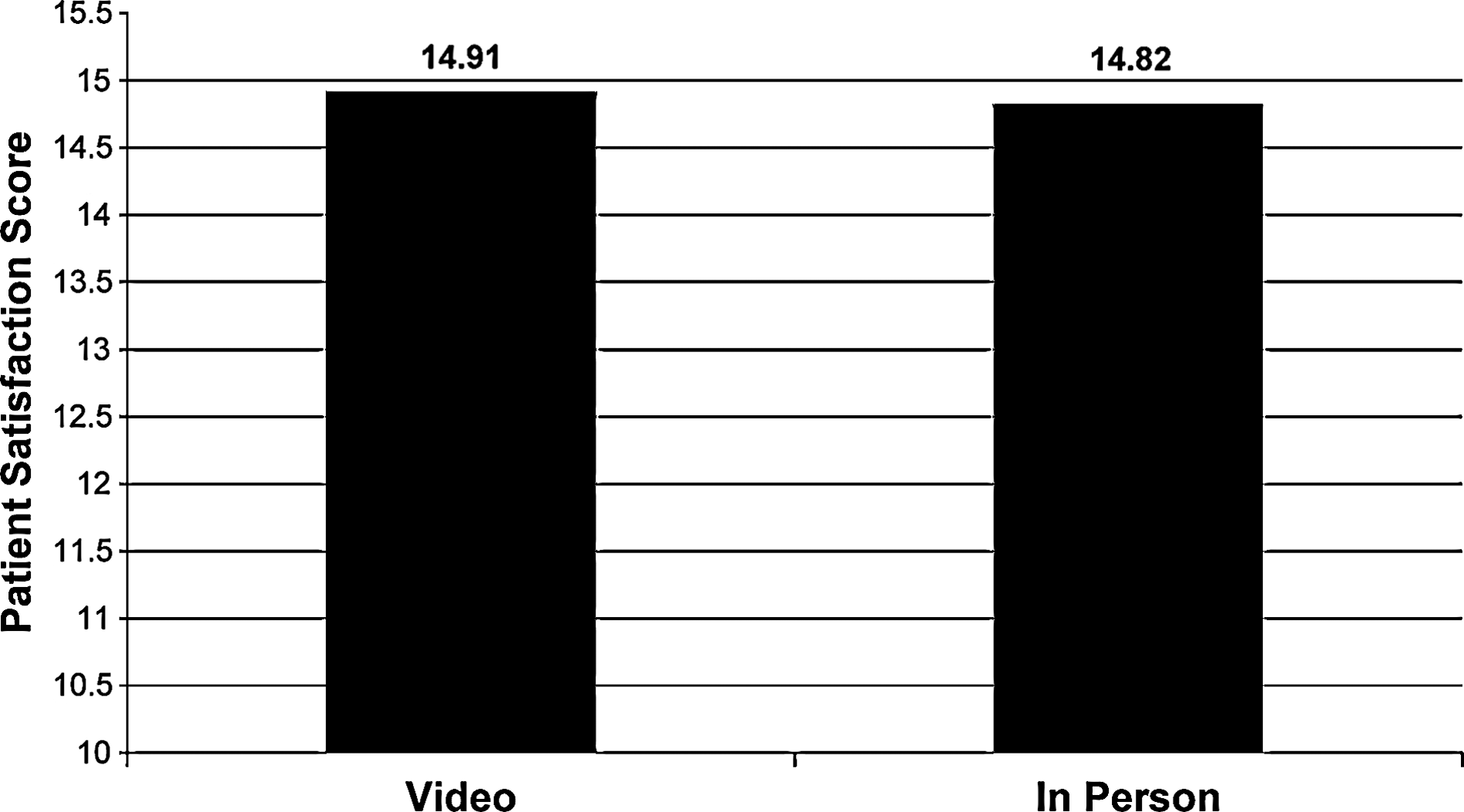
Patient satisfaction score comparison.
Mann–Whitney Test—Patient Satisfaction
Treatment Adherence
Between November 2007 and September 2009, 987 new patients were seen at the Sleep Center (711 met the physician in person; 276 via videoconference). Of these, 174 subjects used a ResMed brand CPAP machine (111 in person; 63 via videoconference). Two subjects were excluded from the study: one was <18 years of age and one did not have adherence data in the database.
Data were analyzed for 172 subjects (111 in person; 61 via videoconference). The groups were similar in gender and age; descriptive statistics are provided in Table 3.
Descriptive Statistics—Treatment Adherence
The Mann–Whitney test was used to analyze the two variables: percentage of nights CPAP was used ≥4 h and the average minutes of CPAP use per night. The null hypothesis for the test states that the means of the two groups are equivalent, whereas the alternative hypothesis states that the two groups are different. The null hypothesis was not rejected in either analysis. Therefore, there is no difference between groups. Results from the statistical analysis are displayed in Tables 4 and 5 and Figures 2 and 3.
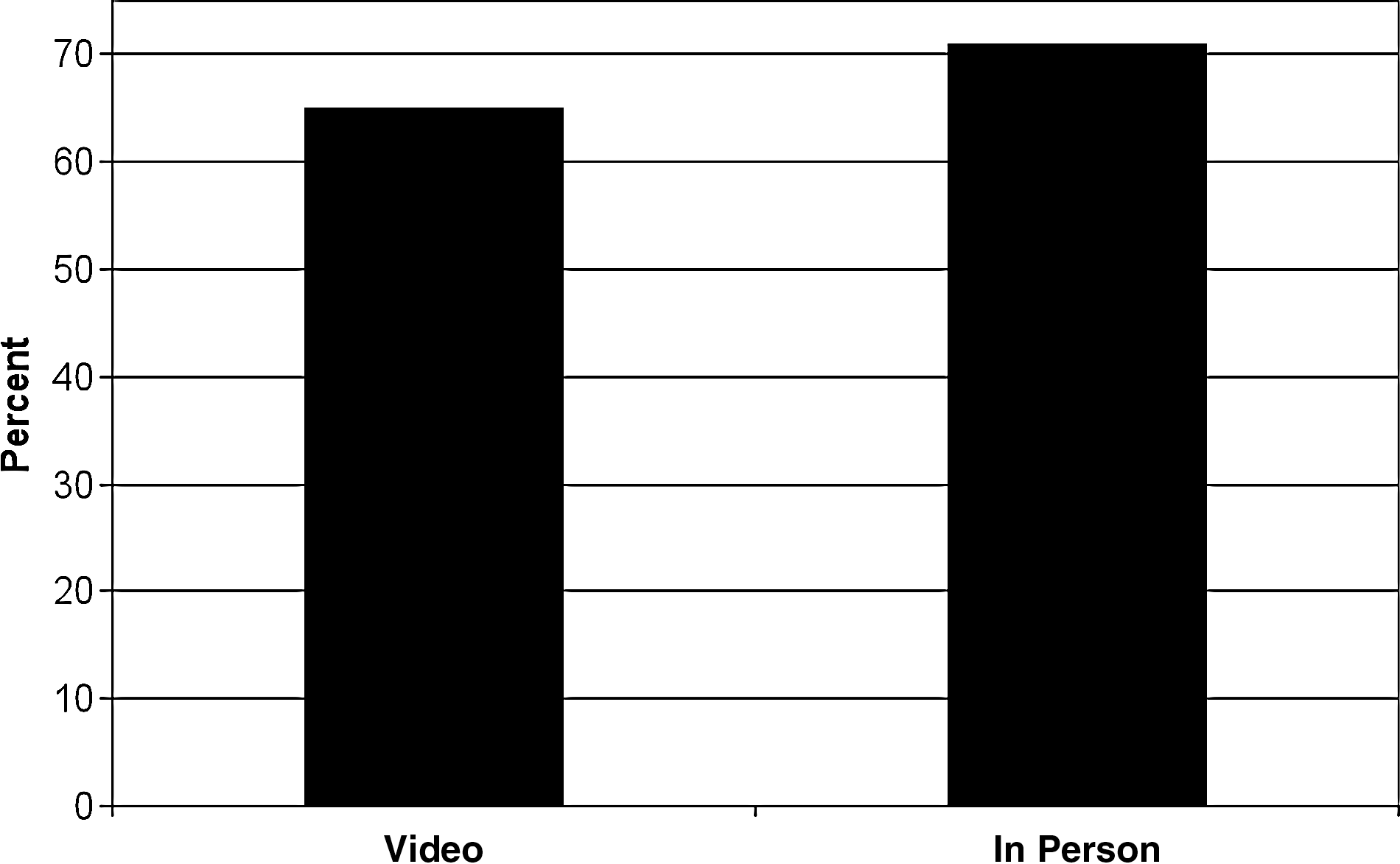
Percentage of nights continuous positive airway pressure (CPAP) was used ≥4 h.

Average minutes of CPAP use per night.
Mann–Whitney Test—Treatment Adherence (Percentage of Nights Use ≥4 h)
Mann–Whitney Test—Treatment Adherence (Average Minutes Use per Day)
Discussion
Multiple studies have shown how various telemedicine techniques have been positively viewed by patients. Smith et al. provided at home CPAP education via telehealth services, which were positively viewed by most patients. 6 Harrison et al. showed a positive patient perception of telecommunication tools in joint teleconsultation among the patient, the general practitioner, and a specialist. 27
Patient adherence to CPAP for the management of OSA has been a longstanding struggle for sleep specialists. Studies have been done to determine rates of CPAP adherence and to establish predictors of adherence. Three different studies resulted in a varying range of CPAP, with an average use ranging from 5.6 h per night to 6.2 h per night. Major predictors of CPAP compliance include subjective factors such as perceived daytime sleepiness (Epworth Score) and snoring history and objective factors such as the apnea/hypopnea index and the oxygen desaturation index. 20,28,29 Smith et al. reported that providing patient education through telehealth services at home improves CPAP adherence (90% after telehealth CPAP education vs. 44% without telehealth CPAP education) and that having the ability to monitor patients at home via telehealth services can prevent issues that would predispose people to nonadherence with their CPAP. 6
To the best of our knowledge, the use of telehealth services at the initial consultation appointment in sleep medicine has not been previously studied with respect to either patient satisfaction or treatment adherence. This study showed that patient satisfaction and treatment adherence were no different between subjects who met the sleep physician in person and those who met the sleep physician via videoconferencing. This suggests that videoconferencing may be an acceptable and effective tool to increase access to care for patients with undiagnosed OSA.
The setting from which the physician and patient each originate may influence the perception or acceptance of telemedicine. Croteau et al. showed that physicians in urban areas tend not to be willing to dedicate time to learn how to use new telemedicine equipment; however, if the technology is easy to use the correlation between ease and implementation is positive. 30 In a study of rural communities, Campbell et al. showed that physicians are more likely to adopt telemedicine technology if they perceive an increased capability of telemedicine to accommodate the constant advances of technology. In both rural and urban areas, perceived usefulness had the most significant impact on the decision to adopt telemedicine by healthcare providers. As long as telemedicine can be proven to be a useful tool for healthcare, the willingness of physicians to utilize telemedicine technology remains positive. 31
In sleep medicine, the use of videoconferencing may be particularly helpful in two different settings. First, geographical areas where sleep specialist physicians are not available would benefit from videoconferencing tools to increase access to patient care. Rural communities, for example, may lack specialist services and may benefit from videoconferencing capabilities. Second, videoconferencing may assist clinical sleep medicine practices with multiple locations and a limited number of sleep specialist physicians. For example, this system has worked well at the sleep center with locations in Peoria and Morton, IL.
Limitations of the Study
In this study, all patients were initially seen by an NP (in person) followed by the sleep specialist physician (either in person or via videoconference). Whether CPAP adherence or patient satisfaction would differ with sleep specialist physician involvement versus the NP alone was not studied. This limitation was not tested because of the limited number of patients who are seen only by an NP at the initial visit.
This study had no means to compare patient preference of in-person versus televideo visits. The only comparison that could be made was between subjects. Each subject only had a single initial visit opportunity, and they were randomly chosen to see the physician either in person or via video.
This study also does not address the cost effectiveness of the patient meeting with the NP and sleep physician in person versus the sleep physician via videoconference. The costs of videoconferencing are not examined or compared with the costs of an in-person visit with the NP and sleep physician. Notably, telemedicine evaluation and management of patients is variably reimbursed by third-party payers, partly determined by the geographic location of the patient.
Videoconferencing differs from an in-person interaction both objectively and subjectively, and patient and physician impressions may differ. For example, the lack of physical contact (e.g., a handshake) may subtly change the perception of the personal nature of the visit. Either the patient or physician may perceive less time is available to communicate, even if the time is the same as in an in-person visit. The single-camera perspective of each person in the conversation limits the movement and angle of view of each participant. Sound quality via videoconferencing is likely to significantly differ than in an in-person conversation. These potential influences on the perception of teleconferencing were not specifically investigated in this study and may be worthy of further investigation.
This study indicates that subjects were equally satisfied with their provider interaction and adherent to CPAP treatment whether they saw the sleep physician in person or via videoconference. Therefore, videoconferencing may be an acceptable and effective tool to improve access to patient care.
Further study comparing patient satisfaction and CPAP adherence among those who saw only an NP with those who also saw a sleep physician may provide valuable additional information. Future study may also include cost analysis of seeing patients via videoconference versus in person, both in settings in which reimbursement for the visit is approved by third-party payers and those in which it is not. Finally, additional investigation into the numerous objective and subjective factors that can change both the patient and physicians' perception of a visit may be warranted.
Footnotes
Acknowledgments
The authors thank Aaron Taylor, Peggy Fisher, and Catherine Lipovsky for their assistance with this project.
Disclosure Statement
No competing financial interests exist.