
Abstract
Telemedicine in the intensive care unit (Tele-ICU) has grown exponentially since the first formalized program in 2000. Initially, there was limited product choice, and certain capabilities have been engineered into the process with the implication of necessity. New technology is evolving, and new vendors are entering the market place, which should yield a multitude of technologies from which to select. To date, there has been no organized lexicon designed to facilitate communication, comparison, or evaluation. This article is designed as a starting point to develop a lexicon applicable to all technologies for the Tele-ICU with the goal of facilitating clinical comparisons and administrative choices.
“Mr. Edison, I was informed, had been up the two previous nights discovering “a bug” in his phonograph–an expression for solving a difficulty, and implying that some imaginary insect has secreted itself inside and is causing all the trouble.”
Introduction
Technical language evolves sometimes by accident, sometimes in an orderly fashion. Edison's computer “bug” was not an insect but understood to be some vague process-causing malfunction deep within the electronic device, and so “bug” became the accepted lexicon for computer science. From time to time, new definitions should be established. Time is past due to develop a lexicon for the utilization of telemedicine in the intensive care unit (ICU). There exists significant technical lexicon for telemedicine 1 and a clear understanding that technical “informational literacy” will help clinicians understand conceptual differences in the telemedicine technology. 2 In general, lexicon has evolved in the larger field of telemedicine to include “tele-pathology,” “tele-dermatology,” tele-radiology,” and so on. 3 However, to date, we could not discover any published lexicon describing the structure and function of the telemedicine in the ICU (Tele-ICU). Therefore, in creating this lexicon document, new meanings and concepts will be proposed, in some cases, without previous references. The intent of this article is to grow a technical language that will facilitate evolution of discussion. A high-level, technical language, when uniformly used across all vendors and devices, should organize the thought process for comparison yet should be comprehensible by the relative novice. Additionally, the goal would be to develop definitions that are intuitively meaningful. As a consequence, visual image and concrete examples will be an important aspect of these definitions.
As defined by the American Telemedicine Association (ATA), “Telemedicine is the use of medical information exchanged from one site to another via electronic communications to improve patients' health status.” The ATA suggests that telemedicine “may assist in addressing the shortage of healthcare providers by promoting new models of practice that improve the effectiveness and efficiency of the care process,” improve distribution of services, and partially mitigate the physician manpower shortage. 4 Others describe telemedicine as a “branch of e-health that uses communications networks for the delivery of healthcare services and medical education form one geographic location to another. 5
The introduction of telemedicine into the ICU dates back 20–30 years with the early efforts of Grundy et al. 6,7 In the United States, telemedicine in the ICU has gone through an explosive growth phase since the first, commercial system installation in Norfolk, Virginia, in 2000. 8,9 During the decade 2000–2010, a single design has largely driven growth in the Tele-ICU arena. More recently, there has been significant growth with other vendors and technologies.
The impetus driving telemedicine in the ICU evolved from a recognized manpower maldistribution 10,11 critical care manpower shortage, 12 –16 growing clinical support for intensivists, 17 –20 influence from the Leapfrog group, 21 successes with a systematic approach to telemedicine in the ICU, 8,9,22 and support for increasing telemedicine as part of healthcare reform. 23,24 The intensivist, when employing telemedicine technologies, can have a significant and positive impact on outcomes of the critically ill patient. 8,9,25,26 Elements of the visual examination and visual review of graphical waveforms improves accuracy of decision making. 27,28 There are multiple reports suggesting better compliance with evidence-based medical protocols when a centralized telemedicine process is in place. 29 –35 Telemedicine may have even greater impact in the rural environment. 36 –39 Therefore, we believe that Tele-ICU is here to stay, although evolution is inevitable.
The Tele-ICU is defined as “Networks of audio-visual communications and data systems to link hospital ICUs to intensivists and other critical care professionals at remote locations.” 40,41 As with other focused fields of endeavor, understanding the Tele-ICU literature requires knowledge of the process. Further, understanding the comparative basis of Tele-ICU models will be vital. To date, there have been no head-to-head evaluations of the various alternative technologies, networking models, or staffing structures for the Tele-ICU. It remains unclear what informational elements are absolutely mandatory to facilitate best diagnostic and therapeutic decisions via telemedicine or tele-presence or what elements are unnecessary, superfluous, or over engineered. Once the lexicon is developed, the next step may be to perform a structured comparative evaluation of systems such as suggested by the Office for the Advancement of TeleHealth, Health and Human Resources Services Administration, and the National Center for Research Resources. 42
Background and Process
To achieve the goal of lexicon development, national experts in the field ICU telemedicine have been recruited to develop and review the current article. For the purposes of this article, “expert” candidates were selected as individuals who are physicians working clinically, either trained in critical care medicine or actively working in critical care medicine, with at least 5 years of experience in telemedicine, and have a national/international presence by either committee work, editorial positions, or original contributions to the related literature. As is the nature when employing clinicians, each expert may have clinical experience or bias with specific technologies and vendors. Therefore, experts with multiple perspectives were recruited to develop a balance of opinions. All potential conflict of interest is described in each author's financial disclosure in the appendix. Specific acronyms were avoided in the development of the lexicon.
The specific lexicon developed was by group consensus so as to • Generically define major distinguishing characteristics between existing systems. • Create verbage describing current variable usage patterns. • Avoid fine technical details likely to be outside the purview of administrators and clinicians. • Create a language that is flexible enough for future evolutions of the Tele-ICU.
Due to manuscript length limitations, some definitions were not included with the hope that the current foundation will serve as a living document for future growth of the language.
In developing descriptors, it was necessary to be relatively rigid while recognizing that there may be systems with multiple or over-lapping characteristics. To give life to this effort, once the descriptors have been developed, then existing vendors are described by using the new definitions.
The following descriptors have been created:
General Descriptors: 1. Intensivist or Tele-ICU Intensivist 2. Virtual Presence or Bedside presence 3. Surrogate examiner and Surrogate “Hands” 4. Tele-ICU or Tele-Critical Care 5. Tele-Expertise or Tele-Surveillance
Structural Descriptors: 1. Centralized or De-Centralized Tele-ICU 2. Open, Closed, and Hybrid Communications Architecture 3. Fixed versus Portable technology at the ICU end a. Dependent portability b. Semi-autonomous, independent portability c. Autonomous, independent portability 4. Fixed, Portable, Mobile technology at the Tele-ICU (user) end 5. Tele ICU Clinical Information Systems (CIS) a. Independent Tele-ICU only CIS or b. Hospital Wide Integrated CIS.
Care Models: 1. Continuous 2. Pre-Emptive/Scheduled 3. Reactive
General Descriptors
Intensivist or Tele-ICU Intensivist
Intensivist
A physician with additional, sub-specialty fellowship training in the defined field of Critical Care Medicine who can provide both cognitive skills and psychomotor skills in the care of the critically ill patient. 43 Intensivists may have background training in either internal medicine, anesthesia, surgery, or emergency medicine.
Tele-ICU intensivists
An Intensivist, as just described, who provides cognitive skills via virtual presence 44 and directs, requests, or delegates the performance of psychomotor skills at the bedside through a “surrogate examiner” or via “surrogate hands.”
Remote Presence or Onsite Presence
Onsite presence
Traditional visitation at the bedside by a care provider that includes elements described in Remote Presence plus “hands-on” contact such as palpation of the abdomen, assessment of skin temperature, auscultation of heart and breath sounds, and so on.
Remote presence
The use of audio-video technology to place the remote care provider (physician, nurse, or intermediate level care provider) virtually at the bedside for real-time, two way verbal and visual communication, review of bedside graphics, and visual patient examination. There is no direct “hands-on” contact with the patient, but there may be surrogate “hands-on” examination. Remote presence examination can include auscultation of the heart, lungs, abdomen, vascular bruits, and so on with the use of electronic stethoscope as well as ophthalmologic funduscopic exam, otologic exam, and/or real-time ultrasound examination.
Surrogate Examiner/Surrogate Hands
Generally, the Tele-ICU Intensivist is remote from the hospital ICU or if in proximity to the ICU, the Intensivist would generally be restricted from leaving the Tele-ICU. In the normal process of care, it may be necessary to perform certain elements of examination such as palpation for crepitus, for warmth or coolness, or fluctulance, all of which can be performed by a bedside nurse. Higher skill level may be required to perform airway intubation, central line insertion, closed thoracostomy tubes, arterial line insertion, lumbar puncture, and so on. The remote Tele-ICU intensivist will delegate those psychomotor skills to a trained, on-site individual (see “Surrogate Hands).
Surrogate examiner
This could be the same person as the individual performing bedside procedures but more likely is the bedside nurse, resident, or fellow. Necessary points of examination are performed at the direction of and/or during observation by the Tele-ICU intensivist who can observe the examination, provide immediate feedback, or coach elements of the examination.
Surrogate “Hands”
Can be any of several individuals who will be available to perform procedures. Options for “surrogate hands” include the following: 1. Medical/Surgical Residents in a training program 2. Critical care Fellows in a fellowship program 3. In-house Hospitalists 4. In house Anesthesiologists/Anesthetists 5. Cross coverage by Emergency Department physicians 6. Respiratory Therapists with airway management skills 7. Dedicated “Line Teams” for insertion of central lines 8. Acute care nurse practitioner or physician assistant
Tele-ICU or Tele-Critical Care
Tele-ICU
Refers to “where” the remote critical care services originate (the intensivist end). The Society of Critical Care Medicine (SCCM) and the internal medicine committee of the SCCM have adopted the phrase “Tele-ICU.” Adoption of the term, although somewhat imperfect, was partially driven by a growing acceptance and usage by The Center for Medicare and Medicaid Services. The same terminology has been adopted by the ATA Tele-ICU “Discussion Group.” The four letters “eICU” are trademarked and will not be used in this article. “Tele-ICU” implies a specific physical existence and location. Though generally accurate, there are multiple applications that do not operate from a single, discrete site. Despite some ambiguity, the term “Tele-ICU” will be used to define the discrete electronic ICU or distributed, open architecture electronic ICU programs.
Tele-critical care
Refers to where the critical care services are provided (the patient end). A more general phrase suggesting that the delivery of telemedicine critical care services is not site specific. Critical care could be provided in the ICU, the general medical/surgical floors during a rapid response event, the emergency department, or in the Post Anesthesia Care Unit (PACU) after surgery.
Structural Descriptors
Centralized or De-Centralized Tele-ICU
The centralized tele-ICU
A hub-and-spoke model from which critical care services originate. 32 The hub (or center) is an established, remote site with staffing to include intensivists, nurses, and clerical and technical staff. The established hub is connected to multiple medical facilities and/or multiple ICUs (Fig. 1).
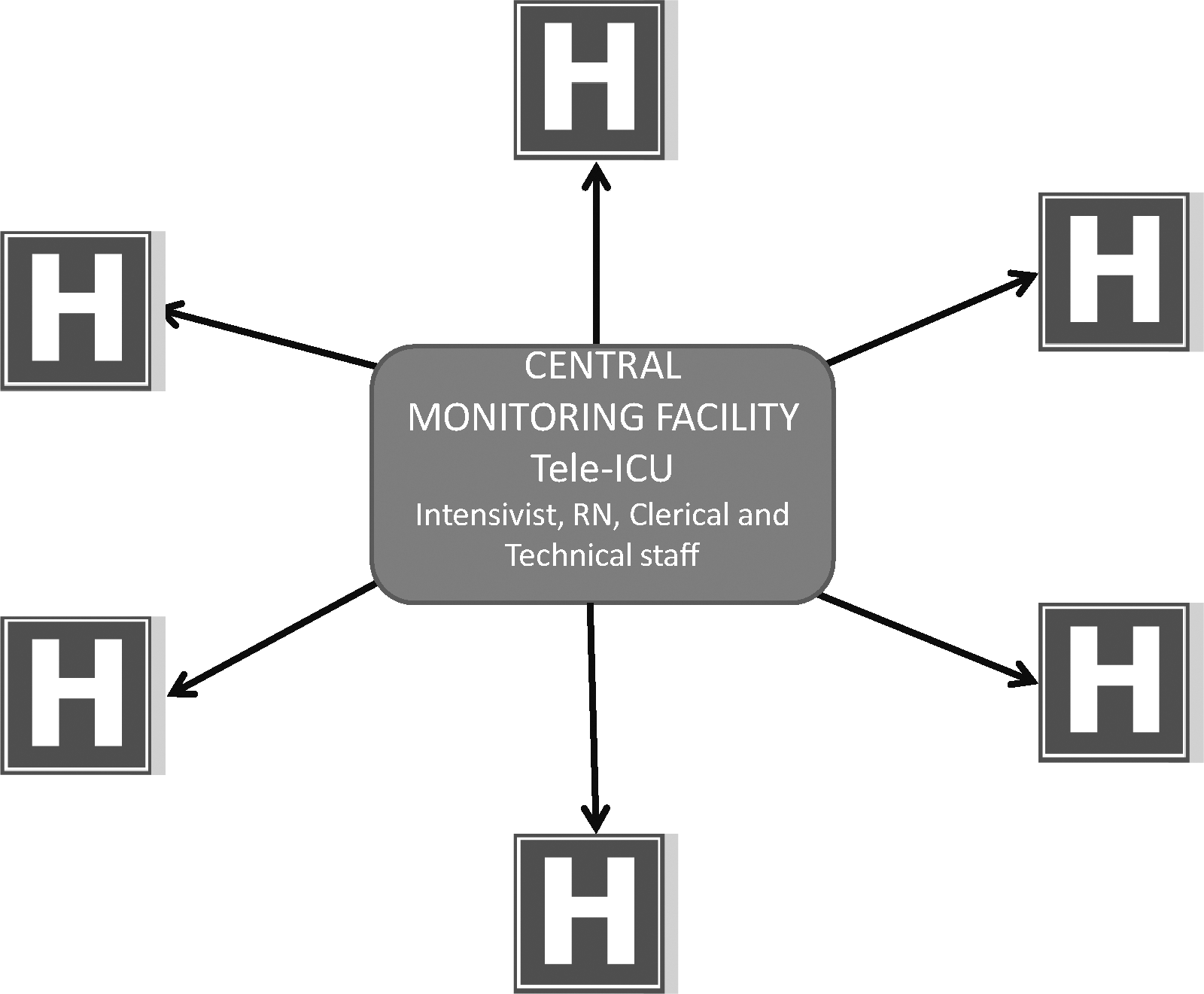
Centralized Tele-ICU with an established central monitoring facility. The central monitoring facility is a real and defined site, staffed variable periods per day ranging from 12 to 24 h.
The de-centralized tele-ICU
A reverse, hub-and-spoke model. 45 In this model, there is no defined established central monitoring facility. The de-centralized model typically involves computers equipped with camera, speakers, microphones located at sites of convenience such as physician offices, homes, or mobile sites utilizing laptop computers or smart phones. Therefore, the de-centralized Tele-ICU is not a specific or single site but rather a process (Fig. 2).

Decentralized Tele-ICU has no established central monitoring facility. This diagram indicates a single medical facility at the Hub. The open architecture De-Centralized Tele-ICU could connect with multiple facilities.
Communications Architecture: Open, Closed, or Hybrid
Open architecture
A flexible, undedicated communications system
46
that supports connectivity by one or multiple care providers from one or multiple sites to one or multiple sites. Open architecture generally implies connectivity via the Internet. Open architecture networks may take any of the following forms: a. Single Physician, To a Single Site with Multiple Patients. One physician (from home or office) providing critical care services to one ICU and providing care for any or all the patients within that ICU. b. Single Physician, To Multiple Sites, Multiple Patients. An individual physician could be virtually present at several different medical sites from a home or office and provide services for some or all patients at each site. c. Multiple Physicians, From Multiple Sites, to a Single Patient. Multiple physicians to simultaneously evaluate a single patient from different sites (Fig. 3). d. Multiple Physicians, From Multiple Sites, To Multiple Sites, Multiple Patients. Open architecture can support capability to access patients located at multiple sites from one or more different remote care provider sites.
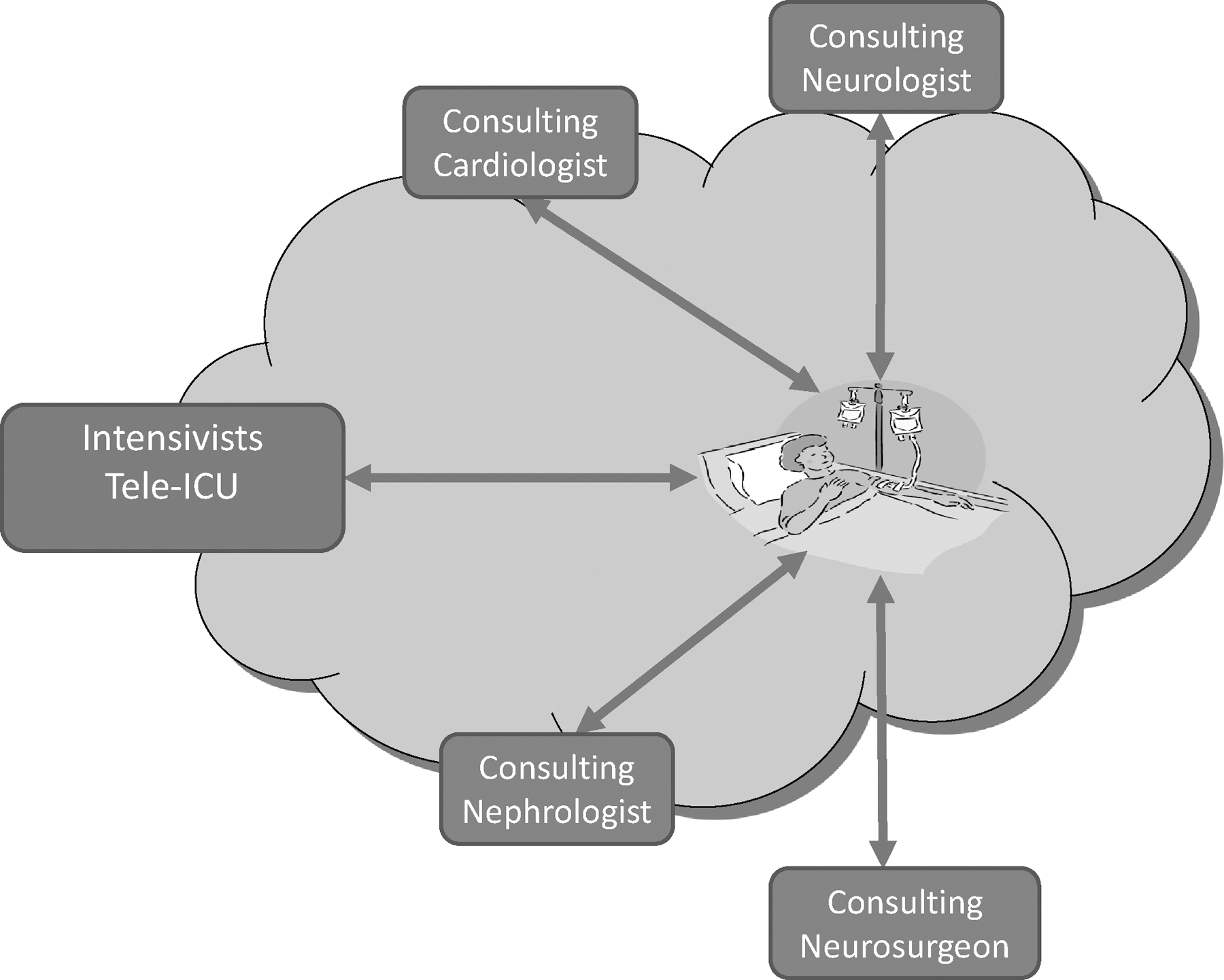
Open architecture system in which multiple physicians or consultants can access the patient (via audio-video) and patient clinical information simultaneously. The “cloud” is meant to indicate the Internet.
Each care provider has full access to all information about the patient to include audio-video connection, access to the CIS, and digitized radiographic information. Functionally, each physician is within the “system.”
Closed architecture
A system that supports point-to-point communications. 47,48 Specifically, a closed architecture Tele-ICU would be point-to-point communication to a patient from a central monitoring facility. For purity of definition, there would be no option for physicians outside the closed system to have full access to patient audio-video, clinical or radiographic information. Medical consultants would be functionally external to the Tele-ICU system and could only evaluate a patient via traditional communications such as the telephone system (Fig. 4).

Closed architecture with direct physician to patient communications limited to care providers within the central monitoring facility. Generally, subspecialties are excluded from direct patient visualization and communication limited to traditional telephonic modalities and are functionally outside the Tele-ICU system.
The closed architecture model generally employs dedicated high-speed lines. Functionally, the closed architecture exists outside the Internet, although internal data may be transmitted over high-speed cables or fibers by using Internet Protocol (IP).
Combined hybrid open and closed architecture
By combining the capabilities of the open and closed architecture, 49 it may be possible to achieve greater connectivity, maximize inclusivity of consulting or community physicians, keeping costs within reach, and getting high-level reliability of dedicated lines. Conceptually, the hybrid architecture could look as shown next in Figure 5.
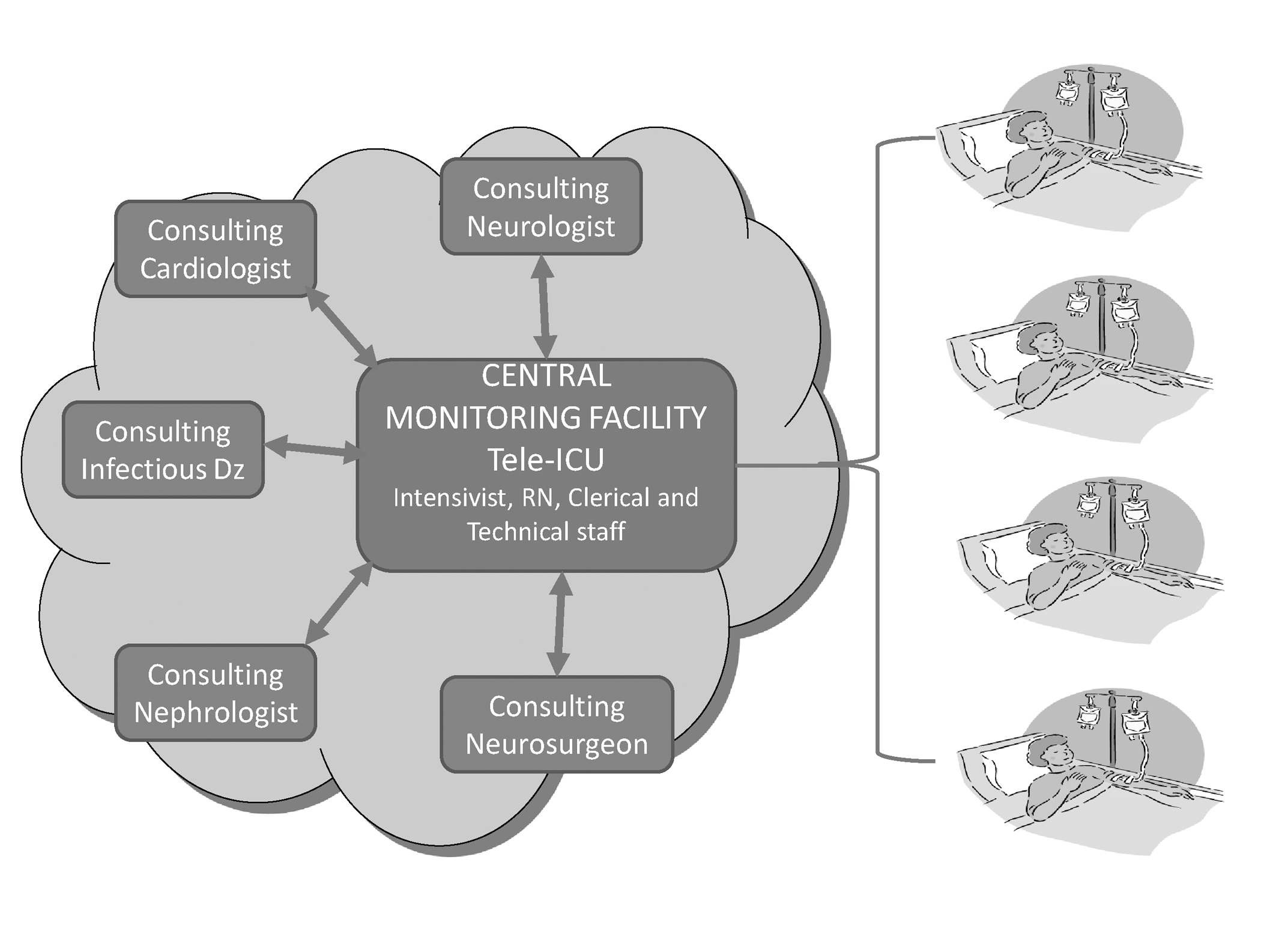
Combined open and closed architecture. A network of physicians would be able to access the patient audio-video information and other technical data from the Internet. However, the Tele-ICU, as such could be external to the Internet. The “cloud” is meant to indicate the Internet.
Utilizing Internet connectivity from consultant office sites, including wireless mobile technology, would enable a larger spectrum of clinicians to participate in patient care and render patient care with the benefit of ALL clinical information. Such clinicians are functionally within the Tele-ICU system. Meanwhile, the Tele-ICU can maintain the security and reliability of dedicated lines from the Tele-ICU to the patient bedside.
Technology at the ICU End: Fixed or Portable
Fixed at the ICU end
Audio-video devices are permanently attached to some site in proximity of the patient, 8,9,44 facing the patient generally from the foot of the bed (Fig. 6). The camera may be connected to the hospital network, have an IP address, and be Web accessible. To provide the audio, cameras can be equipped with Voice over Internet Protocol technology to support the two-way audio. Commercially available packages usually provide software for the remote control of Web-enabled devices.

Simple, fixed cameras located on the ceiling over an ICU bed (left). Sophisticated camera, speaker, and microphone with a screen to show remote Tele-ICU physician (middle). Commercially available software for the remote control of cameras via the Internet (far right).
Portable technology at the ICU end
Systems are brought to or arrive at the bedside. Portable units, generically referred to as “Carts,” provide two way, real-time, audio and video communications (Fig. 7). Portable technology may be wireless and perform within a wireless environment or require access to a Local Area Network drop access point via a cable and jack-type connection to the network. Portable systems can move or be moved outside the ICU room to participate in family conferences, collaborative rounds, physician-to-physician conversations, or “Rapid Response” activities.

Portable devices to include (from left to right) Global Media cart, Polycom cart, Tandberg cart, Intouch Health cart, and Intouch Health “Robot.” All the devices just described are dependent on local personnel for movement except the “Semi-Autonomous” Intouch Health robot on the far right.
Portability at the ICU end may be further subcategorized as follows: 1. Dependent Portability: A cart system that is dependent on personnel who should push the device to the bedside, activate the device, sometimes re-position to achieve optimal view, and then return the device to a storage site. In addition, the device will need to be disconnected and reconnected to power for battery charge. 2. Semi-Autonomous Independent Portability: Movement of the device is under the direct, real-time control of the remote clinician. Semi-autonomous devices, generally called “Robots,” operate within a wireless hospital environment and will not require physical connection to the hospital network, can be driven to any site within the ICU, and can be repositioned by the remote operator completely independent of local personnel. 3. Autonomous Independent Portability: At this point, fully autonomous devices remain in development. Movement to the bedside would be based on pre-programming within the ICU and would not require ICU personnel for assistance. In addition, the remote operator would not be required to have geographic knowledge of the ICU environment. When the remote care provider is summoned to a particular bed, then the remote operator would send a command for the device to go to that particular bed.
Technology at the Tele-ICU End: Fixed, Portable, or Mobile (m Health)
Fixed technology at the tele-ICU end
The “Tele-ICU end” refers to the site from which the remote care provider originates the telemedicine service (Fig. 8). “Fixed Technology” will include equipment so bulky, complex, or heavy that would not be easily moved. 8,9,22,45
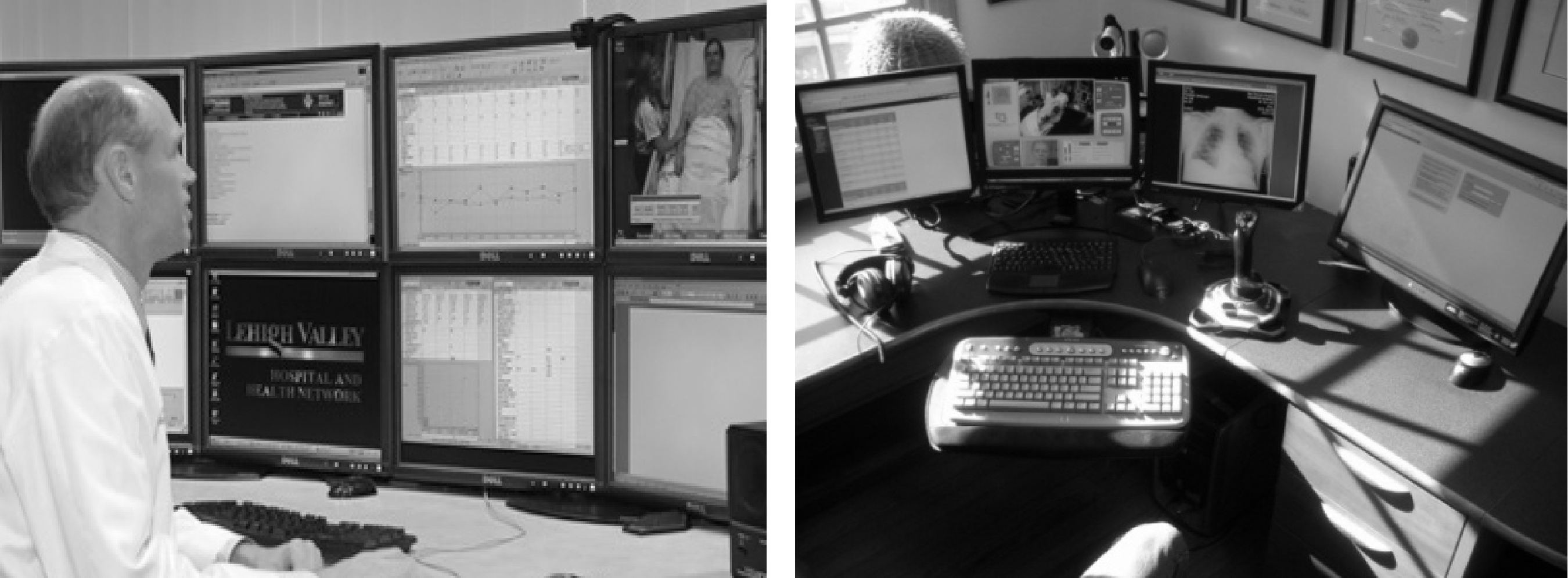
Two types of “Fixed Technology at the Tele-ICU End.” On the left is the Centralized Monitoring Facility, iMDSoft Installation at Lehigh Valley Hospital Center, Lehigh Valley Pennsylvania. On the right is a de-centralized physician work station at a home Tele-ICU site.
Portable technology at the tele-ICU end
Technology or equipment that allows the remote care provider freedom of movement while supporting two way audio-video communications and access to clinical data, real-time vital signs, or radiographic information, and so on (Fig. 9). For the purposes of this lexicon, “portable,” requiring laptop devices has been separately defined from “mobile” as described next. 50,51 Typical requirements include a portable “laptop” computer, necessary communications software, built-in or attached camera, speakers, microphone, with hard-wired, Wi-Fi, or Broadband Internet access. The portable care provider may access patients remotely from home, office, hotel lobby, roadside, and so on.

Portable laptop devices for two-way audio-video communications and virtual presence.
Mobile or “mHealth” technology at the “Tele-ICU” end
mHealth is the practice of healthcare delivery by ultra-mobile devices. 52,53 mHealth includes hand-held smart-phones that can provide the mobile remote clinician with audio-visual patient access and/or graphical data access (Fig. 10).
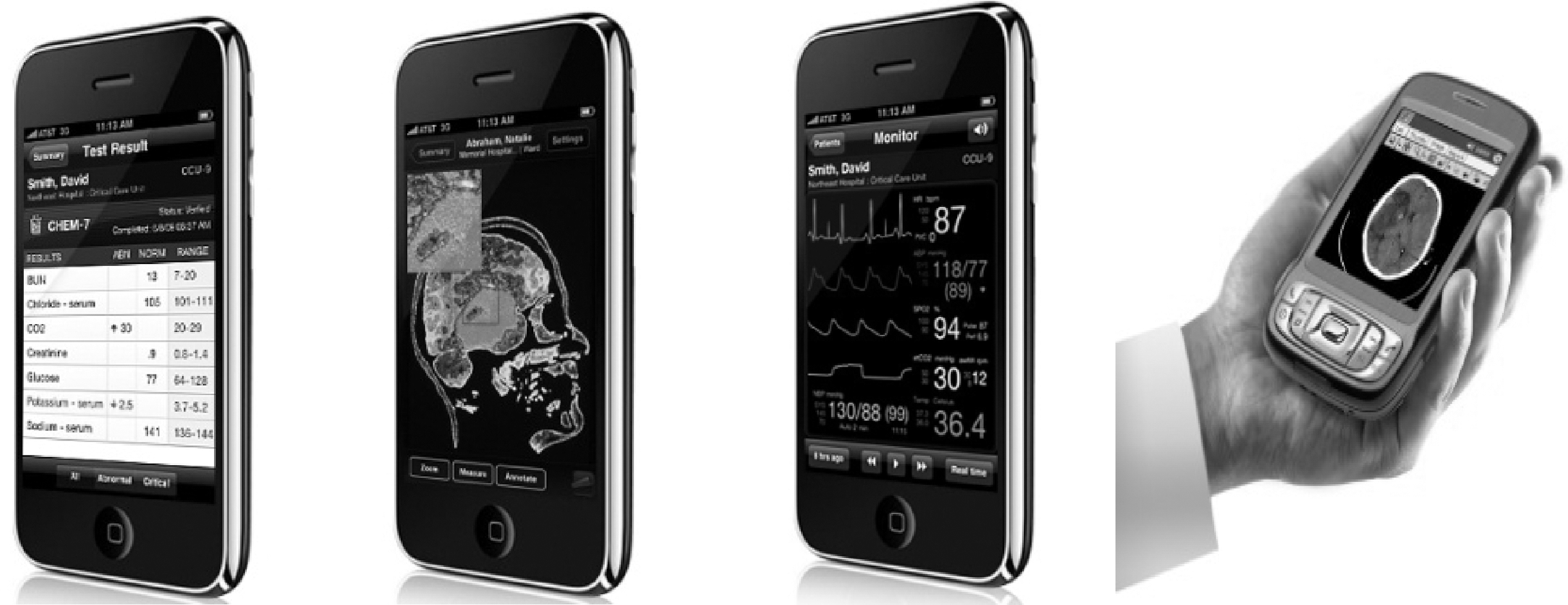
Mobile devices with access to graphical information to include Airstrip Technologies (San Antonio, TX) with laboratory, radiographic, and vital signs data (three left-handed images) or Global Care Quest (right image).
Tele-ICU CIS: Tele-Icu Only CIS or Hospital Wide Integrated CIS
For purposes of description, the following will be defined as if pure. However, systems may evolve from independent to integrated with the gradual development of various interfaces.
Tele-ICU only CIS
A Tele-ICU system that uses a separate CIS in the ICU only without integration to the hospital wide CIS. 8,9,55 The electronic database is created independently once the patient is in the ICU and does not move with the patient as the patient transitions back out to the general medical/Surgical floors.
Hospital wide integrated CIS
A Tele-ICU system that uses the facility's existing CIS. 22 The electronic database is created at any entry point to the hospital and moves with the patient as the patient transitions from the Floor/ED/PACU to the ICU or when moving back out to the general medical/surgical floors.
Care Models: Continuous, Pre-Emptive/Scheduled, Reactive
Care models may vary widely. The following definitions are presented assuming care models are distinct. However, some programs may offer all or several different forms of care models. The intent is to develop an understanding of how the care is being delivered and to be able to describe the care model succinctly.
Continuous care model
The word “continuous,” implying absolute 24×7 monitoring, requires some consideration. Continuous may be 24×7 or limited to 8, 12, or 18 h per day depending on institutional needs and contractual agreement between medical facilities. 8,9,22 The concept of continuous care may be further nuanced based on different staffing models. Certain arrangements include 24×7 critical care nursing monitoring with the intensivists providing support during the 8, 12, or 18 h per day. See concept diagram in Figure 11.
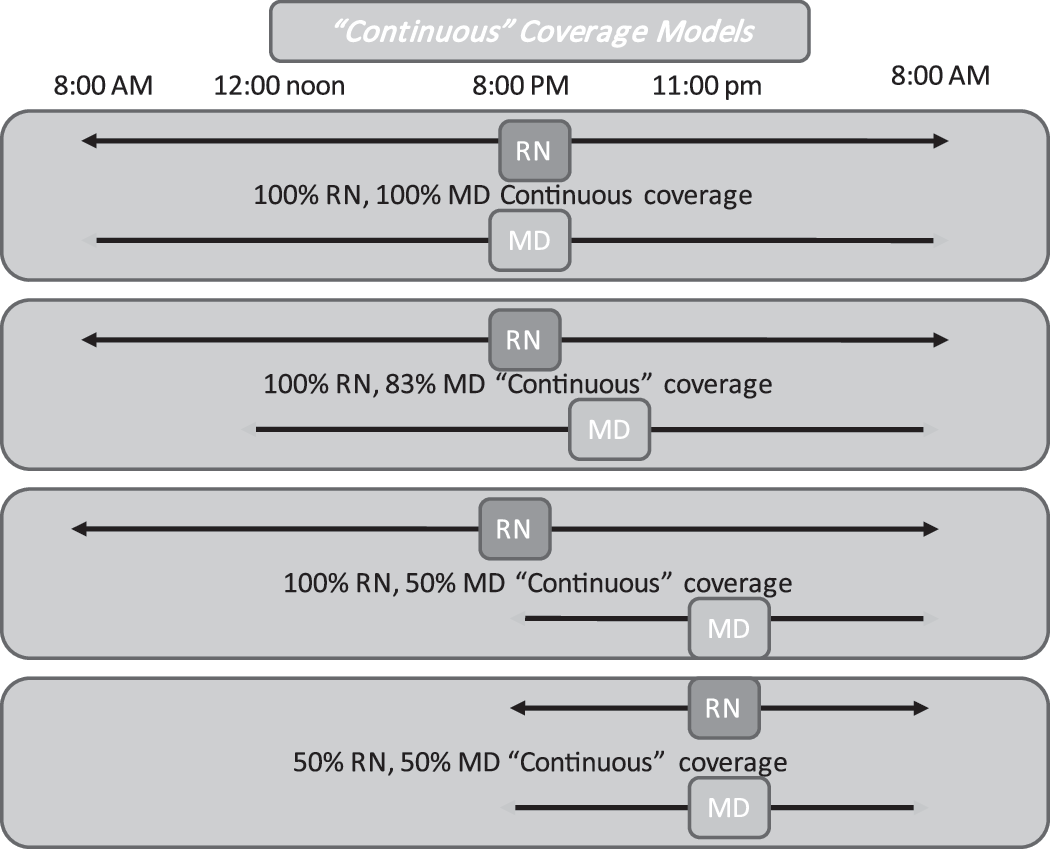
Various paradigms for “Continuous Care.” Top panel describes a true 24×7 continuous care and monitoring program with both monitoring nursing staff and intensivists continuously active. Least involvement shown in lowest panel with remote care and monitoring enabled when local hospital staff is least available.
Within the Continuous Model, there are other nuances. The level of coverage provided may vary from patient to patient. Specifically, by contractual agreement, private attending physician staff may be given the right to completely opt out of the remote Tele-ICU services or transfer a very high level of responsibility to the Tele-ICU. By opting out, the private attending patient may only receive emergency care, as the attending is summoned to the bedside. Legal counsel may mandate that programs offer the patient the option to “opt out” of Tele-ICU services.
The pre-emptive/scheduled care model
A Tele-ICU program in which the virtual visits occur at a defined time and are not in response to a physician page or solicitation. 56,57 The pre-emptive virtual visit may be routinely timed to occur several hours after the intensivist has left the ICU premises, for example, routinely at 10:00 pm. The scheduled visitation model, although only minimally different than the Pre-Emptive model, includes the scheduled performance of routine daily ICU rounds more typically during the morning hours, even though it may include both morning and afternoon rounds and team/collaborative rounds.
The reactive tele-ICU care model
Includes a virtual visit for the purpose of responding to an acute physiologic issue or for the performance of a critical care consultation. 58 Reactive virtual care would be unscheduled and unpredictable.
Application of the Lexicon to Existing Technology
To give life to the lexicon just described, known current and future programs and products were described with the developed terminology. Other than Skype, only U.S. products were reviewed. There was no attempt to examine international products. There was no malice or fore-thought if a U.S. product was overlooked. The lexicon was applied either from direct communication with vendors, personal experience of one or more authors with the vendors, and/or review of any written and published literature. Estimates describing market penetration were not independently verified. Although the descriptors and lexicon may not fit with absolute precision, the effort was to give a generally fair description and, therefore, a fair, real-world demonstration of the lexicon in action.
All known U.S. vendors, providing Tele-ICU programs or CIS that have or could evolve to a Tele-ICU program, were queried. In some cases, there is no program and no stated intention to enter the market. In some cases, there is a clear intention to enter the market pending development of product and complete resolution of patent-related litigation. Generally, the products have been listed in order of decreasing market penetration and/or closeness to providing an actual “Tele-ICU” (Table 1).
Summary Description of Current Tele-ICU Technology
Discussion
The intent of this lexicon is twofold. The first intention is to stimulate and broaden the range of technological discussions. With the recent resolution of a patent infringement suit, multiple vendors are likely to enter the Tele-ICU market, particularly considering the growing physician shortage, size of the Tele-ICU market, maldistribution of physicians, and recent emphasis on telemedicine as part of healthcare reform. As new vendors move into the market, there will be greater variability in products with more available choices to make when establishing a Tele-ICU program. Therefore, it is incumbent on the purchaser to have a higher level of sophistication in making choices rather than relying on the word of vendors. To make such choices, it is not necessary for the administrator or clinician to be knowledgeable at the micro level such as switching theory, bytes versus bits, Cable Cat, or specifics of data transmission speed. Rather, it is important to have the high-level view of systems with the advantages and limitations. In this article, we have begun to develop some of the high-level definitions and lexicon for the Tele-ICU.
Second, this lexicon aims at setting the stage for comparative analysis and to ask the question, “What system provides the best patient outcomes at an affordable cost.” Some of the current Tele-ICU systems have evolved substantial capability with the implication that these capabilities are necessary. Now, it is time to begin the high-level discussions regarding where the technology should go next.
Almost all the technologies discussed in this article are currently available and deployable. However, certain applications, such as the “autonomous independent portability,” have not yet been deployed as described. Further, higher-level hybrid models are just evolving, and final forms are yet to be defined.
Conclusion
Telemedicine has become an ever-increasing part of the medical delivery system driven by the evolving and aging demographics, increased demand for ICU care, cost containment initiatives, limited manpower supply, and mal distribution of care providers. The Tele-ICU technology should continue as an integral part of the solution for the Critical Care Manpower shortage. However, the ultimate technology and supporting scientific studies will need to continue to evolve.
We believe that the future of the Tele-ICU will include a more open architecture that permits the mobile consulting physician full access to patient information from any site. Additionally, the open architecture will provide cost savings for physician coverage, as professional fees could be reduced to an “on-call” standing charge and as needed consultation charge rather than the 24×7 hourly physician costs. Similarly, the “on-call” structure improves the feasibility to have multiple or essentially all subspecialists available. Open architecture should integrate with the hospital system clinical information to enhance access for the mobile physician. Hybrids are expected to evolve that may include combined de-centralized sites with centralized sites and systems offering different technologies at different facilities. There will likely be less dependence on costly fixed and dedicated “high speed” lines and, as wireless broad band increases in availability and speed, greater utilization of the open network provided by the Internet or extremely high-speed wireless networks.
Cost of the technology is expected to come down as more vendors enter the market and provide a wider spectrum of solutions. Cost of personnel and manpower supply will continue to be problematic unless models evolve that permit satisfactory and acceptable physician “personal life choices” while still providing quality patient care. It is conceivable that the central monitoring site could be populated only with nurses and mid-level practitioners with all the physician back up located at de-centralized sites such as home, office, or mobile devices.
Finally, introduction of the Tele-ICU technology has often been limited or delayed due to resistance from local or community physicians. With open architecture networking, the local community of physicians can have access to the system and collaborate/participate in the remote care of their own patients. Although costs of technology, manpower shortage, and cultural adaption are currently major issues, continued experience and published peer-reviewed literature will position the Tele-ICU as an essential and integrative process.
Footnotes
Disclosure Statement
H. Neal Reynolds, M.D.—Unfunded Board of Advisors, In Touch Health.
Herb Rogove, D.O.—President and CEO of the private company, C3O providing remote clinical support.
Joseph Bander, M.D.—None.
Matthew McCambridge, M.D.—None.
Elizabeth Cowboy, M.D.—Employee of private corporation, Advanced ICU.
Michael Niemeier, M.D.—None.