
Abstract
Introduction
Fine-needle aspiration (FNA) biopsy is an accepted diagnostic modality for evaluating thyroid nodules, and often is the initial step in diagnostic assessment of thyroid lesions. FNA is now considered to be the most accurate, cost-effective, and simple screening test for rapid diagnosis of thyroid nodules with accuracy approaching 95%. 1 Pathologists at several institutions perform on-site preliminary evaluation of material obtained by thyroid by rapidly staining cytologic smears. Immediate feedback is provided to clinicians or radiologists regarding whether adequate material has been obtained and preliminary cytologic diagnosis may also be rendered. Distances of radiology suites and physician-based FNA clinics from pathologist's offices and laboratory and multiple locations for aspiration procedures are an impediment for a timely immediate on-site assessment by pathologists. In addition, these procedures can be time consuming.
Telepathology facilitates transmission of microscopic images via Internet connections for online consultation and diagnosis. Dynamic telepathology systems focus on transmission of live images that are viewed electronically in real time at a remote site in contrast to static telepathology systems that are based on capturing of cytologic pictures in a digital format and then transmitting to distant observers. 2 A recent study revealed that onsite evaluation of FNA specimens from pancreas, gastrointestinal tract, liver, and lymph nodes via dynamic telecytopathology assures sample adequacy and accurate preliminary diagnosis. 3 High diagnostic concordance of 97% and diagnostic accuracy rate of 99% was reported in another recent study that evaluated the feasibility of using a dynamic telepathology system for making preliminary diagnosis of hundred FNA specimens procured from various body sites, including nine thyroid FNAs. 4
Reproducibility of thyroid lesion using static telecytology system based upon transmission of selected digitized images has shown promising results. 5,6 In this retrospective study we present our experience with use of dynamic telecytopathology for preliminary evaluation and diagnosis of ultrasound-guided FNA (USGFNA) biopsies of thyroid nodules performed by endocrinologists and surgeons at a distant site and compare it to final cytologic diagnosis.
Materials and Methods
The study involved USGFNA biopsies of thyroid nodules performed by endocrinologists and surgeons at two remote offices located away from the SUNY Upstate University Hospital. On-site cytotechnologist prepared cytology smears that included Diff-Quik-stained slides and alcohol-fixed smears that were later stained with Papanicolaou method in the laboratory. Total number of Diff-Quik-stained slides prepared on site ranged from 2 to 5 slides. Additional material was collected for cellblock as needed. A maximum of 4 passes were performed per thyroid nodule. Initially, two passes were performed and evaluated with telecytopathology system. Additional passes were performed only if the initial two passes did not yield adequate material for preliminary diagnosis.
Telecytopathology was introduced in the two remote offices in February 2010.
A telepathology system consisting of an Olympus CX41 microscope and a digital camera with NetCam software was used to transmit the images (Fig. 1). A 2.11-megapixel cooled digital color camera (Olympus DP20; Olympus America, Center Valley, PA) was used for image acquisition with the microscope (Olympus CX41) and a Dell desktop computer with a direct Ethernet connection. NetCam software (Olympus) used transmission control protocol/Internet protocol (IP) to transmit live images over the Internet via an assigned static IP address (Figs. 2 and 3). The computer and the image server required login and the IP address was known to the faculty or the operators of the microscope. The original size of the acquired image was 800×600 pixels with the NetCam transmitted image having a resolution of either 800×600 or 640×480 pixels.
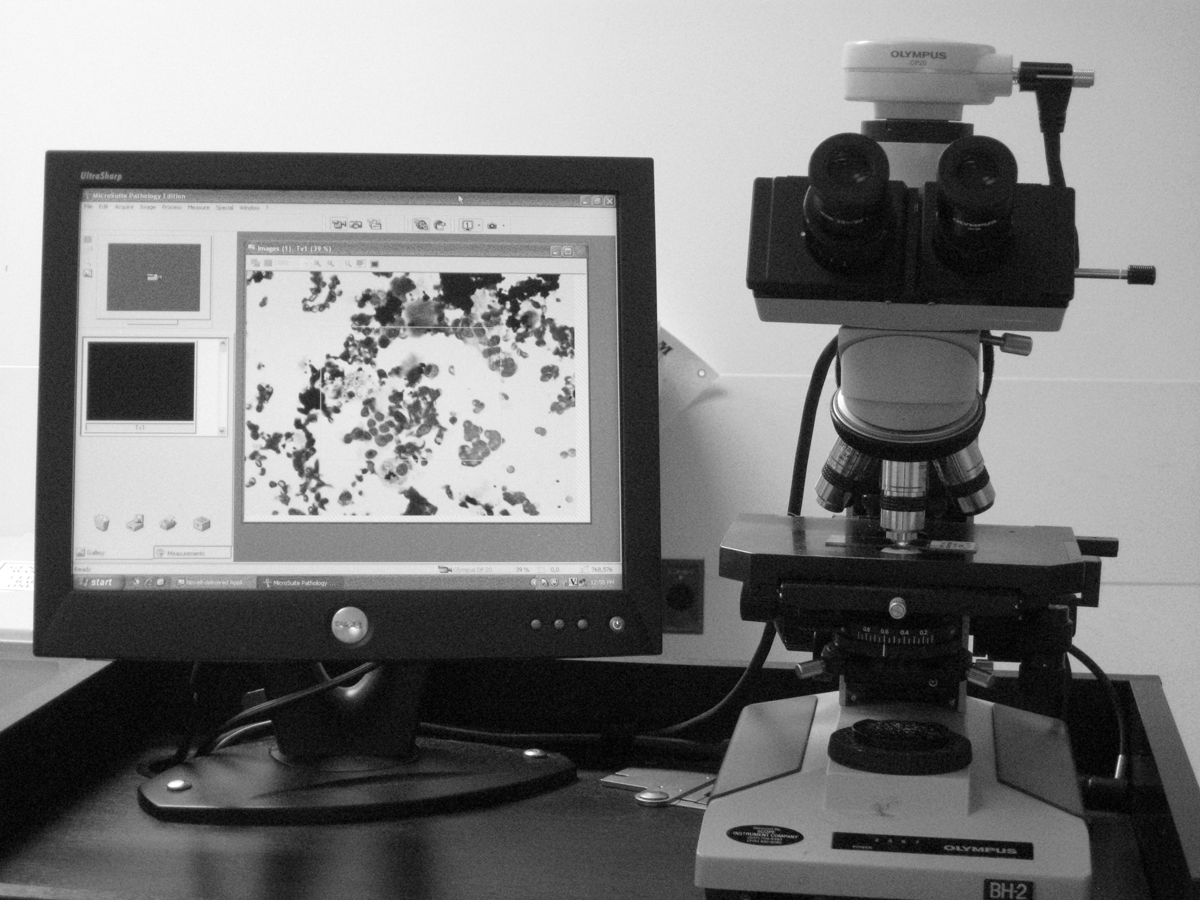
The telecytopathology digital system comprises of an Olympus camera and a monitor with microscope.
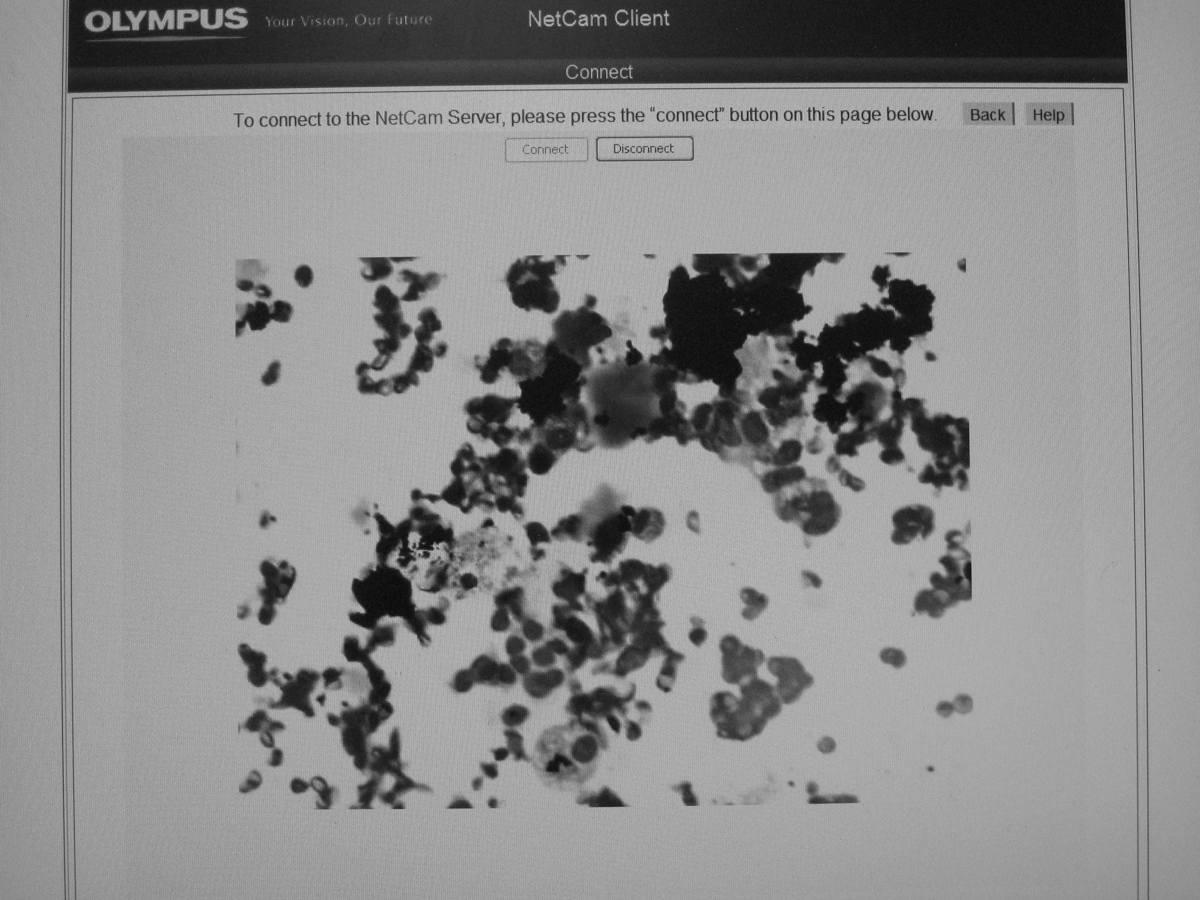
Benign thyroid consistent with goiter is shown in a patient with a thyroid nodule, viewed remotely on a computer screen using telecytopathology system (Diff-Quik).

Hürthle cell neoplasm is shown in a USGFNA in a patient with a thyroid nodule, viewed remotely on computer screen using telecytopathology digital system (Diff-Quik).
Different cytotechnologists with 12 to 20 years of experience and well conversant with the telecytopathology system operated the microscope at the remote site. The faculty cytopathologist (K.K.K.), with special interest in aspiration cytology of thyroid FNA, could not control the microscope or camera and interacted with the cytotechnologist via speaker telephone. Preliminary diagnosis was communicated to the endocrinologists and surgeons. The images were transmitted continuously as the cytotechnologist moved the slide on the stage and the pathologist could view on the screen what the cytotechnologist was seeing at the microscope.
Diagnostic categories that were used for preliminary on-site evaluation, and final cytologic diagnosis included unsatisfactory, benign, and suspicious/malignant. A satisfactory smear was defined as containing five or six groups of well-preserved cells; each group consisted of at least 10 to 15 cells. 7 Suspicious and malignant category were combined into one group for assessing accuracy rate. Suspicious category included all cases that were considered suspicious for follicular neoplasm, Hürthle cell neoplasm, and papillary carcinoma or cases with atypical features that were suggestive but nondiagnostic for malignancy. Two cytopathologists (K.K.K. and I.S., cytopathology fellow) performed the initial and final cytologic interpretations for the majority of the telecytopathology cases.
Accuracy was defined by agreement between the preliminary and final interpretations in the two groups. Cases were considered discrepant if the preliminary diagnostic category did not correspond to final diagnostic category. All discrepant case slides were reviewed to assess the cause of discrepancy. Impact of telecytopathology evaluation on the number of passes performed was also assessed.
Results
There were 100 consecutive cases of thyroid nodules (65 right sided, 30 left sided, and 5 isthmic) in 79 patients (10 men and 69 women; aged 7–76 years) that were evaluated by telecytopathology from February 1, 2010, to January 10, 2011.
Table 1 shows the final cytologic diagnosis on all thyroid nodules along with preliminary diagnosis rendered via telecytopathology. Of the 72 cases with initial telecytopathology diagnosis of benign, all were benign on the final cytology. Of the seven thyroid nodules with a preliminary telecytopathology diagnosis of suspicious/malignant, five were suspicious/malignant on final cytologic assessment and two were reclassified as benign adenomatous nodules.
Preliminary Onsite Telecytopathology and Final Cytologic Diagnosis
Of the 21 nodules with a preliminary telecytopathology evaluation of unsatisfactory, 4 (19%) were benign on final cytologic assessment. Unsatisfactory specimen revealed that three cases contained only histiocytes and the remaining 18 cases comprised of predominantly blood, rare follicular cells, and variable amount (moderate to none) of colloid. The accuracy rate of preliminary telecytopathology diagnosis was 94%.
Telecytopathology cases with discordant preliminary and final diagnosis are shown in Table 2. Two discrepant cases involved cellular adenomatous nodules that were initially interpreted as suspicious for follicular neoplasm because of cellular smears that revealed follicular cells but lacked colloid. On review inspissated colloid was identified in Diff-Quik-stained slides in both cases and cellblock section revealed variable-sized follicles filled with colloid in one of the cases.
Discrepancies Between Preliminary Telecytopathology and Final Cytologic Diagnosis
Of the 21 cases that were initially interpreted as “unsatisfactory,” Diff-Quik slides revealed histiocytes only in 3 cases and remaining cases comprised of predominantly blood, rare follicular cells, and variable amount (moderate to none) of colloid. On further review, four of these cases that were interpreted as “benign consistent with goiter” on final cytological assessment revealed more follicular cells, colloid, and histiocytes in one or more of the accompanying Papanicolaou-stained slides. Most of the Papanicolaou-stained slides in these cases were from additional passes performed after initial telecytopathology evaluation.
Table 3 shows the number of thyroid nodules in each of the diagnostic categories that underwent two or more passes. Of 72 benign thyroid nodules, 11 (15%) required more than two passes to obtain adequate material for cytologic diagnosis. In the unsatisfactory category all cases required more than two. Two of the seven cases (29%) in the suspicious/malignant category required more than two passes to render a cytologic diagnosis. In all “unsatisfactory” cases, including four cases that were reclassified with final cytologic diagnosis as “benign,” four passes were performed.
Number of Passes Performed in the Thyroid Nodules in Each of the Diagnostic Category
Discussion
Innovations in telepathology have made it feasible to procure pathology consultation remotely. Kaplan et al. 8 validated the use of telepathology for frozen section diagnosis with retrospective examination of frozen sections from various organ systems. The use of telepathology has included intradepartmental frozen sections and neuropathology subspecialty remote consultations. 9,10 Although increasing number of studies in the recent cytology literature have demonstrated the usefulness of dynamic and static telepathology systems to review cytology smears remotely over an Internet connection, dynamic systems appear to be more accurate when compared with static system. 2,11 –15
In the current study we performed initial on-site evaluation of USGFNA biopsies of thyroid nodules via a dynamic live and remotely operated telecytopathology system. To the best of our knowledge this is the first largest case series assessing the role of dynamic telecytopathology for rapid preliminary diagnosis of USGFNA of thyroid nodules. We demonstrated a high concordance between preliminary telepathology cytologic diagnosis and final cytologic diagnosis.
Discrepancies in telecytopathology between on-site preliminary diagnosis and final diagnosis were mostly minor and could be attributed to lack of material in the on-site slides that were evaluated. Unsatisfactory rate at the time of preliminary telecytopathology was 21%. However, identification of more follicular cells and histiocytes in cellblock material, cytospin slides, and Papanicolaou-stained slides at the time of final cytologic evaluation reduced the unsatisfactory rate to 17%. Our unsatisfactory rate was within the range of 2% to 21%, which has been previously reported. 16 At our institution most of the patients with “unsatisfactory” final diagnosis are followed up by clinical examination and ultrasonography at a 3- to 6-month interval, and a repeat FNA is performed only if the patient has risk factor for thyroid malignancy or ultrasonography shows suspicious findings. In our follow-up 2–8 months, none of the patients with “unsatisfactory” final diagnosis had a repeat FNA.
We encountered two false-positive cases that were initially suspected to be follicular neoplasms and received final interpretation of benign adenomatous nodules. Retrospective review of the slides in these case showed that there was inspissated colloid that was overlooked at the time of preliminary telecytopathology evaluation. In addition, the cellblock section in one case showed variable-sized follicles filled with colloid that further helped in reclassifying the lesion as a benign adenomatous nodule. Although we did not miss any malignant neoplasm at the time of preliminary cytologic evaluation, our study is limited by the modest number of malignant and suspicious cases. Additional studies using similar telecytopathology system are needed to evaluate on-site assessment of malignant and suspicious cases.
On-site telecytopathology evaluation accurately classified vast majority of the thyroid nodules as benign, and communication of these results to the patients immediately after the procedure alleviated patient anxiety. Four patients with suspicious or malignant diagnosis were appropriately triaged and referred to other specialties without further delay.
In our study, telecytopathology preliminary onsite evaluation limited the number of passes to two per nodule in 66% of cases. In 34% of cases more than two passes were performed due to an unsatisfactory telecytopathology preliminary evaluation of initial two passes. Adequate material for cytologic diagnosis was obtained in 51% (17 of 33 cases) of thyroid nodules that underwent additional aspirations. Prior studies have suggested four to six passes per thyroid nodule as the optimal number of passes needed to maximize diagnostic certainty, in the absence of immediate assessment of specimens by a cytopathologist. 16 –19 Based on our study, telecytopathology preliminary on-site evaluation minimized the number of passes required to procure adequate material for cytologic diagnosis to two passes in the vast majority of thyroid nodules. Thereby, patient discomfort associated with each additional pass was reduced.
Under current practice, staff cytopathologists alone are able to bill (Current Procedural Terminology code 88172, 88177) for passes performed during telecytopathology services as long as they participate in preliminary evaluation of these passes and assess the need for additional passes to obtain material for cytologic diagnosis and ancillary studies. The results of these preliminary evaluations have to be communicated to the physicians performing the procedure. Staff cytopathologists are legally responsible for all cases in which they provide diagnostic services, including telecytopathology. However, the importance of the cytotechnologist and cytopathologist working as a team for effectiveness of telecytopathology services cannot be overemphasized.
Telecytopathology allows for on-site evaluation at multiple sites by different cytopathologists and also facilitates consultation with a colleague in difficult cases. In this retrospective study we did not focus on the time spent by pathologist on each individual pass. However, based on experience, the estimated time that the cytopathologist spent evaluating each pass was 4 to 6 minutes.
In summary, we demonstrate that on-site telecytopathology preliminary evaluation for thyroid USGFNAs is highly accurate when compared with final cytologic evaluation. It assures sampling adequacy and decreases the number of passes that are needed to procure the adequate material. The low cost of the telecytopathology equipment (∼$6,000, excluding the microscope) makes it a cost-effective alternative in situations where distance and time constraints may preclude cytopathologists from rendering preliminary on-site evaluations at distant and multiple locations.
Footnotes
Acknowledgments
We would like to thank Ms. Cindy Steele, cytopathology laboratory supervisor for help with retrieval of data for this study.
Disclosure Statement
No competing financial interests exist.