
Abstract
Introduction
In patients with a major cardiac event, the first priority is to minimize time to treatment. For many patients, the first and fastest contact with the health system is through emergency medical services (EMS). 1 However, there are several factors such as patient-level and neighborhood-level factors that are associated with elapsed time in EMS. 1 In patients with acute coronary syndrome (ACS), total prehospital delay (symptom onset to hospital admission) was divided into two components: decision time (symptom onset to call for medical help) and home-to-hospital delay (call for help to hospital admission). Shorter total prehospital delays and decision times were associated with ST segment myocardial infarction (STEMI), recognizing symptoms as cardiac in origin, being married, symptom onset outside the home, and the presence of a bystander. 2 Shorter home-to-hospital delays were more likely among younger patients, those experiencing an STEMI, and patients reporting a greater number of symptoms. Initial contact with EMS was related to shorter total delays and decision times. Patient characteristics associated with longer time to reperfusion in subjects with acute myocardial infarction (AMI) included female gender, age ≥75, tachycardia at presentation, history of diabetes mellitus, coronary artery bypass graft, or congestive heart failure, and presentation at night, including on the weekend and weekdays. 3 Factors associated with shorter time to reperfusion included arrival at the emergency department (ED) by ambulance and the presence of cardiogenic shock on arrival.
Delay in seeking medical care after symptom onset in patients with an AMI is related to increased morbidity and mortality. According to data from the Worcester (Massachusetts) study, mean delay times have remained essentially unchanged during the past two decades (4.1–4.6 h). 4 Approximately 45% of patients with AMI presented within 2 h of acute symptom onset, whereas an additional one third presented from 2 to 6 h after the onset of acute coronary symptoms. Advancing age and history of either diabetes or AMI were associated with prolonged delay. Compared with patients arriving within 2 h of symptom onset, those with prolonged prehospital delay were less likely to receive thrombolytic therapy and primary percutaneous coronary angioplasty within 90 min of hospital arrival. A large proportion of patients with AMI continue to show prolonged prehospital delay. In the 14 countries participating in the Global Registry of Acute Coronary Events project, the average and median delay times were longest in patients with non-STEMI (6.1 and 3.0 h, respectively) followed by patients with unstable angina (5.6 and 3.0 h) and those with STEMI (4.7 and 2.3 h). 5 Approximately 41% of patients with STEMI presented to the 94 study hospitals within 2 h of the onset of acute coronary symptoms; this compared with approximately one-third of patients with non-STEMI and unstable angina. In patients with STEMI, duration of prehospital delay was inversely related to the receipt of thrombolytic therapy. A large proportion of patients continue to exhibit prolonged delay in seeking medical care after the onset of acute coronary symptoms and remain in need of targeted educational efforts to reduce extent of delay.
Despite advances in the treatment of STEMI, the mortality rate before any therapy is administered is high, with half of all fatalities occurring within 2 h of symptom onset. 6 Time factors are essential in the success of fibrinolysis and subsequent coronary intervention. Current treatment options, including the timely use of prehospital fibrinolysis, have reduced the overall 1 month mortality. 7 The results of the Vienna STEMI registry suggest that, within 2 h of symptom onset, thrombolysis should be administered preferably prehospital, if primary coronary angioplasty cannot be performed within 90 min of the first medical contact. 8
A large body of evidence demonstrated the benefits of prehospital electrocardiogram (ECG) for decreasing delay to treatment in patients with STEMI, 9 –15 with an ∼10 min decrease in door-to-drug time and 15–20 min decrease in door-to-balloon time. 16 Moreover, studies have shown further reductions in door-to-balloon time when prehospital ECGs are used to activate the catheterization laboratory while the patient is en route to the hospital. 17,18 Patients' transfer seeking for best treatment does not increase the risk of adverse events both in case of AMI 19 and after cardiac arrest. 1
International guidelines 20 as well as other consensus and scientific statements 21 therefore recommend that EMS acquires and uses prehospital ECGs to evaluate patients with suspected ACS, and many communities are implementing prehospital ECG programs. In this study we therefore aimed to report preliminary results achieved with a single telecardiology “hub” active 24/7 providing prehospital ECG for a region-wide public EMS. We also report on the technical requirements, logistics and manpower of a region-wide telecardiology prehospital network, demographics of patients screened by telecardiology prehospital ECG, symptoms reported, and ECG findings.
Methods
The Apulia region-wide prehospital ECG telecardiology program involved 233,657 patients from all over Apulia (19,362 km2, 4 million inhabitants; Fig. 1), who called the public regional free EMS telephone number “118” between October 2004 and March 2010. The 118 is a public, free service for general, either medical or surgical, emergencies, whose aim is an immediate diagnosis of critical diseases, to avoid ED delay to diagnosis. Final hospitalization is disposed by crews' physicians and the 118 district center, connected by mobile phone; direct admission to a critical care unit is arranged according to level of care. In the event of normal findings, patients are discharged from the ambulance and not transported at all. In Italy, 118 crews usually include a physician skilled in emergency medicine and/or nurses.

Apulia and district “118” emergency medical services (EMSs) centers with corresponding logistics: each 118 EMS point was given a telecardiology electrocardiogram (ECG) recorder and all 118 crews (physicians, nurses, and paramedics) underwent specific training. All EMS points depend on the same public regional healthcare service. The single telecardiology hub serving the entire region is located in the capital city (Bari).
One hundred sixty-five crews of the 118 EMS, 27 first-aid points, 33 summer first-aid points, and 12 medical vehicles involved in this project were equipped with apposite devices for recording and telephone transmission of 12-lead ECG (CardioVox P12 heart-line receiving system; Aerotel, Holon, Israel); the device does not directly show ECG records, so ECG cannot be immediately seen by the 118 crew members (paramedics and physicians), although the ECG may be sent back and visualized on a smart phone. Data recorded by the 118 personnel is transmitted by mobile phone to a single regional telecardiology hub center where a cardiologist available 24/7 promptly reports the ECG (Fig. 2) and briefs on-scene EMS personnel and the EMS district center. Admission to a coronary care unit or to cat lab for primary coronary angioplasty is arranged after this consultation. The Regional Health Care Department is completing the regional network for primary coronary angioplasty or prehospital thrombolysis where primary coronary angioplasty is not available in a timely fashion.

CardioVox P12 ECG recorder device: the device does not make it possible to view the ECG, which is transmitted by telephone support to the telecardiology central hub. Here a cardiologist available 24/7 reports the ECG and talks to the on-scene EMS crew and EMS district center, to decide about hospitalization.
Telecardiology support and hub center facilities are provided by Cardio-on-line Europe S.r.l., a telemedicine company-certified UNI EN ISO 9001:2008 (quality certification) and UNI CEI ISO/IEC 27001:2006 (security data certification). The telecardiology hub center serving the entire regional territory, operative 24/7, has one or two cardiologists promptly available for ECG reporting, 12 computer terminals, 25 telephone lines, 2 call center operators active 24/7, and an emergency power system in case of electrical power outage (Fig. 2).
All center services and the entire network are shielded from virus threats by a combination of hardware and software firewalls, and a comprehensive antivirus suite capable of real-time scanning and updates, in addition to software back-up procedures. A comprehensive network management program ensures that all systems have real-time updates and that the latest security patches are installed as soon as they are released.
All data are electronically stored onto computers using a unique identification number for center and individual, under the provisions of the Italian Privacy and Personal Information Protection Act (D. Lgs. 196/2003).
Regional EMS and telecardiology provider made a preliminary agreement on indications for ECG recording: presence of chest pain or epigastric pain, breathlessness, palpitations, dizziness/fainting, or any suspected acute cardiovascular disease.
ST segment elevation was considered significant for MI according to the American College of Cardiology/American Heart Association (AHA)/European Society of Cardiology criteria published in 2000 (new or presumed new ECG alterations: ST segment elevation at the J point in two or more contiguous leads with cutoff points ≥0.2 mV in leads V1, V2, or V3 and ≥0.1 mV in other leads). 22
The study was approved by the Regional Health Care Authority.
Statistical Analysis
Continuous variables were expressed as mean value±standard deviation and categorical variables as a percentage. Data were preliminarily cleaned and screened before analysis with SSP Software.
Results
Of 233,657 patients enrolled, 48.5% were male and 50.6% were older than 70 years. The number of patients screened with prehospital ECG by EMS rose constantly between 2004 and 2010. Prehospital ECGs for suspected acute heart disease were 13,416 in the first year, 28,207 in 2005–2006, 40,219 in 2006–2007, 48,554 in 2007–2008, 62,372 in 2008–2009 (Fig. 3). Telecardiology hub callings for prehospital ECGs were distributed as follows: 36% day, 29% afternoon, and 35% night.
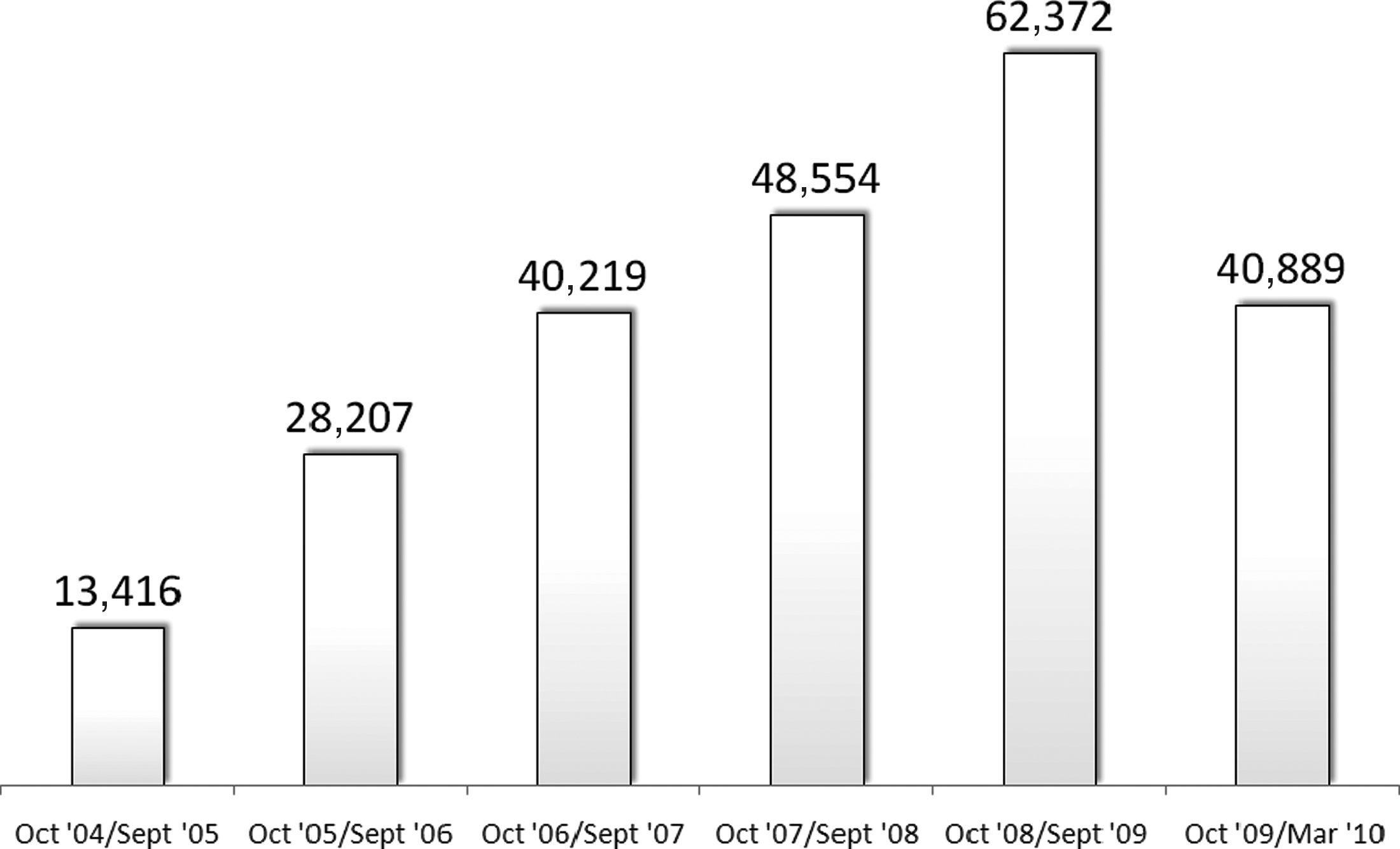
Prehospital ECGs received by telecardiology hub per year between 2004 and 2010 (for 2010, the figure is for 6 months only).
Age distribution for prehospital ECGs was 0–19 years, 2%; 20–29 years, 3%; 30–39 years, 7%; 40–49 years, 10%; 50–59 years, 12%; 60–69 years, 16%; 70–79 years, 25%; 80–89 years, 20%; >90 years, 5% (Fig. 4).

Prehospital ECGs per age class; about 50% are elderly people over 70 years.
Patients screened by EMS complained of typical chest pain in 17.7% of cases, atypical chest pain in 8.4%, breathlessness in 9.8%, epigastric pain in 9.3%, palpitations in 7.4%, dizziness/syncope in 22.9%, and other symptoms in 24.5% (Fig. 5).
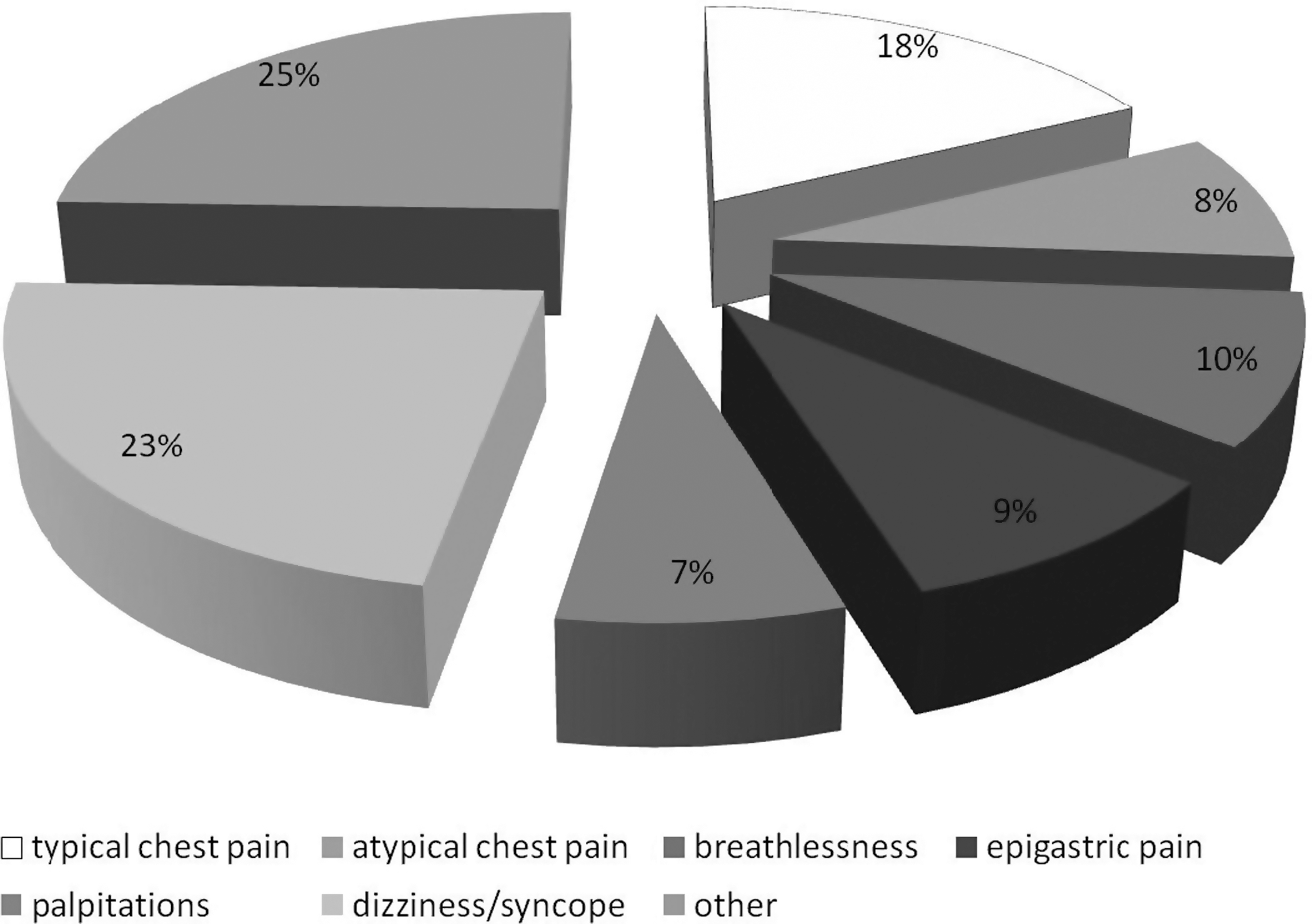
Symptoms reported by patients who underwent prehospital ECG.
Fifty-five percent of prehospital ECGs were unremarkable, without signs of any acute heart disease (Fig. 6); the remaining 45% showed signs suggesting ACS in 18%, arrhythmias in 20%, and minor findings (premature contractions, left ventricular hypertrophy, etc.) in 62% (Fig. 7).
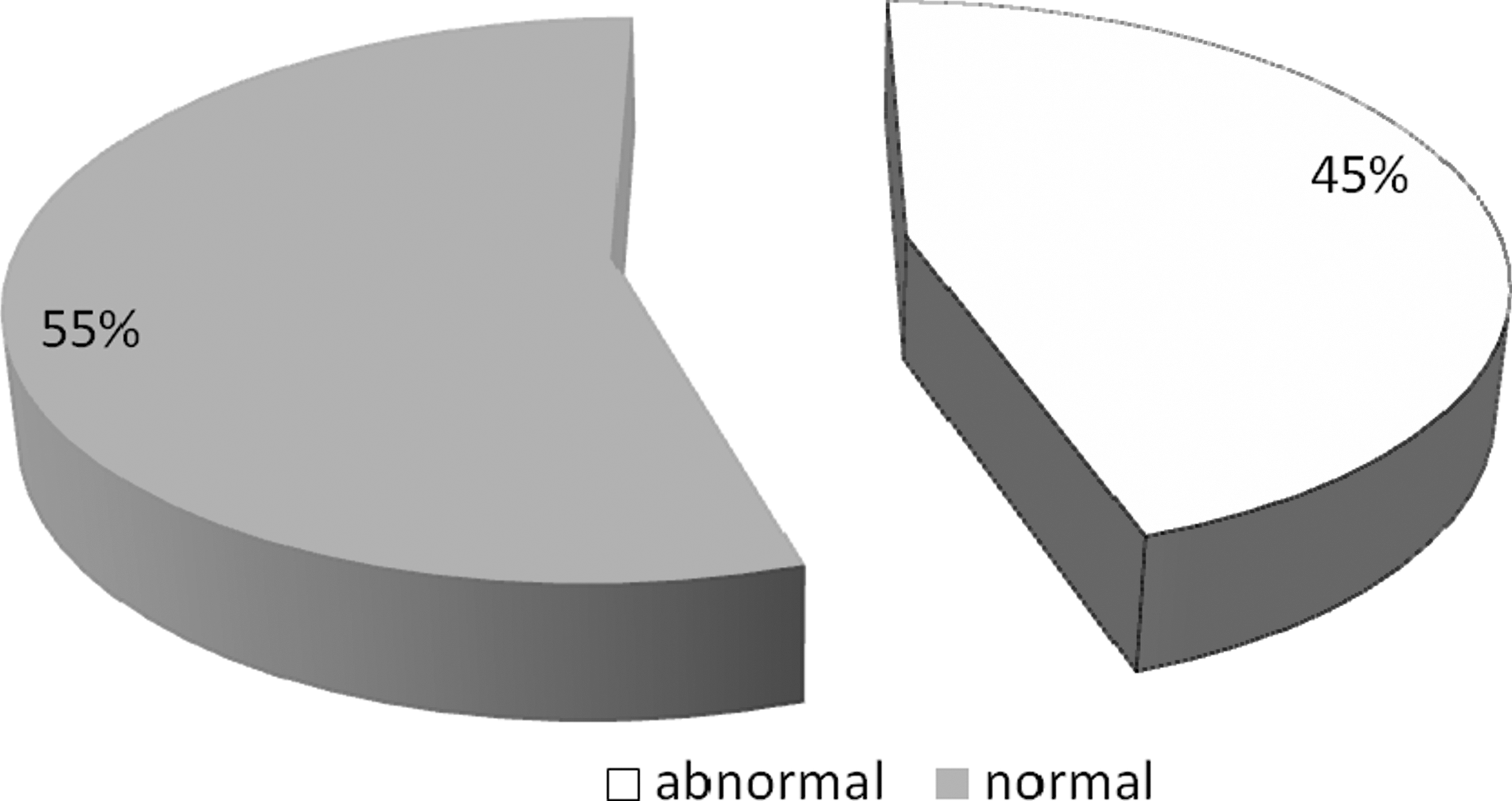
ECG findings in subjects with suspected acute heart disease; 55% had a normal ECG.

Suspected heart disease in subjects with a nonnormal prehospital ECG. In 18% of cases, the suspected diagnosis based on prehospital ECG findings was acute coronary syndrome, and in 20% a significant arrhythmia was present (supraventricular or ventricular arrhythmia or atrioventricular significant block).
In case of clinically suspected ACS, ECG findings were normal in 77% of patients (Fig. 8): 74% of subjects with acute chest pain were screened with a prehospital telecardiology ECG within 30 min of onset of symptom.

ECG findings in subjects with symptoms suggesting acute myocardial infarction (typical chest pain).
Preliminary data on analyzing prehospital ECG findings in patients discharged with a diagnosis of STEMI in 2007 showed a negative ECG in 13% of cases, whereas the remaining 87% showed abnormal ECG findings; ST segment was elevated in 38% of patients.
Discussion
In this article, we report 6-year results, technical requirements, logistics, and manpower of a regional prehospital ECG network with a single telecardiology hub for public EMS in Apulia, Southeast Italy. In line with Italian legislation, the regional EMS is the sole provider of EMS for the entire population of the whole region. All ambulances and medical cars of the 118 depend on the regional EMS and are coordinated by five district centers (Bari, Lecce, Taranto, Foggia, Brindisi). This provides a unique opportunity to standardize protocols and equipment for all crews of the 118. All ambulances and medical cars of the 118 were given the same telecardiology ECG recorder device; all crews of the 118 underwent the same training for the use of CardioVox P12 and were supported by a single telecardiology hub, in line with the same regional operational protocol.
Implementing a single regional telecardiology hub is crucial to delivering a high-level standardized prehospital ECG analysis and to limiting costs. A minimal staff of 20 cardiologists and 20 phone-call operators were required to provide a 24/7 telecardiology service. The call center Hub works using two day shifts (8 a.m. to 2 p.m., 2 p.m. to 8 p.m.) and one night shift (8 p.m. to 8 a.m.). About 24/7 computer assistance is also needed to avoid software system bugs. The mean workload involved a phone call approximately every 8.4 min in the last year. Workload peaks were observed in winter, during flu spread, and summer, during holiday season. 23
Clinical results and fields of application of telecardiology support for public EMS were previously published in several papers. 24,25 Prehospital ECG screening with telecardiology support reduced the rates of wrong or delayed diagnosis in elderly patients with AMI and atypical presentation. 25
In subjects with STEMI who called 118, 45% were diagnosed within 30 min of onset of chest pain, and 41% between 30 min and 3 h. 23 Sixty percent of patients with STEMI were diagnosed by prehospital 118 ECG in towns without an immediately accessible coronary care unit, thus particularly benefiting from an immediate diagnosis because of needing an immediate time-wasting transfer to a distant cath lab; 47% of these STEMI patients from small towns or in peripheral mountain areas were diagnosed within 30 min of onset of chest pain, and 87% within 3 h, with time to diagnosis similar to that in bigger towns.
In 2008, the AHA published a statement for the “Implementation and Integration of Prehospital ECGs into Systems of Care for Acute Coronary Syndrome” 21 ; in that paper, some of the principal community models implementing prehospital ECG programs are reported.
The Boston EMS program, 26 one of the first in the United States, involves municipal trained paramedics; patients with definite STEMI or possible STEMI are triaged to the closest coronary angioplasty hospital, and the former are brought directly to the catheterization laboratory and the latter are evaluated in the ED. The emergency physician decides whether to activate the catheterization laboratory on the basis of the paramedic interpretation while the patient is en route to the hospital. The Boston EMS program covers a relatively small geographical area (<50 mi 2 ) with 60–70 municipal paramedics, and private EMS providers do not participate in the program.
In contrast, the Los Angeles County EMS program includes all EMS providers, an area of >4,000 mi 2 with ∼2,500 paramedics working for 27 agencies. 27 The Los Angeles County EMS program therefore relies on computer algorithm interpretation that identifies ACUTE MI to prompt EMS transporting of patients to the closest coronary angioplasty center (or STEMI receiving center). The emergency physician decides whether to activate the catheterization laboratory on the basis of the computer algorithm interpretation while the patient is en route to the hospital. A few hospitals in Los Angeles County have started to pilot the feasibility of transmitting prehospital ECGs for physician interpretation.
The Reperfusion of AMI in North Carolina Emergency Departments (RACE) Investigators implemented a statewide approach to improve timeliness of reperfusion therapy for patients with STEMI. 28 However, the RACE program did not have standardized procedures for when to acquire a prehospital ECG, who should interpret the prehospital ECG, and how to integrate the prehospital ECG with systems of care. Each hospital and region decided how to interpret and integrate the prehospital ECG based on available resources, geography, and decisions by regional leadership.
The Ottawa citywide system, which included one coronary angioplasty center and four noncoronary angioplasty hospitals located within 7 mi of the cath lab center, reported their 1-year experience in 344 patients with STEMI. 29
Other district-wide programs for implementation of prehospital ECG were reported from Aarhus 13 and Vienna 8 in Europe. In both cases, prehospital ECG support significantly improved times to reperfusion, although both models are limited to a single district.
The 2008 AHA statement also highlights the pros and cons of different presently available models for interpreting prehospital ECGs. Computer algorithm interpretation of prehospital ECG is rapid and easy and does not usually require wireless network or technology for ECG transmission; however, false-positive and false-negative rates are higher than with physician interpretation. Paramedic interpretation is also rapid and easy; however, it usually requires intensive education and quality assurance programs and is more complex in communities with multiple EMSs, providers, and agencies. Wireless transmission and physician interpretation theoretically have the lowest rate of false-positives and false-negatives, even though new technology is required for EMS providers and hospitals. Medical oversight can provide guidance on destination hospital and treatment en route.
The Apulia 118 network fairly fits with the AHA statement because of several positive conditions: the entire 4 million inhabitants in the 20,000 km2 region shares a single EMS and can therefore rely on a single telecardiology hub. This allows standard protocols for prehospital ECG and standard management of patients after prehospital diagnosis.
Other prehospital ECG models, despite a brilliant reduction in time to reperfusion, suffer from some limitations. The Boston model, relying on interpretation by paramedics, sometimes requires a time-wasting second-step medical confirmation of AMI. The Ottawa model shares the same limitations and both are limited to a single big city area.
On the other hand, the Los Angeles model is limited by software misinterpretation and EMS/hospital fragmentation. The North Carolina model seems to be more in line with the AHA statement on prehospital ECG; however, this program did not have standardized procedures for when to acquire a prehospital ECG, who should interpret the prehospital ECG, and how to integrate the prehospital ECG with systems of care. Each hospital and region decided how to interpret and integrate the prehospital ECG based on available resources, geography, and decisions by regional leadership.
Other prehospital ECG programs on ACS management were held in Italy. Ortolani et al. lowered treatment delay from 236 to 146 min, using prehospital ECG 30 ; in a single-city experience, mean door-to-balloon time was reduced from 76 to 47 min and in-hospital mortality from 6.8% to 5.4%. 31 In every case, prehospital ECG significantly reduced delay to treatment, which has been reported as one of the principal outcome determinants in coronary heart disease, both in case of primary coronary angioplasty 32,33 and in case of fibrinolysis. 34
The Apulia prehospital ECG program was particularly effective in reducing time to diagnosis in peripheral mountain areas, where cardiologist assistance is usually not immediately available owing to logistical limitations. 35 The Apulia project covers the entire regional territory, but there is much work to do to reduce not only time to diagnosis but also time to reperfusion.
However, delay to treatment is still significant in developed countries as well. In recent studies, door-to-balloon times for transfer patients undergoing primary coronary angioplasty in the United States rarely achieved guideline-recommended benchmarks. 36 The data from the National Registry of Myocardial Infarction-4 showed a geometric mean time of 83–103 min from the onset of symptoms to hospital arrivals.
Future policy measures are therefore needed to encourage EMS, hospitals, and healthcare systems to adopt and maximize the full potential of prehospital ECG and telecardiology. The Apulia prehospital single telecardiology hub may deserve to feature in the international debate on possible models of prehospital ECG implementation; it is particularly suitable for countries or regions with a single EMS and healthcare system.
Limitations
This is an observational nonrandomized study reporting preliminary results of a model of prehospital ECG screening with telecardiology support in a region-wide EMS network. These preliminary data need to be confirmed in larger randomized trials. In particular, it is necessary to investigate whether prehospital ECG examination with telecardiology support may be helpful in reducing costs and adverse events in subjects with ACS and in evaluating exact sensitivity and specificity of the telecardiology approach in larger populations.
Conclusion
A regional single telecardiology hub providing prehospital ECG for a sole regional public EMS sets an example of a prehospital ECG network optimizing quality of ECG report and uniformity of EMS assistance in a large region-wide network.
Footnotes
Acknowledgments
Dr. Brunetti, Dr. De Gennaro, and Dr. Pellegrino cooperated with Cardio-on-line Europe S.r.l. as consultants. The authors thank Dr. Ambrogio Aquilino and Dr. Vito Petrarolo (from Apulia Health Agency, Bari, Italy), who helped by providing the follow-up data. This work was performed at the Cardiology Department, University of Foggia, Foggia, Italy.
Disclosure Statement
No competing financial interests exist.