
Abstract
Rural American Indian veterans have unique healthcare needs and face numerous barriers to accessing healthcare services. Over the past decade, the Department of Veterans Affairs in conjunction with the University of Colorado Denver has turned to the promising field of telemental health to develop a series of videoconferencing-based clinics to reach this vulnerable population and improve mental healthcare services. The ongoing development, implementation, and expansion of these clinics have been assessed as part of a program improvement. The outcomes of these assessments have been documented in a series of published articles, controlled studies, program and case reports, and model descriptions. This article summarizes a decade of experience with the American Indian Telemental Health Clinics, the clinic model, and the literature arising from these clinics and presents lessons learned while establishing, maintaining, and evaluating these clinics. The ability to tailor the clinics to individual sites and cultures and to provide various services has been critical to the operation of the clinics. Culturally specific care through culturally knowledgeable providers, onsite tribal outreach workers, and collaboration with community services has proven essential in operating the clinics, as well as building rapport, trust, and engagement with the target patient population. It is hoped that the lessons learned and practices presented here can not only assist others working to improve the care for rural Native veterans but also serve as a model in the use of telemental health services for improving care and access to rural veteran and non-veteran populations.
Introduction
Veterans from the Native American Indian, Alaska Native, native Hawaiian, and Pacific Islander populations have an exemplary tradition of military service and sacrifice. Serving at the highest rate per capita of any ethnic group in the U.S. Armed Forces, 1,2 they are disproportionately impacted by the consequences of service, including higher rates of disorders related to combat exposure (e.g., posttraumatic stress disorder [PTSD]). 3 The American Indian Vietnam Veterans Project, the largest and most comprehensive community-based epidemiology study ever conducted on this population, documented rates of PTSD (31% current, 59% lifetime) and alcohol abuse and dependence (72% current, 84% lifetime) significantly higher than any other ethnic groups. 3 This study along with subsequent research demonstrated substantial unmet need for PTSD and other mental health treatments for American Indian veterans along with additional barriers to care involving resources, culture, and geography. 4 Native veterans are the most rural of all veteran groups, with nearly half residing in rural locations on tribal or Alaska Native lands. 5 Challenges of these potentially harsh environments include access to care, healthcare provider recruitment and retention, access to culturally appropriate care, underfunded healthcare resources, and often geographically isolated and dispersed communities. 6
In 2001, to address the mental health needs of rural American Indian veterans, the Department of Veterans Affairs (VA) in partnership with the University of Colorado Denver's Centers for American Indian and Alaska Native Health (CAIANH) turned to the promising and expanding field of telemental health. The American Indian Telemental Health Clinics were initially established with a pilot clinic in April 2002, including the VA's VISNs 19 & 23, CAIANH, and the Rosebud Sioux Tribe, to improve the mental healthcare of rural American Indian veterans via community-based telemental health services. 7 The success of the initial clinic catalyzed the expansion of this model to multiple active and developing clinic sites serving tribes in Idaho, Montana, South Dakota, and Wyoming. The ongoing development, implementation, and expansion of these clinics were assessed as part of a program improvement process. The outcomes of these assessments have been documented in a series of published articles, encompassing controlled studies, program and case reports, and model descriptions. The intent of this article is to summarize the American Indian Telemental Health Clinics, the clinic model, and the literature arising from these clinics and present lessons learned while establishing, maintaining, and evaluating these clinics.
Materials and Methods
The clinics represent an internal VA collaboration between VISNs (19 & 23), VA Medical Centers paired with individual clinic sites, and the VA Office of Rural Health's Native Domain. External partners include the CAIANH and a mix of community-based partners determined by the patient sites, which include tribal communities, tribal veterans centers, Indian Health Service (IHS) facilities, and tribally run medical systems.
The clinics follow a shared model where a VA-credentialed psychiatric practitioner at the CAIANH in Denver provides telemental health services to a patient site based on or near a rural reservation. Providers have experience with Native veterans and/or cross-cultural populations. They receive training, education, and orientation about Native communities, Native veterans, and the specific tribe with which they will be working. Training is completed via written and Web-based trainings, readings, community site visits, and work with cultural facilitators. Each patient site has different structural and organizational configurations determined by the resources and needs of the local communities. For example, some are co-located in VA community-based outreach clinics, others in IHS or tribal facilities. The telemental health services usually occur on a weekly or bimonthly basis depending on the needs of the patients. Services offered include diagnosis, assessment, case management, and treatment encompassing medication management and psychotherapy (group, individual, and family), and linkage to other VA services and benefits.
Medication is prescribed remotely and delivered via mail to the patient using the VA's electronic medical record system. Labs, diagnostic tests, and assessments are obtained from facilities located near the patient as available through partnership with local healthcare organizations such as the IHS or tribally run systems. PTSD is the most common mental health diagnosis seen in the clinics, followed by substance use disorders. The clinic patient population is characterized by high psychiatric and medical comorbidities, comparable to other clinical rural veterans populations. 8 In general, the clinics follow a progressive model of engagement and treatment (see Fig. 1 for PTSD) that encourages family and community involvement, with interventions tailored to individual patient needs. This model is intended for long-term treatment engagement as opposed to a consultative model often found in other telemental services.

Progressive psychotherapy posttraumatic stress disorder (PTSD) treatment model of the American Indian Veteran Telemental Health Clinics. TOW, Tribal/Telehealth Outreach Worker; TVR, Tribal Veterans Representative; CBT, cognitive behavioral therapy; CPT, cognitive processing therapy.
The clinics use a variety of methods at the patient site to provide culturally specific care. These include the use of Tribal/Telehealth Outreach Workers (TOWs), partnership with the Tribal Veterans Representative (TVR) program, and collaboration with local traditional healers. The patient site is run administratively by the TOW who performs critical patient outreach and community liaison functions. TOWs employed by the VA are generally veterans and members of the tribes for which they serve. Their background facilitates them in fostering trust and rapport with Native veterans and reduces cultural barriers to engagement in treatment. Their duties include assisting enrollment of Native veterans in the clinics, scheduling intakes and appointments, orienting patients on the use of videoconferencing, troubleshooting equipment, and coordinating community resources. TOWs work closely with the clinic providers, giving guidance on cultural and community issues relevant to a patient's care.
TOWs collaborate with TVRs who are appointed by their tribal councils. TVRs function to help rural Native veterans enroll, obtain benefits and care, and navigate the VA system. The TOWs attend TVR training and work closely with TVRs to link clinic patients with wider VA and veterans resources. This facilitation builds engagement with the telemental health clinic patients and local tribal veteran community. Each of the clinic sites has collaborative relationships with traditional healers from the local community. These collaborations occur through both formal and informal processes providing opportunities for interested patients to utilize traditional approaches for treating mental health conditions. The Sweat Lodge Ceremony is the most used traditional treatment, although a range of activities have been undertaken including talking circles, blessings, and smudgings. 9
Figure 2 reflects the key components of the clinic model, depicting (1) VA-based providers with expertise in PTSD, (2) VA system and technology infrastructure with a mix of community organization partnerships at the patient site, and (3) cultural facilitation of care through community liaison and collaboration.
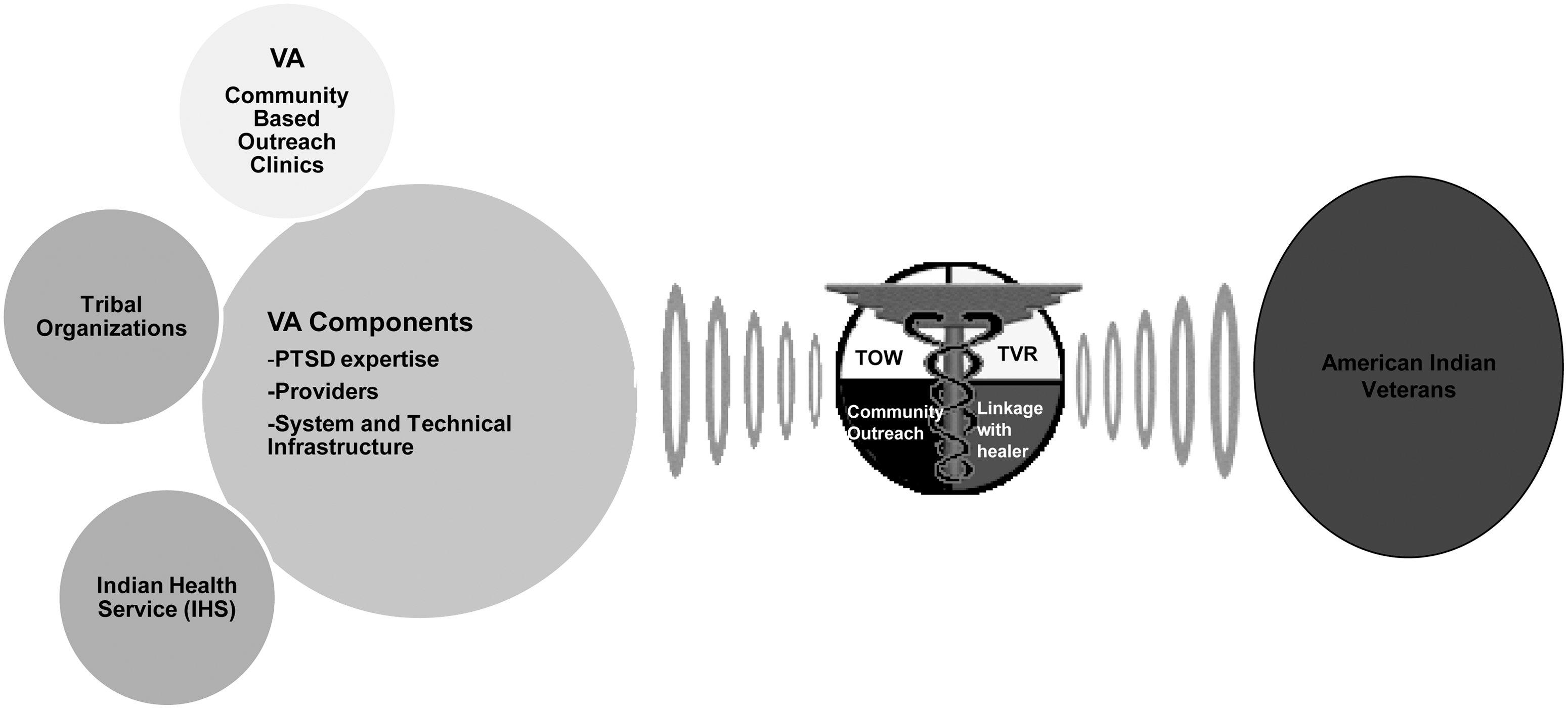
Model of American Indian Veteran Telemental Health Clinics. VA, Veterans Affairs.
Results
The initial clinic began as a pilot on the Rosebud Sioux Reservation and represented collaboration between five different organizations. 7 The first patients were seen in April 2002, but planning for clinic implementation began in 2001, with concept exploration beginning in 1999. Currently, the Denver-based clinics have eight active sites serving 14 different tribes. An additional three non–Denver-based clinics patterned after this model are run directly from regional VA medical centers in the Northern Plains. From inception in April 2002 through February 2011, there have been approximately 970 clinic days held in the Denver-based sites. Of these, 185 individual American Indian veterans have received an initial psychiatric assessment. There were 3,220 individual follow-ups and 440 group sessions (ranging from one to six veterans, an average attendance of two to four participants per group, with approximately 15–20% of patients attending groups at sites where groups were available), representing a total of 3,845 sessions and 4,610 patient contacts. Approximately 5–10% of the individual sessions involved the participation of patient family members.
Since inception, the clinics have provided context and material for manuscripts addressing their implications for rural telehealth and underserved populations. Table 1 lists these publications, describes them, and highlights a summary of their lessons and findings. The manuscripts' main foci can be broadly categorized as addressing administrative/logistical, clinical, or cultural/process issues. The administrative and logistical manuscripts present the clinic implementation process including challenges and successes, key issues (e.g., jurisdiction on civil commitments), examined impact on patients, and attempted to characterize the general clinic framework for further refinement and dissemination. Articles describing processes explore cultural issues and successful cultural adaptations in the clinics. In addition to published articles, other products focused on telehealth with underserved populations include Web-based trainings, protocols, and a procedures template. 10
Telemental Health Clinics' Published Articles and Evidence
Several key administrative lessons have been learned from these clinics and are summarized in Table 2. One of the most important is that multi-organization collaborations are essential, possible, and desirable in order to implement care for special populations in remote environments. The right configuration of organizational partners is critical with clear definitions of roles, responsibilities, and communication processes. Initial identification of the right partners needs a systematic progressive approach, 11 with individual site partnerships determined by environment, resources, and needs at the local level. Collaborations have ranged from clinics of one to two key partners (e.g., VA partners, CAIANH) to five to six organizational collaborative partners (e.g., VA, IHS, Tribal). 7,11
Lessons Learned from American Indian Veteran Telemental Health Clinics
The administration of the overall service has required a consistent structure and framework that is flexible and can be tailored to individual sites. This administrative framework creates a “holding” environment for all the clinics and addresses the challenge of meeting regulatory and technical requirements of multi-organizations. Some of the multi-organizational requirements are static (e.g., licensure and credentialing), whereas others are dynamic and evolving (e.g., technology). Local champions, a common telehealth literature theme, 12,13 have been important for clinic success, along with buy-in and advocacy of the leadership from all partner organizations. The TOW's administrative role in interfacing with tribal systems cannot be overemphasized with the TOW acting as a facilitator and translator between the tribal and federal/university systems.
The clinical feasibility of these services has clearly been established 7,11,14 along with high degrees of patient and provider acceptance and satisfaction. 15 The diagnostic reliability of videoconferencing for American Indian veterans has been supported by a randomized controlled trial. 16 An examination of longitudinal clinical data from a subset of these clinics has shown a significant global increase in medical service utilization associated with the clinics. 8 This study also helped to depict the high psychiatric and medical comorbidities that impact clinic patients, consistent with other research on Native veterans and rural veterans, 1 emphasizing the importance of medical care coordination. As in previous studies, 17,18 patients in these clinics exhibit dual VA–IHS utilization and use of traditional treatments. Patients choose to receive care from the source they perceive most experienced to treat their specific complaint. Although formal methods of care coordination are part of clinical protocols, coordination appears most effective when individual clinicians work directly with the patient and the patient's other providers. The VA electronic medical record system, based at each VA medical facility that providers can access remotely, is an invaluable tool for care coordination and communication within the VA since the telemental health clinic providers are based in Denver, and patients receive their medical care and ancillary psychiatric care (e.g., residential treatment) at the nearest VA facility.
Experiences around mental health emergencies during the early years of these clinics helped to further pilot and standardize processes for emergency management critical for service implementation. 19 –22 The overarching principles involve identifying patient site emergency management resources and processes and adapting them into the clinic protocols with clear delineation of local partners' roles and responsibilities for handling psychiatric emergencies. 20 This follows the principle of creating a consistent yet flexible administrative structure, a “holding” environment, for the clinics to adapt to community resources and organizational changes.
Some of the most important lessons to emerge from these services are the recognition of the impact that videoconferencing has on patient–provider relationships and the clinical process, including the importance of modification to cultural considerations. 23 Individual patient–provider relationships are critical to achieve successful treatment outcomes, but the larger relationship with the local tribal community is equally important. Without respect, trust, and community alliance the clinics are unable to function, and patients are not comfortable engaging in treatment. The TOWs are vital in this area, with their most important function to facilitate community relationships, build rapport, and foster the reputation of clinics. Additionally, the use of the TOWs and the traditional healer collaboration illustrate the clinics' intention to work in partnership and incorporate the clinic within the community context. 9
In patient–provider interactions, a critical recognition has been that telemental health has its own sets of assets and liabilities as a medium, as does seeing patients "in-person." Understanding the specifics of these is an ongoing process as both clinical experience and data accumulate. The need for specific as well as general cultural adaptations for clinics using this model has been reviewed in detail previously. 22,23 This encompasses principles around assessing patients' experiences, regard, and reactions to technologies and adapting clinical styles as appropriate to local cultural styles. In general, liabilities for clinical telemental health include the lack of physical presence, which can impact patient rapport and situational assessment, and the perception of distance during clinical interactions. As implied in the results of the reliability study, this may make work with internalizing diagnoses (e.g., depression) more challenging and require clinicians to adapt a more active personal style. 16 Benefits for clinical telemental health are increased perception of confidentiality in small communities, enhancement of observing ego, and the increased feeling of personal space/safety for the patient. 7,14,23 This feeling of space at times can be an asset in building initial rapport, trust, and engagement. This is salient for rural Native veterans with PTSD whose past experiences with governmental systems may create ambivalence around further treatment. 24 –26 Regular provider visits to the reservations help enhance and maintain rapport with clinic patients and the community.
Discussion
Although there is not a universally accepted definition for “best practice,” one reasonable progressive model for best practices defines the highest level of “best practice” as “… a specific action or set of actions exhibiting quantitative and qualitative evidence of success together with the ability to be replicated and the potential to be adapted and transferred. Best practices represent the ‘Gold Standard’ of activities and tools that can be implemented to support program objectives.” 27 The accumulating evidence around telemental health clinics for rural American Indian veterans is consistent with this definition.
The quality and process improvement plan for these clinics has been focused on the goal of building a rich set of diverse data, processes, and outcomes to capture successes and challenges. More focused work is needed to understand the impact of PTSD treatment for rural Native veterans that radiates beyond the veteran and into the family and community social structure. An individual veteran's PTSD often has ripple effects that extend out in small, closely knit rural communities, and conversely so does treatment that supports improvement. 28 –33 Family and community consequences of PTSD have been explored in the general population but have not been examined in detail for rural Native veteran populations. The potential wider social consequence of treatment for rural veterans through direct delivery and community-based treatment needs to be better understood and represents an argument for increasing these types of clinic models.
Although these clinics are based on a model of a single psychiatric provider, examinations of different models of mental health treatment delivery should be explored, including mental health team-based approaches and collaborative/consultative treatment in primary care settings. An observation from these services has been the importance of one or two key treatment relationships to facilitate the veteran's interface with the mental healthcare system. As discussed, many of the clinic patients have reasons that temper their interest in engaging in treatment, including historical mistrust of federal systems, 25,26 associated stigma around mental health, 34 –36 past prejudice, system access barriers, 4,35,37,38 and the individually isolative nature of PTSD. 39,40 One of the strengths of one to two primary treatment relationships (e.g., clinician and TOW/TVR) is the ability to build long-term treatment rapport, engagement, and trust. The long-term continuity of the providers (ranging from 4 to 10 years), comprising psychiatrists and nurse practitioners, has been an important component for the cultural specificity of the services and facilitated ongoing patient engagement in the clinics. Alternative models need to take in consideration the importance of this type of trust and rapport building and consider team-based approaches that include a primary individual to foster engagement.
A final area of consideration involves understanding the cost and economics associated with this clinic model. Cost is widely acknowledged as an underdeveloped area in the telemental health literature. 41 –43 In our controlled cost comparison study we demonstrated the potential cost savings of videoconferencing-based assessments with this population. 44 More work is needed in this area, although obtaining these types of data in a controlled manner presents several challenges such as finding an appropriate comparison service and population, as well as attempting examining wider clinic impacts (e.g., community benefits). Additionally, if the realistic alternative to this clinic model is no or extremely limited care (due to geographic and other access issues), then factors such as cost of untreated illness, disease burden, morbidity, and mortality need to be accounted for. It is also unclear how cost factors for clinics in federal systems can be translated into non-federal healthcare systems serving rural populations.
There are several limitations to this synthesis. The foremost is to what extent can the lessons, results, and models described here be translated and generalized to other Native veteran, veteran, and non-veteran populations? We have demonstrated initial success in propagation of this model in the Northern Plains, which presents real limitation in the generalization of each of the individual studies due to limited numbers and geographic and cultural specificity. For this model to gain wider dissemination it will be necessary to better understand which aspects of these clinics afford themselves to wider translation and adaption, which aspects need modification for dissemination, and which are relatively site and community specific and do not lend themselves to generalization.
Indeed the current and future strategic foci of this work will be to better comprehend the issues discussed here. Further expansion of clinical services designed to increase the healthcare access of rural Native veterans will be important to honor their service and sacrifice to our nation. It is hoped that the lessons learned and practices presented can not only assist others working to improve the care for rural Native veterans but also serve as a model for other rural veteran and non-veteran populations.
Footnotes
Acknowledgments
This manuscript was sponsored and funded by the Department of Veterans Affairs, Office of Rural Health, Veterans Rural Health Resource Center—Western Region, Salt Lake City, UT. The views expressed in this article are those of the authors and do not necessarily reflect the position or policy of the Department of Veterans Affairs.
Disclosure Statement
No competing financial interests exist.