
Abstract
The use of telehealth technologies to overcome the geographic distances in the delivery of hospice care has been termed telehospice. Although telehospice research has been conducted over the last 10 years, little is known about the comprehensive findings within the field. The purpose of this systematic article was to focus on available research and answer the question, What is the state of the evidence related to telehospice services? The article was limited to studies that had been published in the English language and indexed between January 1, 2000 and March 23, 2010. Indexed databases included PubMed and PsycINFO and contained specified key words. Only research published in peer review journals and reporting empirical data, rather than opinion or editorials, were included. A two-part scoring framework was modified and applied to assess the methodological rigor and pertinence of each study. Scoring criteria allowed the evaluation of both quantitative and qualitative methodologies. Twenty-six studies were identified with the search strategy. Although limited in number and in strength, studies have evaluated the use of a variety of technologies, attitudes toward use by providers and consumers, clinical outcomes, barriers, readiness, and cost. A small evidence base for telehospice has emerged over the last 10 years. Although the evidence is of medium strength, its pertinence is strong. The evidence base could be strengthened with randomized trials and additional clinical-outcome-focused research in larger randomized samples and in qualitative studies with better-described samples.
Introduction
Hospice care is delivered to more than one million terminally ill patients and families each year in the United States. The National Hospice and Palliative Care Organization estimates that >38% of all deaths in the United States now receive hospice services. 1 Although 49% of hospices in the United States remain as not-for-profit providers, another 47% are now declared for-profit. 1 Despite the tax status, management of a per diem fixed federal reimbursement payment requires all providers to carefully manage costs while delivering care to a geographically disperse, often isolated, and always clinically fragile population.
Hospice care in the United States is primarily delivered in the home setting. This home environment creates many similarities to home healthcare, including large geographic distribution of the patient population. The cost considerations and geographic challenges make telehealth technology an interesting solution for both home health and hospice populations. Although both the technology and research for telehealth technology has grown dramatically over the last decade in home healthcare, there has been less focus on the use of such technology in hospice care. The use of telehealth technologies to overcome the geographic distances in the delivery of hospice care has been termed telehospice. Although telehospice research has been conducted over the last 10 years, little is known about the comprehensive findings within the field. The purpose of this study was to systematically review the literature to discern available research and answer the question, what is the state of the evidence related to telehospice services?
Methods
A systematic review of the published literature was initiated to assess the evidence. PubMed and PsycINFO databases were searched for studies published between January 1, 2000 and March 23, 2010. Key words in the search included “telehospice,” “telemedicine and hospice,” “telehealth and hospice,” “technology and hospice,” and “informatics and hospice.” Studies were included if they were published in English in peer-reviewed journals and reported empirical data. Studies were excluded if they were non-English, in trade or nonpeer reviewed journals, and did not report data but were opinion or editorials. Data were extracted from each article using a standardized form. The extraction process identified the authors, sample size, setting, objectives, study design, and findings. Information collected on the standardized form was entered into a spreadsheet for analysis. The individual study findings were then coded to allow for comparison and identify common themes. Initial coding was developed by one author and reviewed for discussion among all authors. Finally, the articles were each reviewed and scored using the scoring form shown in Table 1 and described next.
Methodological Rigor Scoring
#7 Follow-up modified from original to reflect time frames identified in the study and percentages changed to reflect high attrition found in hospice studies. #9,10,11 scoring of item d changed from 8 to 0 to allow comparison of scores.
Given the limited evidence available in both telehealth and hospice, a decision was made to evaluate the evidence by assessing both the methodological rigor and the significance of each study to the field of telehospice. As suggested by Gysles and Higginson, 2 each study received a methodological score to reflect its scientific rigor as well as a pertinence score to recognize its significance to the overall evidence base found in the field. A study could, therefore, be of poorer methodological rigor yet have findings that are important to the evidence base. This was viewed as an especially critical issue in an emerging domain with limited but increasing evidence.
In recognition of and appreciation for the differences between quantitative and qualitative designs, different scoring schema were used to assess the methodological rigor based on the study design for individual articles. A standardized scoring form was developed to promote reliability in scoring across studies (See Table 1). The methodological rigor for quantitative articles used a modified scoring format from Gysles and Higginson 2 that recognizes differences between observational and experimental research studies. The scoring format is outlined in Table 1, Part 1A. In this model, higher scores represent higher scientific rigor in the data collection, analysis, and reporting process. Scores range from 0 to 22 depending on the presence of certain elements influencing the methodological rigor. For example, a specified randomization procedure is given two points, a nonspecified randomization would be given one point, and a nonrandomized sample would receive no points for that element; thus, lower scores indicate less methodological rigor.
Likewise, the methodological rigor for qualitative articles was assessed using a standardized scoring form modified from the work of Greenwood. 3 There is debate regarding the feasibility of quality assessment in qualitative research, and there is currently no gold standard scoring criteria for qualitative research. Greenwood's model was selected for this project because of its inclusion of relevant elements from several qualitative assessment frameworks and the ease of assessment and scoring generated from this approach. The quality assessment elements are outlined in Table 1, Part 1B. Similar to the quantitative scoring, a higher score reflects a higher degree of methodological rigor in the qualitative data collection, analysis, and reporting process. Articles were scored on a 0–11 scale with higher scores assigned to increased methodological rigor. In general, the more transparent the data collection and analysis, or the better detailed the procedures, the higher the score, as rigor in qualitative methodology is often based on the trustworthiness of the data. 4
The second part of the assessment of the evidence involved evaluation of the pertinence of each of the studies, as illustrated in Table 1, Part 2. This criteria was adopted from a similar scheme for grading studies in palliative care. 5 Pertinence refers to the degree to which the evidence is significant to telehospice. 6 In a Higginson 5 review, the pertinence of the evidence was a sum of three components: (1) the relevance to the building of evidence, (2) the applicability of the study, and the (3) overall value of the study. Relevance refers to having significant and demonstrable bearing on the facts or evidence of telehospice. Applicability is the ease to which the study translates into the implementation in hospice. Finally, value is determined by the significance of the evidence to the base of proof for the field. As in the scoring of methodological rigor, determining the pertinence of a study relies heavily on the clarity and transparency of the information reported in the article. For example, if an author does not report details on how the staff were involved in implementation, the study receives a lower score on this criteria in the same way it would if there were no sampling protocol reported.
Relevance was assessed in the context of the 26 articles reviewed. Articles that contributed something different than the others or a study conducted before others in a category or with a larger more diverse sample were seen as more relevant. Applicability was assessed through the evaluation of the translation of the study to the staff, how the study applied to hospice practice by the staff as well as the demands for staff, training, and resources. For example, if implementing a telehospice project requires substantial staff training, then it is not as translational or applicable as a project that uses current staff without additional training. Finally, a study's value was assessed based on the importance of the study findings for the future of the implementation of telehospice projects or future research in the field. Since pertinence is open to individual interpretation, it was not held as a single quality indicator for any article, rather it was combined with the methodological rigor scores in assessing the overall state of the evidence in telehospice. Although other studies have used this joint approach, no analysis of telehospice has involved this dual assessment.
To minimize bias in the scoring of each article, initial data extraction and scoring was done independently by the two authors not involved on any of the studies in this sample (T.D., H.N.). Coders were familiar with the health arena, but did not have telemedicine experience. Inter-rater reliability was achieved by discussion between the independent graders, and consensus was reached on the final scoring. An analysis table was built outlining the individual scores from each study, and the table was reviewed and discussed by all authors. Bias within studies was assessed in the scoring model through consideration of rigor; bias between studies in the sample was assessed by reviewing the sample of authors, journals, and themes.
Results
The initial search strategy identified 214 published articles. After a review of the abstracts and elimination of duplicates from the combined databases, a list of 50 articles was generated. Finally, the full articles were reviewed, and the inclusion criteria were applied, resulting in a final list of 26 unduplicated, peer-reviewed, empirically based telehospice studies published between January 1, 2000 and March 23, 2010. Figure 1 is a flow diagram of the sampling process.
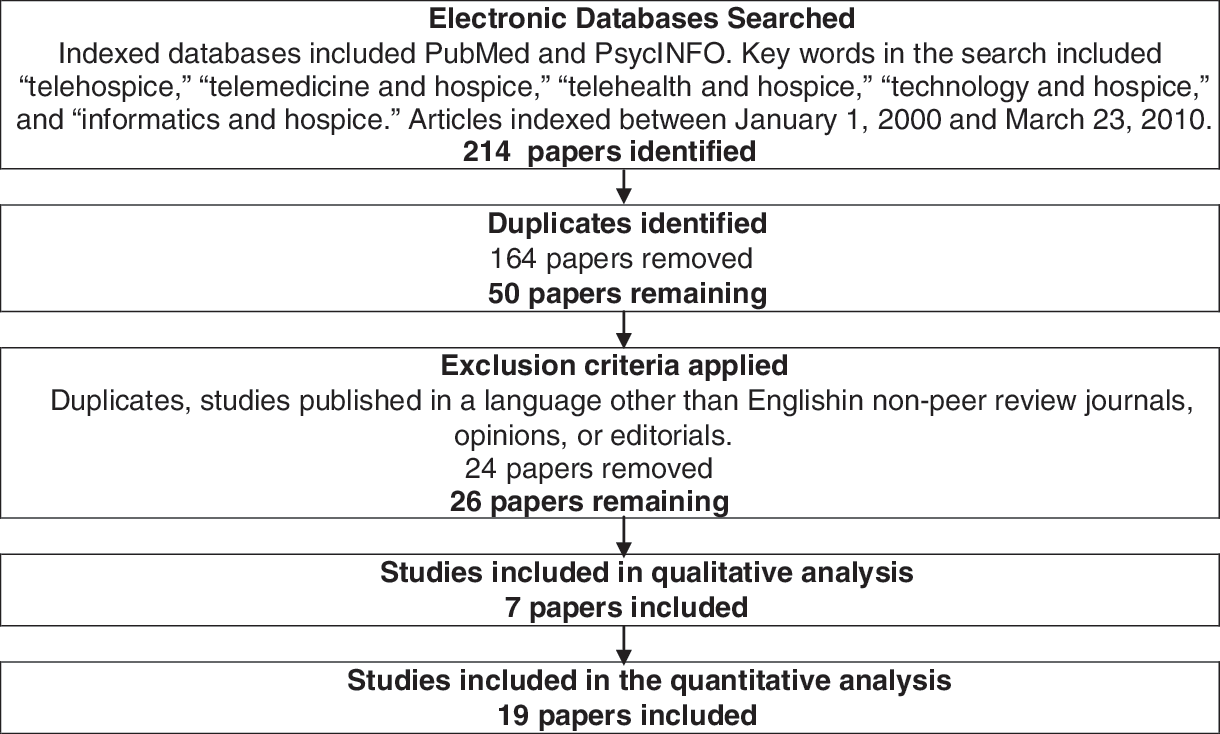
Flow diagram of the search strategy.
The 26 studies were published in 13 unique journals, indicating no journal bias. Of note, the sample involved 10 teams of authors, with 47 different authors publishing evidence related to telehospice. Eight teams published one study, whereas two teams published 18 (61.5%) of the papers, indicating a limited number of researchers in the field and potential researcher bias in the evidence. Funding was acknowledged in 16 of the studies by nine sources and included university funding, private foundation support, and U.S. federal funding from the National Library of Medicine, National Cancer Institute, National Institute of Nursing Research, and U.S. Department of Commerce. The mean sample size in all studies was slightly >407, although there was a large variance with a range of 2 to 3,569. Table 2 identifies and summarizes the articles in the sample.
Summary of Studies in Telehospice
PDA, personal digital assistant.
The findings of the individual studies were categorized into six themes: use, provider attitudes, patient/family attitudes, clinical outcomes, readiness, and cost. The most common findings related to assessments of the use of different telehospice technologies and assessments of provider attitudes. These two categories accounted for 61.5% of all articles. Studies assessing the use of telehospice included the evaluation of telephone advice lines, videophones, personal digital assistants, pen tablets, and computers. The various forms of technology were all found useful in the hospice setting and various considerations for success were identified. Overall, providers were supportive of all forms of the telehospice technologies. The provider attitudes were positive for both perceived usefulness and ease of use in different studies by different groups of researchers. Similarly, patient/family attitudes were assessed in 15% of the studies. Without exception, all articles reported that the majority of patients and families found the technology useful and helpful and demonstrating positive attitudes. In some cases, patients/families reported feeling that their providers could have used the technology more. 7
Clinical outcomes were measured in only three of the studies. 8 –10 The outcomes measured included patient anxiety, caregiver quality of life, communication anxiety, and caregiver perceptions of pain medication. No study was large enough to find significance in these clinical measures, but all found the clinical tools appropriate for use in the setting.
Three studies reported various issues related to barriers to the implementation of telehospice projects. Specifically, despite the positive attitudes toward telehospice technologies, providers were found to be gatekeepers in the referral of consumers for telehospice interventions, thus limiting utilization. These results were discussed among two separate teams of videophone researchers. 11,12 Additionally, organizational considerations were identified that facilitated and impeded the implementation of telehospice projects. 13
The categories of study findings involved the assessment of readiness by providers in two studies and the assessment of cost in one study. Readiness to use and experience with technology varied among providers and points to the need for comprehensive training with implementation of any telehospice project. There was one study that focused on cost of telehospice visits and determined that they were a cost-effective alternative for providers. 14
Methodological rigor was evaluated for each study and is summarized in Table 3. Nearly three quarters (73%) of the studies used quantitative methodologies. Studies were predominately cohort or descriptive. There was one experimental study; however, the differences between the groups were not adjusted, and assignment was not randomized, thus lowering its rigor. The criteria for follow-up (element 7 in the model) were difficult to score, because most studies did not report this information. The mean score for quantitative studies was 9.2 (range of 5–14) representing low-medium strength evidence. The lack of randomization and the lack of a power calculation weakened most of the evidence.
Scoring Summary of Studies in Telehospice
Seven studies used qualitative methodology. The mean score of the qualitative evidence was 9 out of 11 (range of 5–11), representing medium-high strength of evidence. In reviewing the individual components of the quality scoring, the weakest component involved the adequate description of the subjects in three studies. 9,15,16
In assessing the pertinence of the evidence, three component scores created a total score for each study. The total pertinence score averaged 12 (range of 10–14) out of a possible 15 for both quantitative and qualitative articles. This score demonstrates fairly high pertinence of the evidence. Several studies were small, thus reflecting the pilot nature of telehospice research.
Discussion
The assessment of research quality, although controversial, is important for building evidence-based medicine. The goal of a systematic review is to separate unsound or redundant work from innovative and carefully designed studies in an effort to identify gaps and provide guidance to research agendas. 2 A systematic review is, in fact, a systematic collation and analysis of research findings that reduces information into a meaningful integrated package of evidence. 17,18 One of the assumptions of a systematic review is that the evaluation of the evidence reflects what is published, and, thus, the comprehensiveness and accuracy of the evaluation is limited to what is documented in any given article.
The standard orientation of reviews has been toward using the randomized controlled trial (RCT) as the gold standard: however, in many instances, including emerging fields, the assessment of evidence needs to address different types of research, as decisions are made related to policy and implementation on a wider variety of evidence, inclusive of experimental, nonexperimental, and qualitative research. The methodology of these nonrandomized studies lays an important foundation of evidence for understanding meaning and issues that are critical to the future building of more clinically based traditional RCTs. Although there is no universally accepted way to assess qualitative and nonexperimental studies, there are models that have been used to assess the validity of these works. 2
Despite the limitations presented by a small research base in terms of the traditional gold standard RCT, the standardized assessment of evidence can be valuable and used to inform future research agendas. Given the subjective nature of any scoring scheme inclusive of non-RCT studies, we have attempted to do so with the purpose of identifying gaps in the evidence and strengthening the future research in the field. To minimize the limitations, we have used a systematic process for identification of evidence and a defined standardized assessment schema, based on previous reviews in related fields (palliative care), as well as using a two-pronged approach to assess both rigor and pertinence. Finally, as authors of some of the studies in the review, we recognize the potential for bias in the assessment of evidence and, thus, have collaborated with two authors responsible for independent study assessment and consensus.
The identification of twenty six empirical studies shows that an evidence base for telehospice has emerged over the last 10 years. These studies, although of limited number, have established a foundation for the field. The evidence generated indicates that telehospice technologies hold promise to be useful and important tools for the future delivery of hospice care. The studies demonstrate that several technologies may be of use, that stakeholders (staff, patients, and family members) are interested and accepting the use, and that there are potential clinical outcomes and cost benefits. Implementation of telehospice technology has faced barriers in these early efforts including the various levels of readiness among staff, the differing perceptions of use and ease of use, and differing reports of technical quality challenges. Finally, implementation of more than one project has faced gate-keeping challenges by hospice staff, limiting the sample sizes, utilization, and success of the initial projects.
The evidence base, although growing and promising, is of mixed scientific rigor with lower-medium strength evidence in quantitative studies and medium-higher strength evidence in qualitative studies. Due to the limited number of researchers involved in telehospice research, there is also an element of researcher bias in the evidence. In spite of the limited amount of evidence available, the pertinence of all studies is fairly strong. Publication bias is limited, as these studies appeared in several journals across many disciplines including telemedicine, palliative medicine, and computer science. The interest by numerous journals in different disciplines indicates that telehospice is important and has wide-reaching practice, thus further validating the significance of building an evidence base.
If hospices are to invest in telehospice technology, then the evidence needs strengthening. Given the limited resources of hospice programs, patient outcome evidence is critical not only from a clinical perspective but also an administrative one. If telehospice is to live up to the promises found in these initial studies, then increased focus needs to be made in the building of evidence to identify the clinical benefits of telehospice programs and its associated cost savings. Finally, funding is needed to conduct large randomized trials and overcome the methodological limitations that are currently preventing the generalization of research findings. This, however, is not unlike the building of any evidence in palliative care, also a new and emerging field within medicine.
Footnotes
Disclosure Statement
No competing financial interests exist.