
Abstract
The current U.S. economic recession has resulted in a loss of income, housing, and healthcare coverage. Our major goal in this socioeconomic setting was to provide ophthalmic remote health screenings for urban soup kitchen and homeless populations in order to identify and refer undetected vision-threatening disease (VTD). We assessed visual acuity, blood pressure, pulse/oxygen saturation, body mass index, and intraocular pressure for 341 participants at soup kitchens as part of the homeless outreach program in Newark, NJ. History of diabetes, hypertension, and smoking, last ocular examination, and ocular history were noted. Imaging was performed with an 8.2 megapixel non-mydriatic retinal camera with high-speed Internet ready for off-site second opinion image evaluation. Positive VTD findings were identified in 105 participants (31%) (mean age, 53.6 years), of whom 78% were African American, 73% males, and 62% smokers. We detected glaucoma in 34 participants (32%), significant cataract in 22 (21%), diabetic retinopathy in 5 (5%), optic atrophy in 1 (1%), age-related macular degeneration in 1 (1%), and other retinal findings in 43 (41%). The incidence of VTDs was higher among this cohort than among study groups in previous screenings (31% vs. 12%). This finding shows an increase in ocular morbidity in a younger, at-risk population with elevated rates of hypertension, diabetes, and smoking. Functional visual impairment was 2.5 times higher than the national average (16% vs. 6.4%). Comprehensive, community-based screenings can provide more sensitive detection of VTDs in high-risk groups with low access to ophthalmic care and can be an integral part of recession solutions for improving healthcare.
Introduction
The homeless population, as indicated by the number of shelter beds, is increasing. 1 Thirty-one percent of homeless persons are older than 45 years, more than 60% are from ethnic minority groups (primarily African Americans), and 44% are single males. 2 The current economic recession has led to high unemployment rates (9.9% nationally and 14.3% in Newark, NJ as of April 2010), 3 which has resulted in a loss of income, housing, and ultimately healthcare insurance for families and the working poor. This economic trend will undoubtedly significantly increase the number of “poor” (persons living with less than $10,830 [USD] per year; 13.2% [approximately 41 million] of the U.S. population as of 2008) 4,5 and “deeply poor” (persons living with less than $5,415 [USD] per year; 5.7% [approximately 17.6 million] of the U.S. population as of 2008). 6 Those living in poverty report having to forgo healthcare insurance in order to afford food and housing. Physical disease is twice as likely to result in hospitalizations and is more likely to result in death in the homeless population than the general population. 7,8
The Baltimore Eye Survey 9,10 showed that the rates of blindness and visual impairment rose dramatically with age, that African Americans were twice as likely as whites to become blind or visually impaired, that gender did not affect the prevalence of decreased visual function, and that the number of years of education was inversely proportional to prevalence of reduced vision. Factors such as median household income and proportion of households below the poverty level showed a strong correlation with prevalence of low vision. Finally, subjects with poor general health had significantly higher rates of blindness and visual impairment than those with better health. 9,10 In addition, it is well documented that half of the individuals with diabetic retinopathy (DR) and glaucoma are not aware they have these ocular conditions, which if left untreated can lead to blindness. 11 For the above-outlined reasons, our attention was focused on community-based shelters and soup kitchens, with the goal of assisting individuals who would not otherwise see an eye specialist until it was too late to save their eyesight.
Materials and Methods
Personnel and Transportation
The Telemedicine Outreach Program Services was established at the University of Medicine and Dentistry of New Jersey (UMDNJ) in 2005 to screen the homeless, the underprivileged, or the working poor for vision-threatening diseases (VTDs), such as cataracts, glaucoma, DR, age-related macular degeneration (AMD), and other ocular conditions. 12 In 2009, the Student Sight Savers Program, chartered and supported by the Friends of the Congressional Glaucoma Caucus Foundation, joined Telemedicine Outreach Program Services in this screening effort. 13 Our mission statement is to serve, educate, and improve the lives and health of the largely disadvantaged, uninsured communities of Newark, NJ, and the surrounding areas while building meaningful, long-lasting professional relationships with local community leaders in churches and soup kitchens.
Soup kitchens often present challenges by holding the screening activities in basements with steep narrow staircases where all equipment must be hand-carried. The equipment was transported to screening locations by small-panel trucks with heavy-duty lifts to allow for ease of loading and unloading of material. Setup and disassembly took approximately 45 minutes each to accomplish. Soup kitchen screenings were scheduled once a week and required 7 hours in total to perform a 4-hour screening. High participation in the screening program was ensured by having an on-site coordinator and availability of food at the screening sites. The screening team included four to six individuals (two to four students, one imaging specialist, and one on-site coordinator). The students included first- and second-year medical students (i.e., post-baccalaureate) and third- and fourth-year pre-optometry students who intend to apply to optometry school upon college graduation. They were trained to perform screening procedures by the imaging specialist and the on-site coordinator. The imaging specialist is the Director of Telemedicine and Tele-engineering at the Institute of Ophthalmology and Visual Science, UMDNJ. The on-site medical director is a residency-trained optometrist whose duties included (1) evaluating retinal images, (2) triaging the screening participants for either a follow-up evaluation in the ensuing 12 months or for a specialty referral based on imaging and intraocular pressure (IOP), at the University Hospital at UMDNJ or through high-speed Internet for remote second opinion by a posterior pole specialist, (3) discussing screening findings, and (4) answering any follow-up questions that may have arisen. Imaging guidelines of the American Telemedicine Association telehealth practice recommendations were followed for single field/posterior pole screening. 14
Screening Procedure
Speed is vital to the success of the screening process, as it improves overall efficiency, increases the number of persons served, and cuts down on false-positive referrals. The act of seating and positioning participants at the chin rest of the screening instrument is time-consuming and may hinder efficient flow of participants during screening. We have been able to reduce the overall screening encounter time per person by 40% by using a mechanical table (Anthro Corp., Tualatin, OR), which can be electrically adjusted to a height of 6 feet 7 inches (Fig. 1). 15 This allowed participants to stand for the screening, although the table can be electrically adjusted to image individuals who are wheelchair-bound or unsteady. This setup allowed comprehensive screenings of about 12–15 persons per hour.

Screening table with (from right to left) non-mydriatic retinal camera, pan-optic ophthalmoscope, automated air puff tonometer, small-format printer, and laptop computer.
Each step of the screening process was explained to participants before initiation of any procedure. At the onset, first- and second-year medical and pre-optometry students performed the following tasks: history taking; assessment of blood pressure, pulse, and blood oxygen saturation; and measurements of presenting visual acuity and refraction with a handheld automated refractor/keratometer (Right-On Medical, Tokyo, Japan). Presenting visual acuity was defined as the subject's entering vision with distance correction, if applicable. Participants received both verbal counseling and an information pamphlet on smoking cessation, weight loss, and nutrition, on the importance of blood pressure and sugar control and their monitoring, and on general wellness.
Imaging was performed under ambient-light conditions (<125 candelas) to allow for maximum natural pupillary dilation. When these low-light conditions were not possible, a “dilation hood” (Natural Dilation Hood; Pacific Medical Technologies, Vancouver, BC, Canada) (Fig. 2) was used to limit light artifacts and enhance nonpharmacologic dilation. When the hood was not available, the fellow eye was covered to avoid fixation and accommodation, which would result in a smaller pupil. All images were saved on a FUJITSU (Tokyo) laptop computer (LifeBook N Series) with a 17-inch screen for optimal, high-resolution viewing (1440×900 pixels; 32-bit color quality). The use of a small-pupil aperture camera allowed for retinal imaging in eyes with pupils as small as 3.8 mm. For pupils 3.5–3.8 mm, imaging produced a shadow artifact on the retina on single image, which was sufficient for clinical evaluation in most cases. However, for pinpoint pupils (smaller than 3.5 mm), it was necessary to capture two images per eye—the first focusing on the macula and the second on the optic nerve head—as insufficient pupillary dilation often results in a reduction of the field of view from 45° to around 22°. The images were captured within 30 seconds of each other. When combined, the side-by-side, two-photo approach per eye allowed visualization of a full field of view (45°). Using a high flash setting, we imaged the macula first because it absorbs approximately 90% of the incident light; we then imaged the optic nerve head but decreased the flash intensity (by at least 50%) because the optic disc reflects about 90% of the light emitted from the flash tube. The 45° color retinal images were captured with a Canon (Tokyo) CR-DGi non-mydriatic digital camera equipped with an 8.2 megapixel Canon EOS-20D single-lens reflex camera. We selected a single field of 45° that included the optic nerve head, the macula, and the superior and inferior temporal arcades (referred to as Field 1). The images of the right and the left eye were evaluated simultaneously, side-by-side for any asymmetry in the size or color of the optic nerve head (cup-to-disc ratios), arteriolar/venous ratio, nerve fiber layer distribution, macula, and retinal appearance. Clinical guidelines for evaluation of ocular disease from the American Optometric and Ophthalmology Associations were followed. 16 For example, distinction between glaucoma suspect and glaucoma was made based on risk factors such as age, race, family history, IOP, optic nerve head appearance or asymmetry, evidence of nerve fiber layer dropout, etc. In the event of ocular findings consistent with a VTD, multifield photography was performed to capture the ocular findings, consistent with the Joslin DR screening fields. 17 If it was impossible or impractical to image all fields, a clinical referral was recommended to the participant for a dilated examination.
Side view of the dilation hood. The hood limits light artifacts and allows for physiologic pupillary dilation.
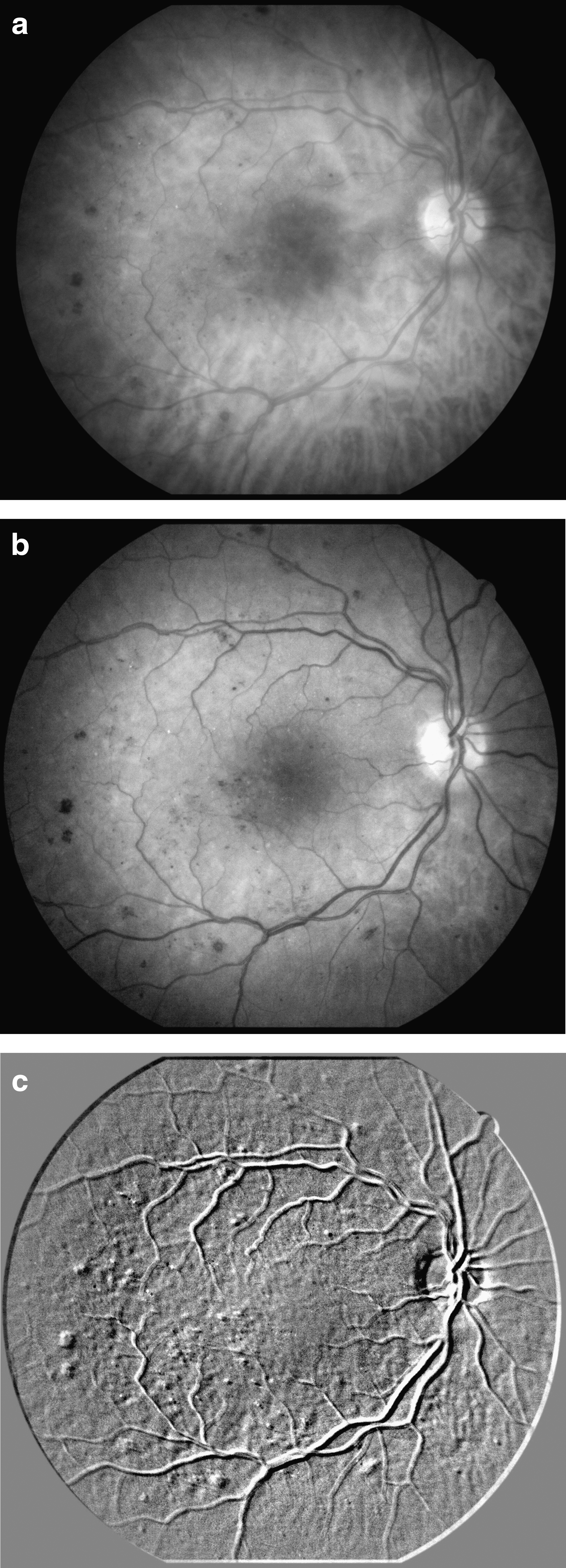
Postcapture imaging processing was performed with Canon's Digital Imaging and Communications in Medicine (DICOM)–compliant Eye-Q imaging software (Canon Medical Systems, Irvine, CA), which allowed for posterior pole layer separation of the images into three monochromatic channels (at one-third of the captured image resolution) (Fig. 3a, b). The three filters included the blue (490 nm) for evaluation of the nerve fiber layer (i.e., glaucomatous changes), the green (550 nm) for evaluation of the retina (e.g., DR, hemorrhage), and the red (610 nm) for detection of the choroid (AMD-related changes, drusen, retinal pigment epithelium disruption, choroidal nevi, and choroidal melanoma). A fourth software-driven filter allowed for a topographical assessment (i.e., elevations vs. depressions) of the posterior pole of the eye, using an “Emboss” function (Fig. 3c). 18 The advantage of using postcapture filters is in avoiding the need to obtain additional images; all the data are extracted from a single image captured for each screened eye. Overall, these postcapture, software-driven filter modalities allowed for enhanced characterization of nerve fiber layer, retinal, and choroidal pathology, which may increase detection and accelerate treatment of VTDs. 19 Collected data and images were reviewed live, on-site, with electronic distant consultation with a medical retina specialist made available via secure Web access.
(
After the imaging session, medical or pre-optometry students assessed the pressure in each eye by using automated noncontact IOP measurements with a Canon (Tokyo) TX-F full auto tonometer. Pressures greater than 21 mm Hg or pressure differences of more than 3 mm Hg were noted during the overall evaluation of our cohort. IOP measurements were performed last in the screening process because the instrument projects a puff of air onto the participants' cornea, which is startling and may reduce participant cooperation during retinal imaging.
Results
In total, 341 participants were screened over a 10-month period at two church-affiliated soup kitchens, health clinics, and homeless outreach services in Essex County, NJ. Participants included 212 males (62%) and 129 females (38%). African Americans represented 79% of our patient population; Hispanics, 11%; Caucasians, 8.7%; and other groups or unspecified, 1.8%. The participants' ages ranged from 10 to 82 years (mean±SD, 47.5±12.9 years). The program was operated at a cost of $12,750 (USD) per year or $750 (USD) per screening, including direct and indirect costs. The average cost to screen a single individual for VTDs was approximately $37.50 (USD). One hundred five participants were identified with some type of VTD. Demographics, detected VTDs, and referral patterns for this cohort are outlined in Tables 1 –3. In addition, 13 participants did not allow adequate imaging owing to opacification of ocular media or small pupil size. These participants were referred for a dilated eye examination.
Screening Participant Demographics
140–159 mm Hg systolic and 90–99 mm Hg diastolic pressure.
>160 mm Hg systolic and >100 mm Hg diastolic pressure.
<20/40 in the eye with better vision.
<20/200 in the eye with better vision.
>21 mm Hg.
HTN, hypertension; CF, finger counting; LP, light perception; IOP, intraocular pressure.
Detected Vision-Threatening Diseases
Pattern of Referrals
More than one referral was made in select situations.
Included suspicion of glaucoma, non-emergent retinal condition, non-surgical cataract, etc.
Discussion
With increasing obesity, poor nutritional habits, and sedentary life style in our society, VTDs, as well as hypertension (HTN), are on the rise. Our program targets all age groups but places emphasis on persons 45 years of age and older. However, reports are showing that children as young as 8 years of age are developing diabetes mellitus (DM) type 2. 20 If the disease is left unmanaged, potentially devastating complications (e.g., earlier need for dialysis, amputation, and vision loss) can arise 12–15 years after disease onset (i.e., before their 25th birthday). Recognizing this trend, we have extended our screening protocol to include elementary school children. We hope that earlier disease detection will lead to prompt initiation of lifestyle modification and/or medical interventions, which may delay disease progression and promote a healthier population.
These yearly ocular health and wellness screenings in community outreach programs are designed for early detection of potentially blinding conditions such as AMD, cataracts, DR, and glaucoma. The prevalence of DR and glaucoma is substantially higher in the African American and Hispanic populations than in the white population. 21 DR is seen in nearly 100% of persons with type 1 DM and in more than 60% of persons with type 2 DM after two decades of disease. 22 Systemic diseases such as DM, when undiagnosed or undermanaged, may result in myriad health-related complications with economic implications.
The overall prevalence of VTDs in our cohort was 31% compared with 12% for previously published screening programs. This result could be in part attributed to higher incidences of important risk factors, such as age, HTN, and DM, for blinding ocular diseases in the VTD cohort compared with other screened participants. Our study participants were 6.1 years older than previously screened communities and had higher rates of HTN and DM: 42% had HTN versus 31% in other programs, and 17% had DM versus 12%. Evidence of glaucoma was found in 10.4% of our screened population, which was four times higher than that for the general African American population. 23 In addition, in our screening population, functional visual impairment was 2.5 times higher than the national average. 24 Although this statistic may represent lack of access to refractive correction in our population, it does not undermine the fact that these individuals are functioning on a visually impaired or legally blind acuity levels. 25 Subsequent studies comparing presenting to best-corrected visual acuity will be undertaken. These results demonstrate an alarming trend of significant increases in visual loss in a group of individuals whose rates of HTN, DM, and smoking are two to four times higher than that of the general population and who lack routine eye care.
The overall psychosocial findings in our study were very similar to those performed on an urban, low-income, multiethnic population in Los Angeles, CA. 26 Both of our populations were predominantly African American and Hispanic, and both had difficulty accessing ocular healthcare services. The authors of the Los Angeles eye study identified three statistically significant factors that predicted receiving an eye examination within the past 2 years: (1) receiving advice from a healthcare provider, (2) possessing eye-care coverage, and (3) having continuity of medical care. Although the majority of our population did not have eye-care coverage, we targeted factors (1) and (3) by providing on-site counseling and directing our participants to visit an eye-care provider once a year (or come back to our screening next year) and to maintain a regular relationship with their healthcare provider. Patients with measurements of ≥160 mm Hg systolic or ≥100 mm Hg diastolic pressure (i.e., stage 2 HTN) were advised to go to the University Hospital Emergency room for evaluation (a walking distance of approximately 20 min). In addition, we educated our population about the effects of HTN, DM, healthy diet, and exercise on general and ocular health.
We believe that community screening outreach programs such as ours can play an integral role in addressing unmet healthcare needs and prevention of catastrophic blindness in the predominantly African American homeless populations, while helping to improve quality of life and to maintain autonomy. The potential cost to society over the lifetime of one individual with diabetes can be as much as $1 million (USD) owing to cost of medications, dialysis, amputations, lost revenue, taxes, and services rendered by social programs such as Medicaid. 27 For working-poor and homeless individuals who do not have access to preventative care, a more feasible health management solution may be found in outreach screening programs. In addition to benefiting the screening participants, these programs offer students an opportunity, early in their training careers, to perform general patient evaluation tasks (e.g., blood pressure monitoring), to become comfortable in establishing patient rapport and counseling, to participate in telehealth technologies, and to learn the pathophysiology of numerous systemic and ocular diseases.
Subject participation is the most challenging part of a community-based screening effort. We have found that providing food at these events is proportionally relevant to a successful and well-attended screening. Having on-site coordination at these soup kitchens allowed not only for participant follow-up but also for bridging the overall healthcare and ocular wellness needs of the community. Our future goal is to expand the program to include provisions for fitting corrective lenses for both near and distant vision.
Footnotes
Acknowledgments
The authors wish to thank Sister Alma Pukel and Mr. Larry Crawford, the on-site coordinators of the St. John's and St. Anne's soup kitchens in Newark, NJ, for their tireless work. This outreach effort was funded by the Research for the Prevention of Blindness, the Grotta Foundation, Inc., and the Friends of the Congressional Glaucoma Caucus Foundation.
Disclosure Statement
No competing financial interests exist.