
Abstract
Store-and-forward telepsychiatry, or asynchronous telepsychiatry (ATP), which allows clinical data, including video to be collected to be reviewed at a later time by a specialist, has been described as a feasible alternative to real-time telepsychiatry, or synchronous telepsychiatry (STP), as a consultation model for primary care. In theory, ATP should be economically more cost-effective than STP due to the increased flexibility of patient data collection and the substitution of the time of specialists with that of lower-cost providers. The aim of this study was to conduct a retrospective cost-analysis comparing ATP with STP and traditional in-person psychiatric consultations in the primary care setting. One hundred and twenty five ATP consultations were performed and fixed and marginal costs were calculated for each model using inputs such as equipment costs, time spent by providers and support staff, and hourly salaries. The fixed costs were $7,000 and $20,000 for ATP and STP and marginal costs were $68.18, $107.50, and $96.36, respectively, for the three groups. STP was the most expensive of the three types of consultations. ATP became the most cost-effective of the three models beyond 249 consultations. The marginal cost savings of ATP were due to substitution of low-cost providers for specialists. ATP represents a potential disruptive healthcare process that could allow more affordable care to be delivered to a larger population of patients. A full accounting of ATP's efficiency will require further studies, including prospective cost-benefit analyses from the perspectives of the patient, provider, and society.
Introduction
Telepsychiatry is the practice of delivering psychiatric care using communications technology. Real-time telepsychiatry, or synchronous telepsychiatry (STP), most often refers to interactive encounters delivered via videoconferencing and is typically used in underserved rural locations where limitations such as physician shortages and long distances make it an attractive tool. STP has been used for years as a consultation model for primary care with clinical outcomes and patient satisfaction measures that are comparable to in-person encounters. 1,2 However, despite data showing that psychiatric consultations are effective in treating patients, 3 adoption of telepsychiatry remains limited.
Store-and-forward telepsychiatry, or asynchronous telepsychiatry (ATP), has recently been described as a feasible alternative to STP in the primary care setting. In ATP, clinical data are recorded and then transmitted via email or other electronic communication to be reviewed at a later time by a specialist. 4 Similar models are in routine use in the fields of radiology, pathology, cardiology, and dermatology. 5 ATP may hold economic advantages over STP because of the increased flexibility of data collection and the utilization of low-cost providers such as medical assistants or nurse practitioners for data collection (videorecording of patients), instead of requiring interviews from more expensive providers (psychiatrists). It has been hypothesized that ATP may be an example of a disruptive healthcare innovation that could bring more affordable care to a larger population of patients than traditional care processes. 6,7
Existing cost-effectiveness analyses paint a mixed picture of the economic benefits of using telemedicine. 8,9 Although many studies show that telemedicine is cost-effective for reasons such as decreased utilization and travel costs, there is a lack of high-quality generalizable data. Reasons for this include heterogeneity of telemedicine programs, inconsistent or inappropriate analytical techniques, small sample sizes, and lack of randomized clinical trials or cost-benefit analyses. 10 Analyses that make up for these deficiencies would clarify arguments for or against accelerating adoption of telemedicine. 11
Early cost-effectiveness studies specific to STP were positive 12,13 ; however, later studies have found STP to be more costly than face-to-face psychiatry. 14 As with other telemedicine modalities, further study will be needed to answer this question definitively, but the potential for increased cost inputs is present with STP due to the need to maintain a high quality real-time video connection, whereas healthcare providers spend comparable time with each patient. ATP, on the other hand, differs from STP in this respect and has not yet been evaluated.
The aim of this study was to conduct a retrospective pilot cost-analysis comparing ATP with STP and traditional in-person psychiatric consultations in the primary care setting using data from a recent ATP feasibility study of ours. 4
Materials and Methods
One hundred and twenty-five (n=125) patients in the ATP study were evaluated at a primary care clinic in Tulare County in California. Patients were identified by primary care providers as having nonurgent psychiatric problems and underwent a standard intake protocol.
The ATP patients' interviews were videotaped at their rural community clinic, and the structured interviews and psychiatric histories including the results of the Mini-International Neuropsychiatric Interview 15 were electronically uploaded to a Web-based, specially-designed consultation program that was compliant with the Health Insurance Portability and Accountability Act.
Participating psychiatrists performed their consultations at University of California Davis (UC Davis) by reviewing all available electronic data including electronic medical records and the videotaped interview and then completing a structured consultation opinion that included their overall best-fit DSM IV diagnoses, Global Assessment of Function (GAF) score, 16 and comprehensive treatment plan. The psychiatrist's consultation opinion was then electronically transmitted to the primary care physician who was given the option of follow-up phone or email consultations with the psychiatrist, and if required or deemed necessary by any of the providers, an in-person psychiatric consultation between the patient and one of the psychiatrists. A workflow diagram illustrating this process is available in a previous publication by Odor et al. 17 STP and in-person consultations are regularly performed at UC Davis in our telemedicine and outpatient psychiatry clinics, and costs for those consultations were readily available to us.
A cost-analysis of the three differing consultation models was performed using recommendations from reviews of telemedicine economic analyses by Whited 8 and Dávalos et al. 10 The analysis was performed from the perspective of the health system. Patient and societal perspectives were not directly addressed in the analysis. All relevant costs were considered. Clinical outcomes were not considered due to the retrospective nature of the data collection.
Infrastructure costs of laptops and video equipment were determined using the cost to UC Davis when known and prevailing market prices otherwise. The proprietary Web-based consultation program for ATP was developed by the study participants, and the cost was therefore known. License costs for the STP software and hardware was estimated using average published prices. 5 Infrastructure that had been previously developed for clinical care or record keeping, given that its use represented an incrementally small portion of its total use, was considered a sunk cost and was not included in the analysis. Examples of sunk costs included use of electronic medical records for consultations and the cost of bandwidth.
Labor costs were calculated by multiplying the time spent by each provider (in hours) by the provider's hourly salary. Hourly salaries were determined by the providers' level of training and corresponding average hourly salary published on the 2010 Bureau of Labor Statistics Web site. 18 Time spent interviewing patients during videotaped interviews was determined by the average length of the digital video files. Other measures of time spent were determined by providers' best estimates based on clinic experiences.
Costs were divided into two groups, fixed and variable. Fixed costs did not vary according to patient volume, whereas variable costs did. From these data, the marginal costs of the ATP, STP, and in-person models were calculated. Finally, a “break-even point,” or the number of patient encounters at which the total costs of the models were equal, was calculated.
Results
The fixed costs of implementing the ATP model were $7,000, of which $4,000 consisted of development costs for the Web-based consultation software, $2,000 consisted of equipment costs, and $1,000 consisted of provider training costs. By comparison, the fixed costs were $20,000 for the STP model due to equipment, software, and training costs. The fixed costs of the in-person model were considered to be sunk costs since the infrastructure was already in place for other clinical activities, and its use during the consultation did not represent a significant proportion of its total use.
Variable costs consisted of labor costs and varied considerably between the models. Each model had similar patient intake processes, which took an average of 20 min. During each ATP consultation, a researcher spent an average of 29 min (±10 min) interviewing the patient, with the longest interview lasting 64 min and the shortest lasting 12 min. The length of the video depended on factors such as the patient's style of speech and complexity of presentation. Uploading the digital video took an additional 15 min. A psychiatrist then spent an average of 30 min analyzing the video remotely while simultaneously creating a consultation opinion.
By contrast, during both the STP and in-person consultations, the psychiatrist spent an average of 1 h interviewing the patient, developing the treatment plan, and communicating the plan to the primary care physician. A telemedicine coordinator also spent an average of 30 min per ATP consultation to meet the technical demands of establishing a reliable real-time videoconferencing connection, and to undertake the consent process.
The marginal costs of the ATP, STP, and in-person models were $68.18, $107.50, and $96.36, respectively (Table 1). STP was the most expensive model in terms of both fixed costs and marginal cost. ATP had intermediate fixed costs and the lowest marginal cost. In-person consultations had the lowest fixed costs and intermediate marginal cost. The break-even point between the ATP and in-person models was 249 patient encounters (Fig. 1).
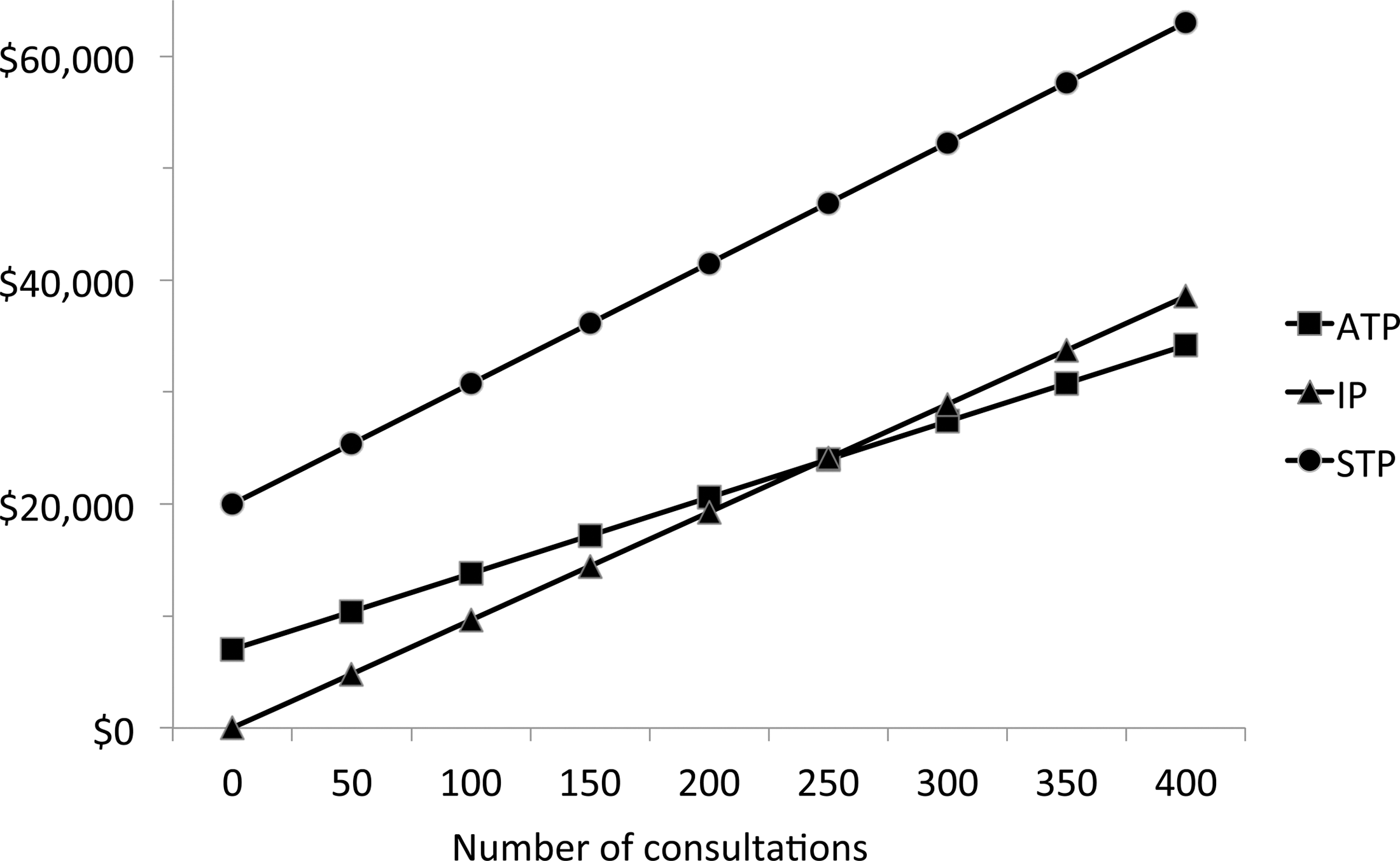
Total cost versus number of consultations. ATP, asynchronous telepsychiatry; IP, in‐person psychiatric consultation; STP, synchronous telepsychiatry.
Summary of Cost and Time Comparisons Versus Consultation Type
ATP, asynchronous telepsychiatry; STP, synchronous telepsychiatry; IP, In-person psychiatric consultation.
Discussion
The results of this study provide early evidence that the ATP consultation model delivers care at lower marginal cost than either STP or traditional in-person consultations from the perspective of the healthcare system. If these data are reproducible, it follows that wider adoption of ATP-like models could lead to less costly delivery of healthcare.
Labor costs are the largest component of healthcare expenditures, so it is perhaps not surprising that cost savings from the ATP model were due to increasing utilization of lower-cost providers (Fig. 2). The typical medical consultation consists of three major elements that do not necessarily have to be delivered simultaneously: data collection, data analysis, and treatment planning. ATP separates these elements in time, allowing lower-cost providers such as licensed clinical social workers or nurse practitioners to collect patient histories through standardized interviews. The more highly trained and highly paid psychiatrist then is able to spend less time per consultation and more narrowly focus on analysis and planning. The psychiatrist spent 30 min per ATP consultation rather than the 1 h during STP or in-person consultation, resulting in cost savings. In addition, psychiatrists noted increased scheduling flexibility since they were able to evaluate patients during any hour of the day including during other patient no-shows and down-time.

Time spent per consultation by providers versus consultation type. ATP, asynchronous telepsychiatry; STP, synchronous telepsychiatry; IP, in‐person psychiatric consultation.
A full accounting of the efficiency of the ATP model would require a cost-benefit analysis, which takes into account clinical outcomes in addition to cost expenditures, and should also be done from the perspectives of patients and society. If clinical outcomes are equivalent or superior while costs are lower, then superiority can be established. The absence of clinical data does not yet allow this conclusion to be made, though numerous studies have demonstrated clinical equivalency between telemedicine encounters and their in-person counterparts. In addition, a review of an analogous substitution of physicians with properly-trained physician extenders in primary care settings showed no difference in quality of care, 19 so it may be reasonable to propose that similar results might occur with the ATP model. Clinical data are currently being collected and will be incorporated into future economic studies.
ATP is not appropriate for all patient encounters. Patients may be uncomfortable being videotaped, for example, or their pathology may be complex enough, or require urgent intervention, to necessitate an in-person interview with a psychiatrist. In these cases patients should be evaluated by other means. However, recorded video offers a wealth of data from which to make clinical judgments, and participating psychiatrists expressed a high degree of confidence in their ability to develop diagnoses and treatment plans. Storing patient videos on electronic medical record systems over time may also provide psychiatrists with additional clinically useful information, especially regarding outcome changes over time or when patients change providers.
The promise of ATP is that by more efficiently allocating providers' time based on their level of skills and training, more patients will be seen at lower cost. This type of disruptive innovation is what many believe is ultimately needed to solve the chronic problem of rising healthcare costs. To determine whether ATP can live up to its promise, further studies, including prospective cost-benefit analyses from the perspective of the patient, provider, and society, are needed.
Footnotes
Acknowledgments
Dr. Alberto Odor, Dr. Don Hilty, Dr. Ana-Maria Iosif, Dr. Paul Leigh, Chris White, George Wu.
This research was funded by a grant from the Blue Shield of California Foundation. The authors report no competing interests.
Disclosure Statement
No competing financial interests exist.