
Abstract
Introduction
Teleophthalmology is the use of ophthalmic information exchanged from one site to another via electronic communications to provide eye care services to individuals who live some distance from the service provider. 1 Teleophthalmology has the promise of improving delivery of eye care to underserved populations and reducing the costs of eye care. 2 –4
Meanwhile, mobile phones have shown to be suitable for medical applications. 5 –8 A smartphone is a mobile phone that offers more advanced computing ability and connectivity than a contemporary basic feature mobile phone. A smartphone allows the user to install and run more advanced applications based on a specific platform. Smartphone use is gaining usage among ophthalmologists, with products like the iPhone® (Apple, Cupertino, CA) and BlackBerry® (Research in Motion, Ltd., Waterloo, ON, Canada) supporting the display of drug references, medical images, decision support, and electronic medical records access.
With the evolution of wireless networks from 2.5G to 3G and further to 4G comes the advantage of very high data speeds, enabling faster and lossless image transmission. In addition to this, the availability of mobile platforms that provide rich imaging features could enable ophthalmologists to view high-quality images, use them in new ways, and thereby provide accurate diagnostics and reports.
The primary goal of this study was to compare a smartphone-based system with a standard office computer workstation towards assessing vision-threatening diabetic retinopathy. The hypothesis established for this study was that using digital fundus photography in convenient locations, in conjunction with smartphone-based teleophthalmology, should make diabetic retinopathy assessment easily available to diabetic individuals.
Materials and Methods
This clinical study was performed in two different settings. The setting for the fundus imaging of diabetic retinopathy was held in the General Internal Medicine (GIM) Clinic, Murrysville, PA. The remote reading of these retinal images took place at 20 miles away at the Eye Clinic, within the complex of the University of Pittsburgh Medical Center (UPMC), Pittsburgh, PA. All instruments and procedures were approved by the Institutional Review Board of the University of Pittsburgh.
At the GIM Clinic, patients were given a tablet PC so they could enter information regarding their personal medical history. If they answered “Yes” to having diabetes, the computer was programmed to offer them the opportunity to participate in this study. Patients reporting the presence of media opacities like cataract and vitreous bleeds in advanced diabetic retinopathy, which could significantly affect non-mydriatic fundus imaging, were excluded from the study. The study coordinators, who also served as the ophthalmic imagers, reviewed the informed consent with the patients and witnessed their signatures. Registration data were then entered into the computer attached to the non-mydriatic retinal camera (8 megapixel CCD camera, model TRC-NW300, Topcon, Tokyo, Japan) by the coordinator. These data included demographic, medical, and ophthalmic information. The patient was then seated at the camera, and three (at maximum) 45° images were acquired for each eye. Fewer images were acquired if the images were thought to be of acceptable quality. At the completion of each patient, the images were uploaded to a server for the picture archiving and communication system (PACS).
After the images were archived in the PACS, they were available for interpretation and grading over the smartphone and also via a secure Web site. The traditional remote examination (gold standard) was transmitted on the backbone of the electronic health record that UPMC had already created and that has been in universal use throughout the UPMC Eye Center since 2006. The viewing workstation was a Dell™ (Round Rock, TX) OptiPlex™ 755.
The quality of image was then compared between the smartphone and Internet-based examination, read remotely and asynchronously by an ophthalmologist (Fig. 1). Basic historical information was supplied to the reader along with the images. This included date of diagnosis of diabetes, hemoglobin A1c level (if known), and date of last eye exam. The images were evaluated systematically. The general quality of the images were ascertained and graded as excellent, adequate, poor but barely gradable, and poor unable to grade. Initially, the optic nerve was evaluated for cupping or swelling. Then the retinal vessels were studied, followed by the macular and extramacular retina. The presence or absence of maculopathy was noted, and all diabetic retinopathy–related lesions were recorded as present or absent. Finally, non-diabetic lesions were listed. The ophthalmologist then created a diagnostic report. The diagnostic information, interpretations, and reports remain in the e-record and PACS for subsequent comparisons and referencing. Two experienced ophthalmologists (R.N. and M.P.) from the UPMC voluntarily participated in this study. The evaluation was mainly divided into three parts, including maculopathy, level of retinopathy, and other findings. Level of retinopathy was noted as follows: None, microaneurysms, intraretinal hemorrhages, hard exudates, cotton wool spots, venous beading, intraretinal microvascular abnormalities, neovascularization elsewhere, neovascularization of the disc, vitreous hemorrhage, tractional retinal detachment, previous laser scars, rhemaogenous retinal detachment, retinal thickening in macula, and soft exudates. Other retinal findings were noted as follows: Macular degeneration, branch retinal vein occlusion, central retinal vein occlusion, and glaucoma. Image quality, recommended follow-up, and other information were also collected for further analysis. The workflow is illustrated in Figure 2.
Screenshot of downloaded study on the office computer workstation.
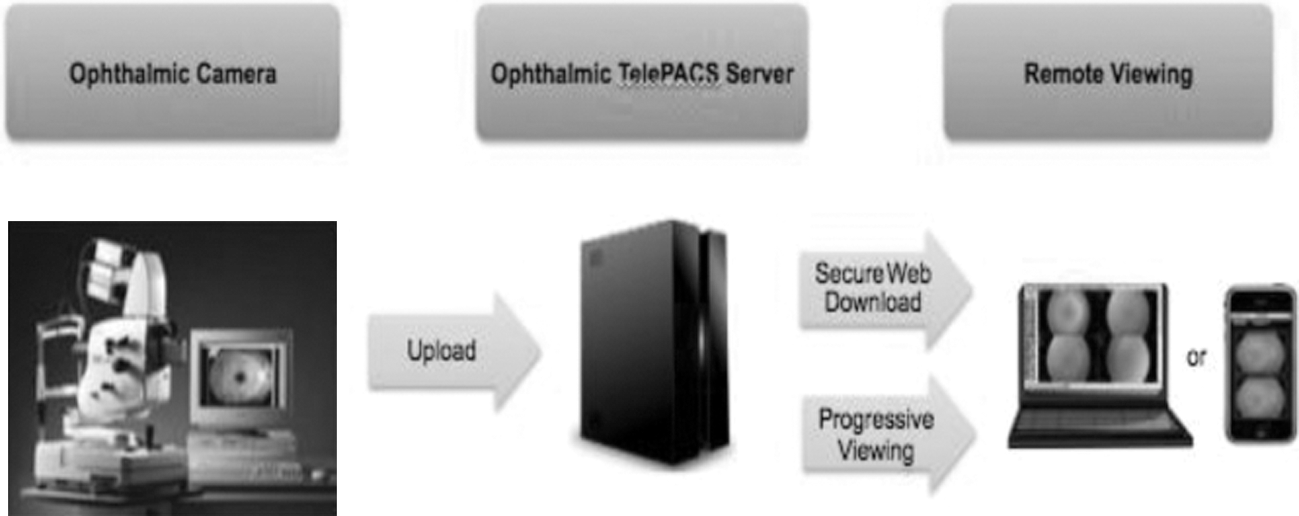
Illustration of the ophthalmic image workflow. PACS, picture archiving and communication system.
The data analysis was performed using SPSS version 17 (SPSS, Chicago, IL). The main outcome measures were the sensitivity, specificity, and κ coefficient between the smartphone and office computer workstation in diagnosing any level of retinopathy. Values of κ of 0.8 and above were considered as excellent agreement between two groups for our study. 9
Smartphone-Based Teleophthalmology
The iPhone 4, a GSM cell phone, was used in this study. The high-resolution display characteristics of this smartphone included a 3.5-inch (diagonal) widescreen multitouch display, 960×640 pixel resolution at 326 ppi, 800:1 contrast ratio, 500 cd/m2 maximum brightness, and a fingerprint-resistant oleophobic coating on the front and back. The operating system is iOS4.0.
For this study, i2iTeleSolutions (

Examples of image viewing modules on the iPhone platform.
Results
This retrospective, comparative study included 55 informed, consenting patients (110 eyes) attending the GIM Clinic in Murrysville. All participants (49% male, 51% female; mean age, 51 years) were previously diagnosed with diabetes mellitus (types 1 and 2). The racial breakdown was 73% white and 27% African American. Type 1 diabetics were 36%. The hemoglobin A1c status was known by only 46% of participants. The last eye examination was greater than 12 months for 46% of subjects. Using the review result from the traditional workstation display as the gold standard, the results indicated excellent sensitivity and specificity (>85%) in all evaluation sections (Table 1). Also, the κ coefficients between the gold standard workstation display and iPhone images to detect retinopathy-related changes for both readers were more than 0.9. The image quality on the smartphone was scored high (91% and 93%) by the ophthalmologists.
Sensitivity, Specificity, and κ Correlation of Office Computer Workstation and iPhone for Detecting Retinopathy Levels by Two Ophthalmologists
CI, confidence interval.
Discussion
Diabetic retinopathy is the most common cause of blindness in Americans under the age of 65 years. 10 It has been estimated that blindness from diabetic retinopathy is preventable in at least 65% of cases, if laser therapy would have been applied in a timely manner. 10 Laser treatments can be quite effective at stabilizing vision and preventing further loss, but in general they are not very successful in restoring lost vision. Therefore, it is critical to evaluate and treat diabetic retinopathy before vision loss is detected.
Commercially available technology has provided new tools to detect eye conditions in an objective and reproducible fashion. Current smartphones are multifunction devices that can be utilized as a near-vision card, Amsler grid, color plates, and pupil gauge in non-office emergency and consultation settings. 11 Smartphone-based diagrams and videos can be used to educate patients about eye conditions or contemplated procedures. With appropriate consent and adherence to privacy rules, clinical photographs, videos, and magnetic resonance imaging and computed tomography images can be wirelessly sent and received securely for real-time consultation with attending faculty and/or subspecialists. 12
The iPhone had a higher specificity in detecting microaneurysms (Table 1). The difference in diagnostic sensitivity and specificity indicated that the office workstation had a lower threshold in diagnosing a patient with diabetic retinopathy compared with the iPhone, especially in cases where there was uncertainty about a suspicious lesion. Although false-positive diagnoses may result in more “unnecessary” referrals to an ophthalmologist, it is critical to note that a screener should always refer the patients with a suspicious lesion to an ophthalmologist to avoid any misdiagnosis of a sight-threatening condition.
This study effectively utilized the advanced image viewing capabilities of the smartphone, including the zoom & pan and pinch & drags capabilities as well as customized reporting template that helps specialists to create medical reports accurately and effectively. The systems used in this study were totally standards compliant, whereby the medical images are always stored in DICOM format. Furthermore, the systems were also Health Insurance Portability and Accountability Act compliant, whereby audit trails are maintained for all activities on the server, enabling traceability of who logged in to the system and who viewed images and when, as well as reporting history. Meanwhile, in this pilot study, the comparisons between the traditional personal computer workstation monitor display and iPhone application were mainly done by two ophthalmologists, and most of the evaluations are subjective and qualitative. Also, the sample size of this study is not large enough to rule out a clinically relevant rate of misses. This study still needs to be further expanded with larger sample size and preferably on with quality comparison using an iPad® (Apple), which has a larger screen and resolution. Although iPads are not as small as current smartphones, they are definitely portable and therefore can be used in m-health applications.
Opportunities and Barriers
Smartphones are widely accessible and have the capability of transmitting data by multimedia messaging service, e-mail, or downloading to a personal computer in a short period of time, where it can be accessed at a later time or place. 11 Further advantages of using a smartphone are that it comes equipped with an increasing number of sensors and peripherals that allow for augmented medical data collection, including voice recorders for note dictation, radio frequency identification or barcode readers, and WiFi/GPRS connections for interfacing with databases. 11 By tying in smartphones to the electronic medical record, eye clinics may improve ophthalmic workflow and maximize electronic medical record use.
However, with attention and growth, a multitude of regulatory and legal issues could emerge in mobile phone–based teleophthalmology, such as licensure and certification, reimbursement, and privacy and security issues. With new interfaces and applications coming to market every day, it is still unclear as how these images could be made compatible to the newer and future smartphones. Groups and individuals engaging in mobile phone–based teleophthalmology practices need to investigate and ensure that the specific practice provides appropriate privacy, confidentiality, and security measures.
Conclusions
The ophthalmic images transmitted through both smartphone and Internet techniques match well with each other. The smartphone is an easy method of accessing an ophthalmologist and a supportive tool for diabetic retinopathy assessments. Further studies are needed to investigate the economic and clinical feasibility of smartphones in ophthalmology.
Footnotes
Acknowledgments
This study was supported by the Eye and Ear Foundation (Pittsburgh, PA) and Research to Prevent Blindness (New York, NY). The authors thank i2iTeleSolutions for their support.
Disclosure Statement
No competing financial interests exist.