
Abstract
Introduction
The development of efficient methods of chronic care management is crucial in light of the growth of the world's elderly population. With a projected monthly increase of 847,000 individuals over the age of 65 years in 2010 worldwide, the increasing burdens of chronic disease on healthcare resources provide a powerful incentive to find better ways to care for chronically ill patients. 1,2 In the United States, these patients account for 78% of all medical costs. 3
Disease management programs (DMPs) offer potential strategies to improve quality and control costs by providing more frequent communication, management, and follow-up. 4 –7 Theoretically, cost reductions are primarily attributable to decreased hospital stays and emergency department (ED) visits.
Remote patient monitoring (RPM) is defined by Coye et al. 8 as “a transformative technology, that is, one that enable[s] a wide range of disruptive and positive changes in clinical care and administrative processes.” In this application, the home care program applies technology to DMPs in managing patients living at home with chronic illness from a distance, through physiological monitoring and telecommunications using telehealth devices. This application of RPM facilitates patient participation in DMPs by reinforcing compliance with daily disease management regimens. Periodic clinician review of data and feedback to patients assist them in mastering basic disease management concepts: For example, patients weighing themselves daily are reinforced when their adherence to a low sodium diet results in weight stabilization. Previous studies have found that RPM improved glycemic control, cholesterol, and blood pressure among Medicare recipients with diabetes. 9 However, a review of RPM patient outcomes across 65 empirical studies found outcomes were more consistent in studies of patients with pulmonary and cardiovascular conditions than diabetes and hypertension. 2 The financial impact of RPM was rarely observed or evaluated, but patient response to RPM was positive, facilitating active participation in their care.
The literature identifies several gaps in follow-up care that contribute to readmissions in patients diagnosed with heart failure (HF), including (1) teaching about diet, self-care, and warning signs such as weight gain, (2) coordinated follow-up care, in which doctors and hospitals communicate about discharge status and needs of patients, and (3) special attention to postsurgical patients, who account for a large proportion of rehospitalizations. 10 RPM can help to close the gaps by providing the patient with self-management tools and facilitating follow-up care.
In a systematic review and meta-analysis of 14 randomized trials, researchers found that remote monitoring of HF patients reduced rates of admission by 21% and all-cause mortality by 20%. 11 Other studies found significant reductions in utilization across multiple disease categories. 12 –14 In 2009, Coye et al. 8 found “a 60% decrease in hospital admissions, 81% decrease in nursing home admissions, and 66% decrease in ED visits among 281 RPM-monitored veterans with HF, in comparison to 1,120 veterans who did not use the technology.”
Conversely, the 2010 study by Chaudry et al. 15 of recently hospitalized HF patients found no reductions in readmissions, length of stay (LOS), or hospitalizations for telehealth patients. The studies reported herein investigate the impact of RPM upon the most frequent diagnosis in hospitalized patients over 65 of age: HF. 16 HF is also responsible for approximately one-third of 90-day patient readmissions. 16 Heart disease is identified as the number one cause of death in the United States by the Centers for Disease Control and Prevention. 17
Hypotheses
Two studies were simultaneously conducted: A randomized and a matched-cohort study. We expected to find that patients receiving RPM would experience lower hospitalization and ED rates, longer times until first hospitalization, shorter total LOS, and lower costs to Medicare. Specifically, for both studies, we hypothesized that 40% of patients in the control group would be hospitalized at least once during the study period and that RPM would reduce that rate to 20%.
Methods
Participants and Setting
All study participants were patients who had recently been released from the hospital who had a primary or secondary diagnosis of HF and were referred for home care posthospitalization. Patients were drawn from two large certified home health agencies operating in the New York metropolitan area. The intervention groups of both studies received RPM as part of home care. New York Heart Association (NYHA) functional classification was assessed at the first visit, which was always a live nursing visit.
Race and ethnicity were abstracted from and defined by the medical record for descriptive purposes. Both studies received institutional review board approval. Written consent was obtained for the randomized study, whiereas the matched-cohort study received a waiver of informed consent. Grant funding for the randomized and matched-cohort studies were provided by the New York State Department of Health and the Fan Fox and Leslie R. Samuels Foundation, respectively.
Description of RPM Technology Intervention and Usual Care
Both RPM and usual care (UC) patients were admitted to a certified home healthcare agency, following a hospitalization. Both groups were managed via DMP guidelines and standards of care for HF based on those of the American Heart Association (2006 guidelines) and the Heart Failure Society of America. As such, home care nurses, trained to teach patients how to manage their condition through medication, diet, and lifestyle modifications, follow a DMP pathway with the goal of preventing and treating congestive HF exacerbation. 18 This pathway guides the nurse's visits, regardless of whether he or she is treating patients using standard home care approaches (live visits) or utilizing RPM.
UC patients received live, face-to-face nursing visits only. RPM and UC group visit frequency was determined by the nurse, based upon the nurse's judgment of patient need, in accordance with home care protocol. Patients in RPM groups received a combination of live nursing visits and RPM visits. A typical visit schedule for patients in the RPM group began with one live nursing visit and two RPM visits for the first 2 weeks, followed by an increased frequency of RPM and a slow tapering of live visits.
The technology utilized closely replicates a face-to-face encounter through two-way videomonitoring. The American TeleCare (Eden Prairie, MN) #1010 video patient station (Fig. 1) was provided, along with instruction on its use. With videoscreens, microphones, and accessories, this technology allows patients and nurses to see each other, speak to each other, and exchange information while in different locations. Nurses contact patients from their desks at the home care agency and are able to watch patients weigh themselves using the scale, listen to patient chest sounds with the built-in stethoscope, and check blood pressure with the cuff to accurately gauge any changes needing attention.
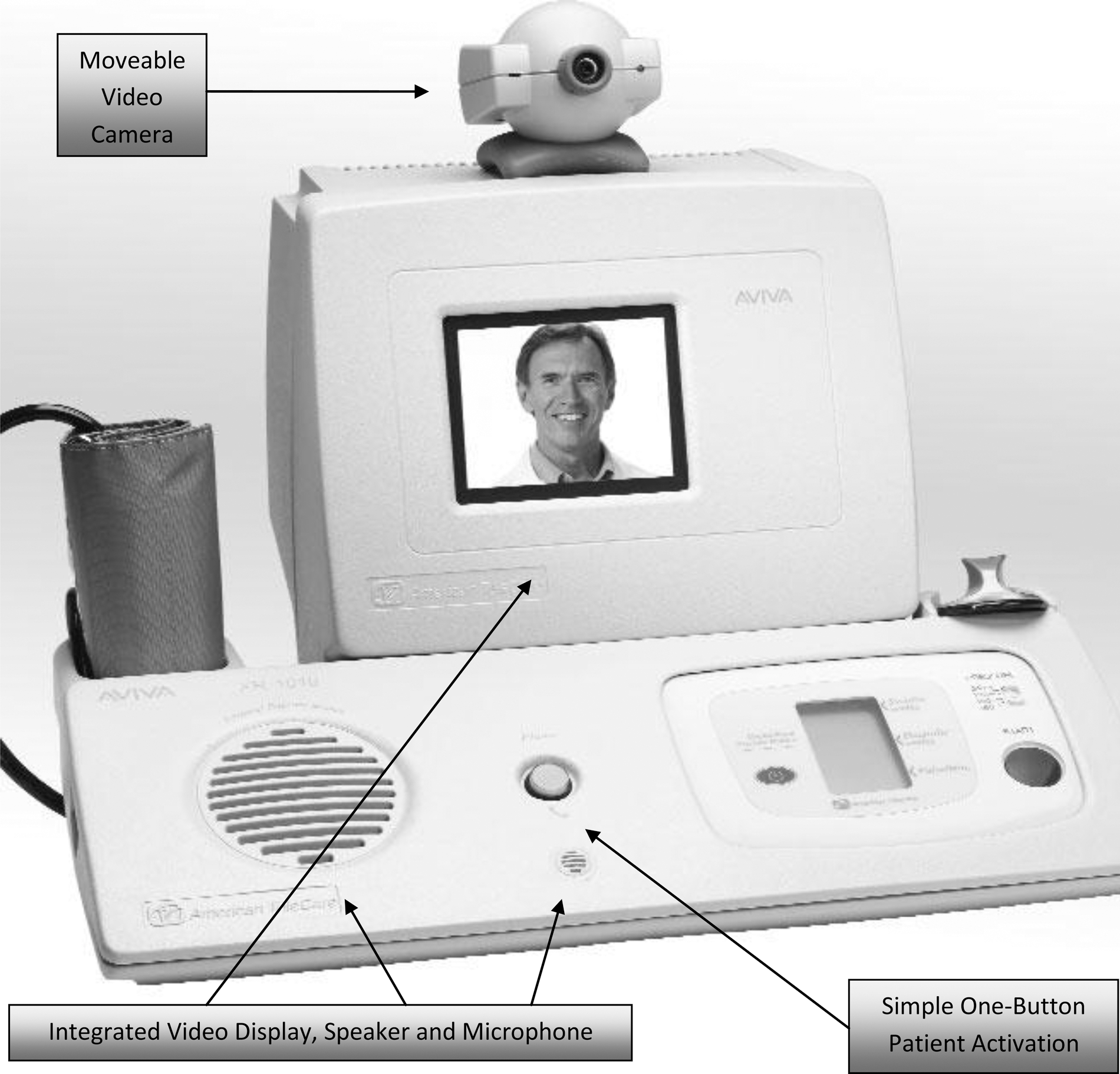
American TeleCare #1010 video patient station. Manufacturer specifications are as follows: Size, 10×16×14 inches; weight: 16 pounds; power, 110 V AC; video display, color LCD. One-button activation links patients with healthcare providers, enabling real-time, two-way personal conversations via an integrated camera, videomonitor, microphone, and speakerphone. Medical peripherals provide a real-time picture of the patient's health status. The moveable color videocamera gives healthcare providers a vivid picture to perform a range of assessments. The unit is equipped with a stethoscope, blood pressure and pulse meter, pulse oximeter, digital scale, and blood pressure cuff. Regarding ease of use, operating is easy to learn and well within the capabilities of most patients. Regarding ease of installation, the unit requires a grounded electrical outlet and an analog phone line. Regarding data transfer, readings from peripherals are securely transmitted to the provider station during video sessions.
The randomized study was quite stringent in the application of RPM (the patient could not begin RPM past the seventh day of home care admission), but in the matched-cohort study the patient could begin RPM at any time during his or her home care stay, as long as the practitioner believed that it would benefit the patient and that the patient was stable enough. Disseminating RPM in a population that did not know they were in a research study enabled the research team to compare results with the randomized study, in which patients were aware of and consented to the research being conducted. Both studies were conducted by the same investigators, at the same time, with patients recruited through the same home care agency.
For both studies, we hypothesized that 40% of patients in the control group would be hospitalized at least once during the study period and that RPM would reduce that rate to 20% (relative reduction of 50%). This hypothesis was based on a review of the telehealth literature. To achieve 80% power for detecting such a difference, 82 patients per arm is required (alpha=0.05, chi-squared test). This also yields 80% power to detect a standardized difference between means of 0.44 (alpha=0.05, two-sample t-test), a "small" to "medium" effect size. 19
Description of the Randomized Study
One hundred sixty-eight Medicare patients with a primary or secondary diagnosis of HF were randomly assigned to RPM or UC from July 31, 2007 to March 31, 2009, upon admission to a certified home health care agency, following a hospitalization. The Department of Biostatistics created a randomization schedule for patient assignment, based on randomly generated numbers. Patients assigned to RPM received their equipment within 7 days of admission to the certified home health care agency and were followed for a 60-day intervention period (the usual Medicare episode of care) and 30 days of follow-up, for a total of 90 days of observation.
Description of the Matched-Cohort Study
One hundred sixty Medicare patients with a primary or secondary diagnosis of HF receiving home care from June 1, 2007 to May 31, 2009 were included in the cohort study. Eighty RPM patients were matched with 80 UC patients. Study inclusion was identical to that of the randomized study, with the exception of the 1-week window of enrollment requirement. RPM patients were matched with UC patients on several variables, including NYHA Class, LOS, principal diagnosis, start of RPM month (to address seasonal exacerbation effects), and patient age.
Measures
For both studies, outcome variables were systematically determined through multiple data sources over the 90-day observation period. All-cause hospitalizations, ED visits, and associated costs were identified through queries of McKesson's Horizon home care database (
Analytical Methods
The primary objective for both studies was to compare hospital and ED utilization and costs for the RPM versus UC groups. Primary outcome variables were proportion of patients hospitalized, time until first hospitalization, total LOS, and cost to Medicare. Similar outcomes are presented for ED admissions. The intention-to-treat (ITT) principle was the primary method of analysis wherein all patients randomized to RPM were compared with all patients randomized to UC, regardless of whether or not they were hospitalized. A second set of analyses compared RPM with UC among only those patients who were hospitalized, in order to identify trends and opportunities for utilization reductions. Two separate analyses were carried out on both the ITT and hospitalized groups: One for the full 90-day follow-up period and a second for a 30-day follow-up period.
The chi-squared test was used to compare hospitalization and ED admission rates. The Lachenbruch method for analysis of data with excess zeros was utilized to analyze time to hospitalization, LOS, and cost to Medicare. 20 The Wilcoxon signed rank test was utilized to test for within-group changes in dyspnea (on a 0–4 scale) and NYHA functional classification (on a 1–4 scale).
Results
RPM and UC patients did not differ on demographic or clinical characteristics. Both study cohorts consisted mainly of white females in their early to mid-80s. The majority of patients had a primary diagnosis of HF, and no differences were found for dyspnea levels, NYHA Class, or weights between the groups (Table 1).
Patient Data
HF, heart failure; NYHA, New York Heart Association; RPM, remote patient monitoring; UC, usual care.
Both studies consistently found no significant differences in primary outcome variables (hospital utilization, LOS, and cost measures) between patients receiving traditional (live) home care and patients receiving RPM at either 30 or 90 days (Table 2). For ITT analyses as well as those of hospitalized patients only, hospitalization rates, time to first admission, LOS, or costs to Medicare did not significantly differ between groups in either study (Tables 2 –4).
Cost, Length of Stay, and Hospitalization Rate at 30 and 90 Days
avg, average; ITT, intention-to-treat; LOS, length of stay.
Total Days to First Hospitalization
Costs and Length of Stay Among Hospitalized Subjects Only
RPM patients were hospitalized between half a day to 4 days earlier across most analyses and observation periods in both studies (Table 3). Although this study was not powered for subanalyses, nonsignificant data trends suggest that the effect of RPM varies by NYHA Class: Reducing hospital costs in HF Classes 1 and 2 but increasing costs in Classes 3 and 4. As can be seen in Table 4, among hospitalized patients followed over 90 days, randomized RPM patients with NYHA classification scores of 1–2 cost Medicare a mean of $12,268, whereas UC patients with NYHA classification scores of 1–2 cost Medicare a mean of $20,794. Conversely, randomized RPM patients with NYHA classification scores of 3–4 cost Medicare a mean of $18,696, whereas UC NYHA Class 3–4 patients cost Medicare a mean of $11,652 over 90 days (Table 4).
Home Care Utilization and Costs
Mean home care utilization in the randomized study was greater in the RPM group (915 live nurse visits and 428 RPM visits for the RPM patients and 904 live nurse visits for the UC patients). RPM visits accounted for 32% of all visits in the RPM group of the randomized study. Mean per-patient home care costs were $153 greater in the RPM group ($816 vs. $663) because of a greater number of overall visits (Table 5).
Home Care Utilization and Cost
Driving time factored into visit time.
R.N. costs per hour factored at $57.36 (8-h day applied).
Software costs=$3.00 per patient-day.
NA, not applicable.
Mean home care utilization in the matched-cohort study was also greater in the RPM group (958 live nurse visits and 539 RPM visits for RPM patients and 1,228 live nurse visits for UC patients). In the matched-cohort study, RPM visits accounted for 36% of all visits in the RPM group. Mean per-patient home care costs were $55 greater in the RPM group ($555 vs. $500), again because of a greater number of overall visits (Table 5). Patients in the matched-cohort study had fewer live nursing visits compared with the randomized study because of later start of care dates for RPM patients.
Discussion
Both studies found no significant differences in utilization and hospital costs between patients receiving RPM and those receiving standard home care, confirming the potential of this technology in home care as a supplement, and perhaps a substitute, for live nursing visits.
The fact that one study utilized randomization and the other used a matched-cohort design does not detract from the interpretation of the data. In the design stage, we anticipated hospitalization rates and costs would be greater in the randomized trial as there was less stability in this population.
As the data accumulated, it was clear that differences in patient stability may have affected utilization outcomes. The authors propose that hospital utilization and costs were lower in the matched-cohort study because patients did not receive RPM until they were deemed “stable.” Randomized subjects began receiving RPM during the first week of their home care stay. In the matched-cohort study, patients were further along in their home care stay at the point of RPM placement and were likely to have had greater comfort with medications, diet, and education related to the disease process and minimal fluctuation in weight, edema, and shortness of breath. Conversely, the 7-day enrollment requirement in the randomized study, with no specific stability of function requirement, may have resulted in a patient sample that was less manageable and therefore prone to earlier and more frequent hospitalizations.
It also became evident from the data that hospitalization rates—one of our primary outcome variables—may be less important than overall costs. The nonsignificant patterns described above with regard to NYHA Class (the RPM group had reduced hospital costs in HF Classes 1–2 but increased costs in Classes 3–4) may be a function of the ability of RPM to detect exacerbation, resulting in an earlier but shorter and less costly hospitalization for patients in the earlier phases of heart disease. This pattern clearly needs further study.
Home Care Utilization and Costs
In the randomized study, RPM was utilized more often as a supplement to UC visits, as the RPM group averaged five RPM and 11 UC visits versus 11 UC visits for the control patient group. The matched-cohort study, on the other hand, utilized RPM more often as a replacement for UC visits—with the RPM group averaging 12 RPM and seven UC visits versus 16 UC visits for the control group. Despite these differences, findings were similar for both studies, indicating that RPM is equivalent to UC as both a supplement and replacement for live visits.
An important issue for further study is the role of RPM in the post–home care population. If, as this study suggests, RPM is equivalent to live patient monitoring, it may well be that RPM is even more effective after home care has been completed, when the standard of care is no nursing visits. Indeed, given that HF patients are likely to benefit from consistent monitoring, continued RPM, particularly for NYHA Class 1 and 2 patients, may be especially cost-effective after discharge from home care.
It is important to note that the type of RPM utilized by these studies does not merely consist of a phone call or a nurse checking data uploaded to a website. These studies utilized live, video-based visits and physiological monitoring featuring high-quality video and audio, a stethoscope, a pulse oximeter, and a weight scale. Given the findings of Sochalski et al. 21 that in-person communication is superior to telephonic communication, our findings may not be generalizable to RPM that does not allow for voice and video.
The recent study of Chaudhry et al. 15 and the findings reported herein were adequately powered and found no differences between the patients receiving RPM and those receiving “standard care.” There are, however, essential differences in both the populations sampled and the intervention itself (in the telehealth technology and the patient experience) that are crucial. First, the study of Chaudhry et al. 15 was conducted in a population in their early 60s; our patients' mean age was in the mid-80s. This may be due to the disqualification by Chaudhry et al. 15 of any patients with a life expectancy of less than 6 months. In our study, more than half of all patients had this designation. Second, the study of Chaudhry et al. 15 did not identify what proportion of patients received home care during the observation period. In contrast, our study focused exclusively on this population. A third, important difference is the technology used by Chaudhry et al. 15 utilized a telephone-based design. In contrast, the model used by the studies reported herein utilized live, video-based visits, which is more likely to be perceived as interactive than an automated phone call.
Study Limitations
Both randomized and matched-cohort studies report large ranges and standard deviations for days to first hospitalization, hospitalization rates, costs, and LOS. This is not unusual as other studies have also reported large ranges in outcomes, verifying the need for large sample sizes to identify significant patterns. 22 Another limitation is that the RPM groups received a larger number of total visits than the UC group. On the other hand, this is one of the major advantages of RPM: More visits are possible by eliminating travel time (and associated costs). Also, this study did not capture dependence on others (e.g., home health aides/family), a possible variable impacting the efficacy of this technology. Lastly, we captured all-cause hospitalizations. Hospitalization rates in both groups may have been lower if the outcome variable was specifically defined as an HF-only hospitalization.
Conclusions
In conclusion, we found that RPM, when utilized in the home care setting in conjunction with a robust HF management protocol, is not significantly different from live visits in managing HF. This technology has the potential to allow efficient monitoring of a large population more cost-effectively than live visits in home care. Specifically, in addition to avoiding costs associated with nurse travel time, this technology allows the nurse to quickly check on patients to determine which ones, if any, require immediate action.
Telehealth monitoring also has the potential to help lower-income, community-dwelling seniors who are not receiving home care and may have transportation challenges commonly associated with low-income seniors. A telehealth visit monitoring vital signs is likely to lower utilization and costs of this traditionally “high end” user population.
Evaluating the impact of RPM should be approached in the same manner as drug efficacy trials. Just as pharmaceutical products have varying effects at different dosages and in different populations, the effect of RPM is very likely to vary by approach (video vs. telephone), frequency of visits, and patient characteristics. We specifically recommend examining the importance of visit frequency and duration, RPM characteristics (video/telephonic), characteristics of the patient (e.g., age, NYHA Class, functional status), care setting (home care, primary care, or simply providing nursing monitoring of the patient living independently in the community), and their effects upon hospital utilization and costs. Consistent with the recommendations of Coye et al., 8 we strongly advocate for the establishment of a national collaborative RPM chronic disease research program to facilitate our understanding of RPM deployment. As RPM is being increasingly utilized in healthcare delivery, it is critically important that we understand what works, by population and care setting, as health systems across the country struggle to manage patients with chronic illness.
Footnotes
Acknowledgments
The authors gratefully acknowledge study support from the New York State Department of Health (randomized study) and the Fan Fox and Leslie R. Samuels Foundation, Inc. (matched-cohort study). These sponsors had no role in the conception, study design, collection of data, analysis of data, interpretation of the data, writing the manuscript, or the decision to submit the manuscript for publication. We would like to recognize the contributions of our research team who did not qualify as authors but who were instrumental in the completion of this project. The team included Joan Lesch, R.N., Pam Donovan, B.A., Julia Tai, M.A., Robert Dufresne, A.S., John Paul Balucan, M.B.A., Tracey Mowatt, M.B.A., Sandra Wenskus, LCSW, Cathy Bell, LCSW, Robin Goodman, LCSW, Marian Korenstein, LCSW, Patricia Reinharz, LCSW, Maureen Ruderman, LCSW, Judith Sheridan, LCSW, Valerie Brunner, LMSW, Sally Swan, LMSW, and Diana Morris, R.N. The authors also would like to thank Theresa Szpilla and Jill Cotroneo for their administrative support for this project.
Disclosure Statement
No competing financial interests exist.