
Abstract
The purpose of this article is to present a taxonomy for telemedicine. The field has markedly grown, with an increasing number of applications, a variety of technologies, and newly introduced terminology. A taxonomy would serve to bring conceptual clarity to this burgeoning set of alternatives to in-person healthcare delivery. The article starts with a brief discussion of the importance of taxonomy as an information management strategy to improve knowledge sharing, facilitate research and policy initiatives, and provide some guidance for the orderly development of telemedicine. We provide a conceptual context for the proliferation of related concepts, such as telehealth, e-health, and m-health, as well as a classification of the content of these concepts. Our main concern is to develop an explicit taxonomy of telemedicine and to demonstrate how it can be used to provide definitive information about the true effects of telemedicine in terms of cost, quality, and access. Taxonomy development and refinement is an iterative process. If this initial attempt at classification proves useful, subject matter experts could enhance the development and proliferation of telemedicine by testing, revising, and verifying this taxonomy.
“Words are born in new sciences like plants in spring. We must resign ourselves to this, and the harm is not so great after all, because the summer that follows will take care of killing of the poor shoots.”
Introduction
The diffusion of a broadly defined telemedicine over the past several decades has been remarkable, though still below proponents' expectations. Today, it is difficult to find a state in the union or a country without an established telemedicine program or plans for developing a telemedicine capability. This trend has involved an expansion of the initial concept of telemedicine to include a wide spectrum of applications and contexts. In turn, the phenomenon has resulted in a parallel increase in concepts, labels, and definitions, some intersecting and others distinct. Unfortunately, this has also introduced a lack of clarity, if not confusion, as to the precise content and boundaries between the original concept of telemedicine and those that were introduced later, including telehealth, e-health, and m-health.
The purpose of this article is to bring clarity and structure and to facilitate conceptual development and research by introducing an explicit taxonomy of the domain of telemedicine. To enable and clarify the discussion in this article, telemedicine is used as a general and inclusive umbrella term to refer to all systems, modalities, and applications for the delivery of personal health services that substitute electronic communications and information exchange for (1) in-person contact between patients and providers, (2) communication among providers, and (3) patient or provider contact with sources of information, decision making, and support systems (e.g., literature, algorithms, electronic Web sites). We first briefly discuss the concept, purpose, and methods of taxonomy and present a classification of extant healthcare domains that rely on information and communication technology (ICT).
The Utility of a Taxonomy
Taxonomies represent attempts to establish explicit classifications according to presumed relationships among similar elements or between the elements and other phenomena of interest. Their main objective is to categorize information for increased theoretical understanding and predictive accuracy in empirical research. Sets of elements are aggregated to enhance their internal homogeneity and the generality and efficiency of empirical predictions. It has been suggested that “entirely satisfactory and reliable work can be done in taxonomy, as in other sciences, without philosophy. But there are times when we need to know what we are doing and why, and then we are faced with the philosophical problem.”*
The precise rules for constructing taxonomies are much less clear. However, informal guidelines for their development include cohesiveness of logical types, mutual exclusivity, intraclass reliability, valid generalization, construct validity, and iterative development. Accordingly, the taxonomy proposed here is an attempt to classify and organize the relevant body of concepts, systems, technologies, and applications pertaining to telemedicine. 2 Like other taxonomies, this requires a multidimensional and hierarchical structure. When properly constructed, each tier in the hierarchy “inherits” or possesses all attributes of the one immediately above it, plus additional characteristics or unique elements that distinguish it sufficiently from its predecessor. The higher the level in the hierarchy the greater generality (or less specificity) is attained, and the reverse is also true. Eventually, subcategories may be used to enhance understanding of the domain under consideration and the relationships among the nodes in the hierarchy. As telemedicine has evolved, so has the complexity of its manifestations. Rather than being a monolithic phenomenon, the forms taken by the application of the technology are as varied as those of in-person care delivery. Rather than treating telemedicine as a single entity with protean applications, a taxonomy allows us to make distinctions that are essential for research and policy.
The situation is not unlike that faced by the emergence and evolution of other knowledge-based fields (e.g., medical informatics, health management, library science). Taxonomy is important to the progress of these fields, because it brings order to an extant body of information and provides an effective guide to the development, collection, and classification of new information. Greater orderliness enhances our ability to conduct summative and formative research leading to a greater understanding of complex subject matter.
Taxonomy development is an iterative process that requires input from its users and repeated refinements. Hence, the process is initiated here with the hope that others in the field will consider it sufficiently useful that they will refine, apply, and maintain the taxonomy of telemedicine.
Background
The evolution of ICT played a major role in the development of all ICT health domains, beginning with basic telecommunication (origins of telemedicine), followed by expanding the scope of telemedicine (telehealth), the networking of ICT (e-health), and most recently, the “personalization” of ICT networks (m-health and u-health). These macrodomains are not well defined, often overlap, and have created a confusion that hinders the conceptual development of telemedicine. One way to resolve the problem is to consider them as an extension of the basic telemedicine concept driven by changes in technology, enabled functionality, and innovative applications. However, to simplify things, we chose to initially treat them as separate domains and subsequently focus on the development of the telemedicine domain, as we explain later.
Telemedicine is a modality of care that challenges the traditional sine qua non dependence on physical presence and contact between providers and patients for medical/healthcare delivery. The urgent need to ascertain the true effects of this modality on the providers, patients, and society at large is both understandable and warranted. To date, the prevailing view among those reluctant to embrace telemedicine derives is, at least in part, from the lack of conclusive evidence regarding its effectiveness and efficiency, although its feasibility, acceptability to patients and providers, and its capacity to improve access are no longer in doubt. The ever-increasing volume of telemedicine literature is rather inconsistent in that while it tends to predominantly support telemedicine, it simultaneously recognizes inherent inconclusiveness, neutral findings, and the paucity of rigorous research.
We must ask, regardless of the application or context, whether definitive evidence can be derived from a single study, no matter how large, well conceived, or rigorously implemented. This problem derives from several factors. Namely, we have to yet (1) reach a clear understanding of the basic parameters and content of the field(s) and its boundaries; (2) define the relationship between the parts and the whole; (3) determine the degree to which success or failure in one component, application, or segment applies to the general context of the application; and (4) identify the discrete units of analysis that should be used in research (e.g., single visits or episodes of care or illness).
In fact, we may never resolve completely the precise nature and tradeoff between the benefits and cost of telemedicine, because the underlying technology is a “moving target.” For instance, when clinical ineffectiveness is attributed to technological imperfections or limitations, further developments or newer forms of technology tend to obviate the problem. Technological limitations are embedded in the specific technologies used rather than any inherent limitation in the broader context of telemedicine. Indeed, there continue to be significant improvements in technology quality (e.g., speed, resolution, connectivity, storage capacity) that are often accompanied by reduced prices.
It is not clear what constitutes telemedicine vis-a-vis telehealth; whether the two terms can be used interchangeably; and what, if any, are the real differences between them? The introduction of more terms (e-health and m-health) complicates the situation further. Moreover, within the context of telemedicine, it is not clear what constitutes the parts or the whole. More specifically, to what extent should evaluation of any clinical application be contingent upon: (1) communication modality (e.g., synchronous, asynchronous, mobile); (2) technological configuration (e.g., equipment, bandwidth, connectivity); and/or (3) composition and relationship of the participants (e.g., patient and provider, provider and provider, user and information sources)? The fundamental questions addressed here are how we can best organize and classify the knowledge base in telemedicine and how to differentiate it from related fields.
We have to yet reach full consensus as to whether the intended clients of telemedicine are limited to residents of rural areas and other isolated and underserved populations (e.g., those in long-term care facilities and correctional institutions) or whether telemedicine is equally relevant among the general population as a routine component in everyday clinical practice, clinical decision support, and care management. Recent federal efforts to promote the use of electronic health records and “Meaningful Use” regulations present new opportunities toward a national goal of adopting these technologies for more efficient and effective healthcare in all areas of the country. It seems clear that we may never be able to deploy a sufficiently large-scale, multi-institutional clinical trial with sufficient rigor (sample size and controls) to represent all configurations of applications, functions, and technology (as will be described later) to reach definitive conclusions on all the relevant questions regarding the benefits and costs of telemedicine. Despite its potential merit, and considerations of experimental design and sampling aside, the feasibility and cost of such an enterprise would be prohibitive.
The Need for Taxonomy
Telemedicine is a multidimensional concept, and it can mean different things to different people depending on the context in which it is used as well as the combinations of clinical and health applications, technological configurations, human/technological interfaces, organizational structures, and human resource mixes. Telemedicine comprises all these combinations. When viewed in their totality, the multidimensional combinations form a mosaic, wherein each permutation may have widely divergent effects on cost and quality of care as well as access to care. This is problematic in the context of research, policy development, reimbursement, and care provision. Hence, a taxonomy is essential for the conduct of research, policy making, reimbursement decisions, as well as provider acceptance.
Research
Obviously, a clear and precise taxonomy is needed to identify the precise nature of an intended intervention and to guide researchers in measuring its effects. This would allow us to define the discrete or nonoverlapping independent variables that represent the true and full nature of the intervention, to identify and control the intervening or contextual variables, to itemize the expected outcomes, and to determine how best to assess them. An explicit taxonomy can help us understand and thus clarify the units of analysis in telemedicine research. Further, a telemedicine taxonomy can clarify those applications for which the effects of telemedicine should be analyzed on the basis of single visits, encounters, and/or episodes. If the latter, the type of episode must be considered (i.e., care or illness episodes). Research designs need to account for short- and long-term, direct and indirect, as well as intended and (to the extent possible) unintended effects. Hence, research and analytic designs, measurement tools, and interpretation of findings require appropriate and accurately selected variables, precision, accuracy, completeness, and validity that a taxonomy can enable.
Policy
When policy determination is guided by empirical evidence, policy development requires definitive information about the relationships between specific interventions and expected outcomes, in terms of return on investment, cost/effectiveness, and cost/benefit ratios. Perhaps more importantly, conclusive data are needed on improvements in health and wellbeing, and equity and fairness, for the public. Finally, the relative merit of various organizational, financing, and care delivery models within the constraints of the prevailing health system (in whichever state or country) must be clarified. These relationships require explication, which, again, can be derived from a taxonomy.
Reimbursement
Public and private sector payers, to the extent possible, require unambiguous information on the effects of various telemedicine modalities, primarily the use of service and its complexities (e.g., emergency room visits, hospitalization, hospital length of stay, intensity of care, amount and types of tests and procedures, and prescribed regimen). The use of these services accounts for the payers' liability for covered benefits. Payers need precise information on the nature of the benefits and costs that affect their financial exposure and risk insofar as their subscribers or beneficiaries are concerned. A taxonomy could be very important for all three factors that are used by Medicare in its Resource-Based Relative Value System of setting provider fees. These include the cognitive component (the complexity of a procedure—removing a melanoma is more demanding than removal of a skin tag), which accounts for about 50% of the fee; the practice overhead (the cost of a telemedicine system in the context of a provider's practice), which accounts for ∼45% of the fee; and the cost of malpractice insurance. Medicare also adjusts fees for geographic variation, and this is also relevant to telemedicine.
Providers
Providers are crucial gatekeepers to the ultimate diffusion of telemedicine. Their requirements of the technology include valid and reliable information on the effects of telemedicine on the medical care process and outreach, impact on work flow, the quality of care delivered, productivity, and return on investment. Convenience is also important. Hence, despite this group's varied and sometimes overlapping perspectives, as gate keepers, all would benefit from a clear understanding of the nature, content, and effects of telemedicine as a modality of care in comparison to that delivered in the traditional in-person setting. The proper nomenclature would help in focusing on system requirements and applications, where to look for information, and how to coordinate resources for maximal efficiency.
ICT Health Domains
The concepts and terms that have proliferated concerning the use of ICT in healthcare, including the full range of electronic processing, storage, and exchange of information, can be grouped into two sets corresponding to two levels of generality.
The first level consists of concepts that refer to a field as a whole, labeled here as a domain of care. This is similar to the concept of class in biology and social science. In historical order of introduction and development, the domains (or classes)—shown in Figre 1—include telemedicine (1905 and 1969), telehealth (1978), e-health (1999), and m-health (2003). Each of these concepts shares a common attribute with the others, namely the substitution of ICT for physical co-presence during the exchange of information between the participants. Further, all are designed for the exchange, provision, and/or receipt of medical care and health-related information. However, despite the shared attributes, the referents of these domains are distinct, and therefore, the terms are not interchangeable. In fact, when used properly, they include different orders of activities, behaviors, and/or content.
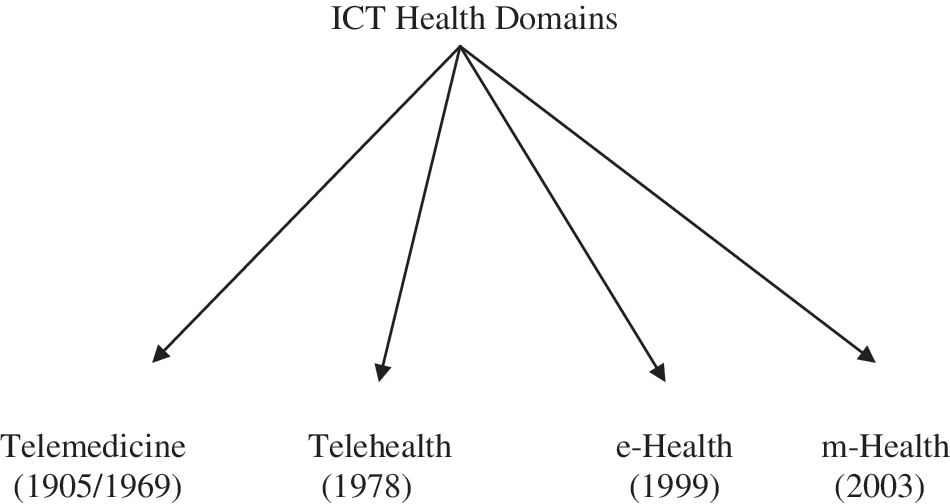
Current information and communication technology (ICT) health domains and their origin.
Each of these domains, in turn, consists of several components or “orders.” Rather than being recognized as distinct, because of the current uncertainty and fluidity in the use of terminology of both domains (classes) and components (orders), there is confusion and lack of precision as to their meaning and content. In this article, we attempt to resolve these issues conceptually and heuristically. We start with a classification of ICT health-related applications into the four domains: telemedicine, telehealth, e-health, and m-health. This is the first step leading to the development of a specific taxonomy for the telemedicine domain. Typically, each domain contains several unique components (or facets), and each component contains several dimensions and subdimensions. The proposed taxonomy of telemedicine, presented later and analogous to Linnaean taxonomy, is based on dimensions, components, and subcomponents, where applicable.
As illustrated in Figure 1, the four current ICT health domains originated at different time periods and in different contexts (described in the subsequent section). Despite the frequent “interchangeable” and overlapping use of these terms, they have distinct meanings and reflect different trends in society, in general, and healthcare, in particular. The following discussion pertains to these trends. For purposes of parsimony, we group the domains by date, focusing first on the earlier telemedicine and telehealth, followed by e-health and m-health.
Telemedicine and Telehealth
Einthoven, a Dutch physician and inventor, first used the prefix “tele” in a medical context in 1905. He referred to a successful telephonic transmission of electrocardiographic images as the “telecardiogram.” 3 In 1950, inventor Cooley and radiologist Gershon-Cohen coined the term “telognosis”—“an abbreviation of three terms teleo, roentgen, and diagnosis”—for the transmission of radiographs over wire or radio circuits. 4 Jutras followed in 1957, introducing the term “telefluoroscopy.” 5 The latter two terms did not achieve much traction and were soon forgotten.
The first documented use of the terms “telediagnosis” 6 and “telemedicine” 7 was made by Bird and his colleagues in 1967 and 1969, respectively. Bird defined telemedicine essentially as the delivery of medical care “without the usual patient–physician confrontation.” 8 Bennet and his associates coined the term “telehealth” in 1978 to extend the scope of telemedicine by incorporating a “broader set of activities, including patient and provider education” in addition to patient care. 9 This latter group of researchers introduced telehealth while working on a project involving an assessment of telemedicine for the Department of Health, Education and Welfare, now Department of Health and Human Services.
In contrast to telemedicine, telehealth was intended to denote a more inclusive conceptualization of an ICT health domain. Conceptually, telemedicine to telehealth is what medicine is to health. The closest corollary practice domains are medical care and public health, but others may offer a different explanation of the relationship between the two concepts. In any case, the term telehealth reflects, in part, a form of political correctness in modern discourse also evident in the adoption of a more inclusive nomenclature in medical care generally. This is manifest in relabeling hospitals as medical or health centers, physicians as providers, and patients as clients or consumers. In part, it also reflects an expanded perspective on the maintenance of health and progression of disease because of increased awareness of behavioral and environmental factors as well as the inclusion of other vital health professions such as nursing, pharmacy, and rehabilitation in the care process.
To some degree, the historical separation between public health and medicine may have been arbitrary from the start. It occurred at the turn of the 20th century when the medical profession was eager to establish its credibility and professional control over the practice of medicine and the delivery of personal health services. Anyone without a license was legally barred from medical practice. 10 Public health practice as we know it today was practically nonexistent. But, within a decade or so from the scientific reforms in medical education, public health was introduced into university programs. The first school of public health was established in 1916 (Johns Hopkins School of Hygiene and Public Health; since 2001, John Hopkins Bloomberg School of Public Health). In the early days, public health focused on hygiene, the spread and control of infectious diseases, and health aid for the indigent. The purview of public health began expanding in the late 1950s and has continued unabated, as will be explained later.
The overlap in content between medicine and public health resulted from several significant factors, namely (1) the wide recognition that the health of populations and individuals cannot be solely attributed to medical intervention (as already indicated); (2) the success of public health in identifying major health risk factors in individual lifestyle and environmental quality and the development of successful interventions aimed at health promotion/disease prevention and environmental quality improvement; and finally, (3) the development and increased relevance of health services research in explaining the effects of structural, organizational, financial, and administrative arrangements in healthcare as well as providing effective tools for health policy analysis and health management.
Today, it has become customary for patients to be queried about smoking, excessive drinking, and other risk factors when completing their previsit forms at clinics and medical centers. They may also be provided with educational materials and/or referral to treatment programs such as smoking cessation and weight control programs, when indicated. There is little or no concern as to whether medicine is encroaching into the purview of public health. Similarly, several areas of public health focus on the etiology of diseases and the effectiveness of various modalities in financing and organizing personal health services, health insurance, care management, as well as quality assessment and quality assurance in medical care delivery.
E-health and m-Health
E-health and m-health are neologisms introduced to reflect technological innovations and their wider use in healthcare. Both terms have been mostly advanced by business and industry to emphasize the utility of emerging technologies in healthcare. 11,12 Thus, e-health and m-health are highly technetronic. Nonetheless, both terms have been adopted in the literature, in some professional circles, and by highly reputable organizations, such as the World Health Organization. 14
We now turn our attention to a brief discussion of the components of the three domains (classes) of telehealth, e-health, and m-health, respectively, followed by a detailed explanation of the taxonomy of telemedicine. It may be appreciated that the inclusion of these three domains in this discussion is problematic. Indeed, they and their components are not orthogonal or existentially/statistically independent.
The Telehealth Domain
Some may argue that an all-inclusive definition of telehealth would incorporate telemedicine as one of its constituent parts. On the other hand, it may also be argued that telehealth is a component of telemedicine, simply more broadly defined. Neither position is taken here, because such a stance would substantially add to the complexity of the taxonomy of telemedicine without contributing to its clarity. Moreover, there is no compelling case for adopting this view, and no one has yet advocated that medicine is part of public health or the reverse. On the contrary, the greater the inclusiveness or generality of any of these concepts the more likely it is for us to interpret them in amorphous and imprecise ways. This situation is similar to a generic problem in coding systems and orientation of coders, where there are basically two types “splitters” and “lumpers.” Lumpers see the similarities between things more readily than they see the differences, and thus, they “lump” objects into relatively few classes to gain generality. Splitters tend to see the differences more readily than the similarities, so they tend to “split” the objects into a larger number of more narrowly defined classes to gain precision. Further, splitters emphasize the necessity for detail and seek to identify differences between things and phenomena as a means to establish cause and effect relationships between them, whereas lumpers are mostly concerned with common attributes and similarities as a means for a broader classification.
Our primary concern here is the clarity of these concepts as a means to reach a better understanding of the content and boundaries of each domain and establishing a credible set of discrete variables that represent its essential attributes. Hence, we treat telehealth and telemedicine as two separate domains analogous to the domains of medicine and public health. Conceptually, this distinction is clear and substantive. Accordingly, the various components that comprise telehealth are essentially those that comprise public health. They include disease epidemiology (the basic science of public health with a focus on the etiology and distribution of health and disease in the population); health behavior and health education (concerned with the effects of individual lifestyle on health and disease); health services management and policy (concerned with the organization, management, financing, and delivery of personal health services); environmental and industrial health (concerned with the health effects of chemical and biological agents in the environment); and biostatistics (which uses statistical tools for the measurement, analysis, and prediction of health and disease at the population level). However, not all of these components are equally amenable to the use of ICT. Indeed, the use of ICT and the prefix “tele” is more applicable in some of these components than in others. Thus, it is not clear whether telehealth can be related to all fields of public health appropriately. For instance, it is clear how disease surveillance in the population and environmental monitoring can be effectively accomplished via electronic devices in contrast to biostatistics. That is why we excluded it from this classification. The proposed components of the telehealth domain are shown in Figure 2.
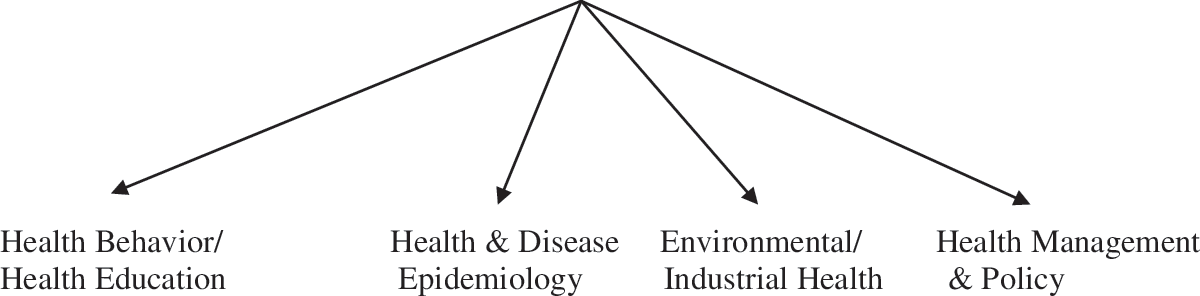
The proposed components of the telehealth domain.
The e-Health Domain
The term “e-health,” as well as other e-words such as e-government, e-commerce, e-education, e-business, e-entertainment, and e-solutions, was introduced primarily by business and commercial interests in the late 1990s. This proliferation was enabled by the increased functionality of the Internet and electronic data systems. Indeed, the “e-movement” was prompted by the phenomenal success of the Internet, evidenced by the rapid progress to dominance of e-mail as a medium for communication in all sectors of society, including health. E-commerce was heralded as a new and efficient means to conduct business and financial transactions of various types. The intent of the “e-solution” was to convey the promise, excitement, and hyperbole in relation to this new technology. This was not lost on the World Health Organization, which adopted an all-embracing normative definition of e-health as “the cost-effective and secure use of ICT in support of health and health-related fields, including health-care services, health surveillance, health literature, and health education, knowledge, and research.” 15 Nonetheless, to date, no consensus has emerged as to a uniform, let-alone unique or nonoverlapping, definition of e-health that differentiates it from similar domains. Some in the field use the term to refer to health applications that rely on electronic processing and the Internet, whereas others prefer to use it as an even more inclusive reference to any computer usage in healthcare (see Oh et al. 16 )
Lacking agreement on a clear definition of e-health, it is difficult to identify its content with any assurance or precision. We chose to include under its purview applications that are generally agreed upon, particularly those that do not overlap with those of the other domains. Nonetheless, they are an ICT/Internet-driven set of applications, as illustrated in Figure 3.
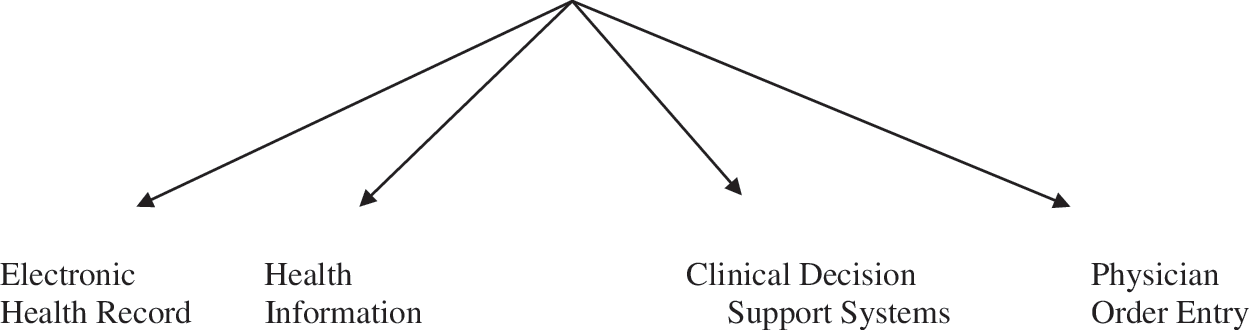
The proposed components of the e-health domain.
The m-Health Domain
The term m-health was introduced into the literature in 2003 17 in response to the vast expansion of mobile communication technology and its perceived usefulness in facilitating access to healthcare, especially in the developing world. Its rationale rests on the global ubiquity and expanded capabilities of mobile communications, which are matched by burgeoning unmet health needs also on a global scale. As with telehealth and e-health, some have suggested that m-health incorporates the preceding domains of telemedicine, telehealth, and e-health as long as their applications depend on mobile communications and network technologies.
The advocates of m-health emphasize the phenomenal reach of mobile technology as the means for improving access to care for underserved populations and communities throughout the world. 13 An important feature of m-health is its person-centered nature and ubiquity enabled by mobile phone technology and connection to the Internet (as a Personal Area Network). The utilization of m-health tools for health education (for both providers and patients) is perhaps one of the best and most widely used applications for this medium. However, m-health is the only ICT-based health domain justified solely on the basis of mobility of a communication modality, albeit an increasingly complex and sophisticated technology that involves the transmission, storage and receipt of voice, still images, data, and video. Hence, it is not yet clear whether this domain will endure and, ultimately, how it can be conceptually and empirically differentiated from telemedicine, telehealth, and e-health as each of these domains do incorporate mobile communication. Moreover, it can be argued whether there is any merit to keep adding neologisms in healthcare simply on the basis of emerging new technologies or conveyances. Nevertheless, the proposed components of the m-health domain are illustrated in Figure 4.
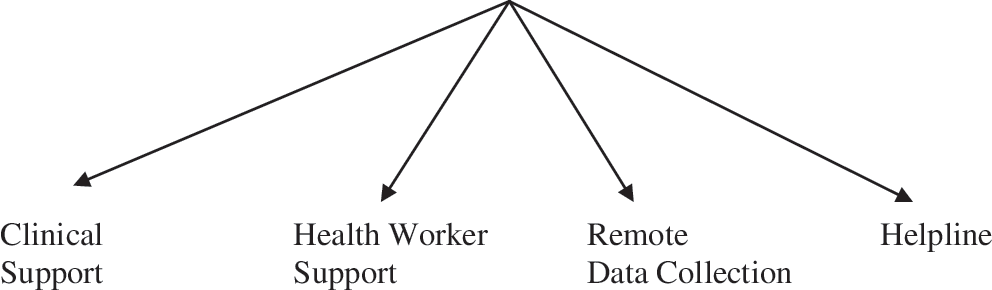
The proposed components of the m-health domain.
The Taxonomy of Telemedicine
Our main concern here is to explore the taxonomy of telemedicine, and the remainder of this article is dedicated to this effort. Hence, an exhaustive exposition of telehealth, e-health, and m-health are beyond our scope. Explaining the specific content and the demarcation lines between these domains and their constituent parts beyond what is presented earlier—where they intersect and where they do not—are neither simple nor straightforward and not germane to our major purpose. In addition, the recency of these terms, especially, e-health and m-health, renders the task of developing appropriate taxonomies problematic. Moreover, including all these concepts under the rubric of telemedicine, however appropriate it may be, would almost certainly detract from our intent. Those interested in developing for the other domains' taxonomies may wish to use the proposed telemedicine taxonomy presented below as a template for explication as well as consider the revisions necessary to complete that task.
As explained earlier, the process of identifying discrete sets of variables representing specific telemedicine configurations is crucial for future research, policy making, and the actual conduct of telemedicine. As such, this process defines telemedicine by identifying composite sets of variables that represent to the extent possible the true nature of the intervention and also incorporate the major dimension of telemedicine and, in turn, their constituent parts.
To date, the majority of telemedicine research has been limited to (1) testing application feasibility without the inclusion of explicitly non-ICT counterparts, or (2) comparative analysis of in-person versus remote clinical visits, encounters, or diagnostic activity. The only notable exceptions are instances in which certain technological aspects were linked with—or integral to the conduct of—the clinical application. In dermatology, for example, important distinctions have been made between online (synchronous) consultations and those conducted in store and forward (asynchronous fashion). 18,19 The same is true in other specialties. In pathology, robotic dynamic arrangements have been compared to traditional static frozen section slides; and in radiology, ultrasound was used either in real time or sent as still images for later asynchronous interpretation. 20 Without such distinctions, all telemedicine encounters might be treated as homogeneous interventions or modalities despite significant variations between them, particularly in terms of differences in cost and quality. In other words, we cannot assume that all in-person and all remote activities are similar, irrespective of the specific technology or functionality involved.
The distinction between technological modalities in clinical applications is a major step in the right direction. Nevertheless, it is not sufficient, and other dimensions must be incorporated. Indeed, the rapid pace of technological development, the proliferation of clinical applications and functions, and the diversity of the type of setting in which these services are offered make it necessary to develop a comprehensive multidimensional classification to represent telemedicine. We need to understand the effects of specific composites or bundles that constitute the various categories. The bundles must identify unique sets and subsets of applications, functions, and technologies, thereby requiring a multilayered hierarchical system. Moreover, we need to understand whether or not telemedicine remains essentially limited to connectivity over distance, as originally conceived several decades ago. Also, how is connectivity to be defined and measured by current standards? Does it apply equally to all clinical applications? Is there a link between bandwidth and quality of service, and does this translate to a difference in quality and/or cost of care?
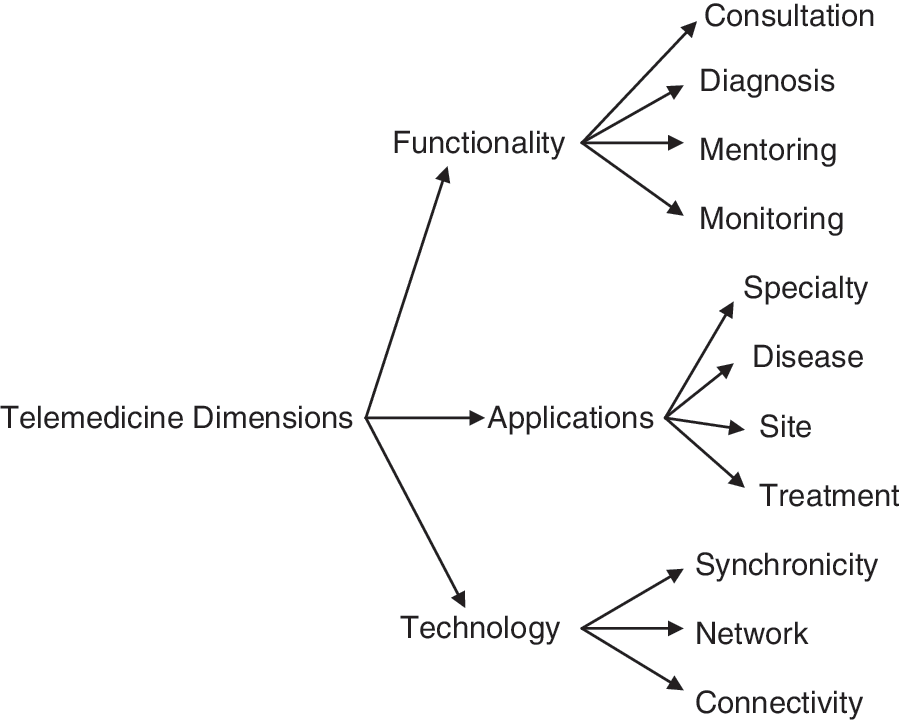
Based on the telemedicine experience to date, as illustrated in Figure 5, the various configurations in the field can be initially grouped into three aspects or dimensions, namely, the functions that are performed (labeled here as functionality), the specific applications, and the technological configurations. This classification constitutes the first, or most inclusive, level of generality in the taxonomy of telemedicine. The second level of the taxonomy consists of the specific components and subcomponents of each of these dimensions. Ultimately, the two levels are combined to comprise a multidimensional taxonomy.
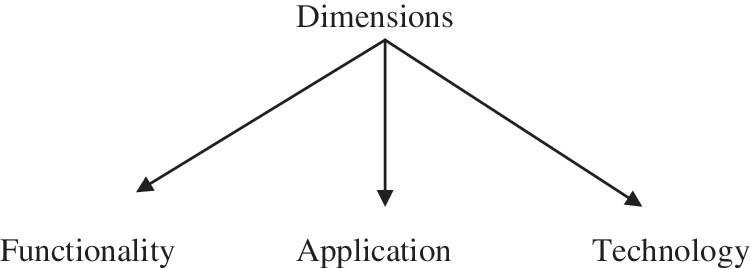
The dimensions of telemedicine dimensions.
In the following section, we attempt to identify the specific components of each of these dimensions.
Functionality
This dimension incorporates all aspects of the medical care process, including activities involved in prevention, diagnosis, treatment, follow-up, and rehabilitation. These aspects are grouped into four component parts (Fig. 6), consultation, occurring between two or more physicians (often between primary-care and specialist physicians) as well as between provider and patient. Diagnosis typically takes place remotely by a radiologist, pathologist, cardiologist, or other specialist relying on transferred images, records, and laboratory results. It should be noted that consultation and diagnosis are not mutually exclusive as both functions can occur during the same encounter. Moreover, both applications incorporate all aspects of the medical care process, as mentioned earlier. Monitoring includes telehome care for home-bound chronically ill, recently discharged persons requiring continued skilled care, wound-care patients, as well as those who are not home bound but have chronic conditions such as congestive heart failure, chronic obstructive pulmonary disease, asthma, and/or diabetes. This also includes other forms of telemetry in settings such as intensive care units. Finally, mentoring includes remote guidance typically by surgeons and other specialists to other surgeons performing new or complex procedures. Of these four, mentoring is the least developed to date.
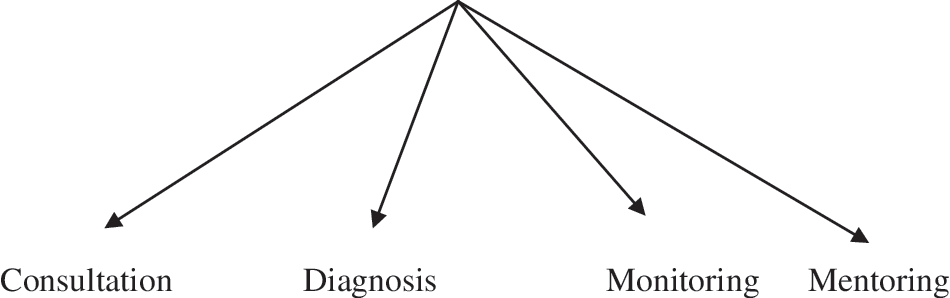
Components of the functionality dimension.
Application
This dimension includes processes of care across virtually all basic medical specialties, as well as subspecialization based on disease entities, sites of care, and treatment modalities (Fig. 7). Obviously, some of these categories are overlapping as medical specialization often incorporates multiple specialties. Nonetheless, they are separately listed here to reflect the vast array of these applications and the complexity of medical practice and medical specialization.
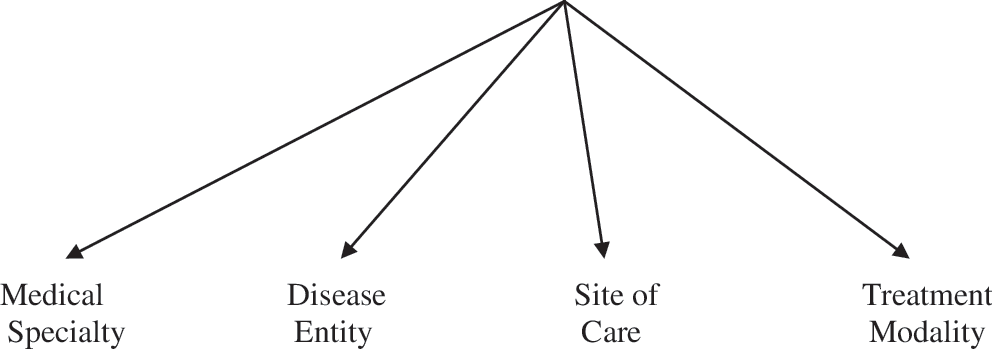
Components of the applications dimension.
The trend over the years has been one of increasing specialization and subspecialization in medicine in response to scientific and technological advances. The knowledge and skill involved in treating children with epilepsy, for example, are so great as to be out of reach of the physician in a primary-care setting. The same trend toward specialization is reflected in telemedicine, in which basic specialties include content areas such as teledermatology, teleradiology, and telepsychiatry. Some telemedicine applications have been developed around specific diseases, including diabetes, stroke, and posttraumatic stress disorder. Programs also may differ by site of care, including the intensive care unit, outpatient psychiatry, the emergency department, and the home. Some programs have been organized around specific treatment modalities such as rehabilitation (e.g., speech/language pathology, physical therapy) and pharmacy.
Further explication is required to sort out the specific nature of each application. For example, in emergency neurology and the evaluation of suspected cerebrovascular accident, images of the patient and of the brain may be important in the evaluation of a stroke. In some locales, Emergency Medical Services personnel (paramedics and emergency medical technicians [EMTs]) have ambulances equipped with a mobile computed tomography (CT) scanner. Obtaining and transmitting CT scans prior to arrival at the hospital allows the emergency department to mobilize certain processes and decide on the appropriateness of anticoagulants such as tissue plasminogen activator, in a situation in which elapsed time to intervention is a strong determinant of outcomes. The same type of convergence occurs in other “team care” situations. The classification is further compounded by the fact that these components contain subcomponents. For example, telerehabilitation encompasses physical therapy and speech/language pathology.
The Technology
The components of the technological dimension can be grouped into three sets of variables: synchronicity, network design, and connectivity (Fig. 8). Synchronicity is used here to incorporate both timing and technology. With regard to timing, telemedicine may be either synchronous (i.e., in real time), referring to the concurrent presence of interacting participants located at different places; or asynchronous (store-and-forward), in which the participants do not interact in real time. Both modes involve a variety of technologies, including videoconferencing, telemetry and remote sensing, and other modes of interactive health communication. Network design/configuration includes three modalities: Virtual Private Networks, the open Internet, and social networks, in which information is posted and shared. The three modalities substantially vary in terms of security arrangements and the ability to protect confidential information such as that required by the Health Insurance Portability and Accountability Act of 1996. However, all may be enabled by two types of connectivity, wired and wireless, both of which now provide different levels of bandwidth and the attendant speed and resolution or quality of service.
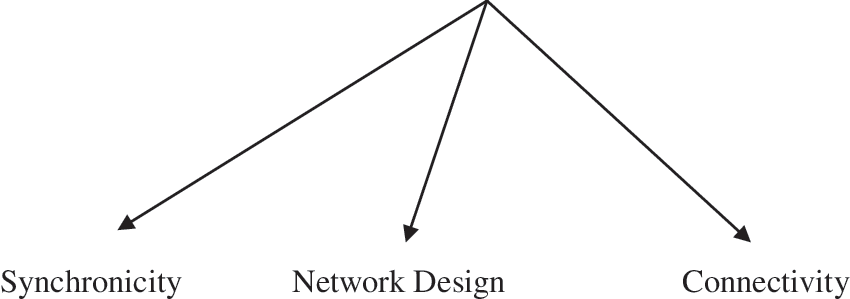
Components of the technological dimension.
Three-Dimensional Model
The taxonomy of telemedicine can be presented in several different ways, most notably either as an embedded hierarchy, shown in Figure 9 in abbreviated form, and as a three-dimensional model, shown in Figure 10. The former form has the advantage of showing the hierarchical derivation of the concepts, an inherent quality of taxonomies. The latter is a simpler, possibly more practical, guide for research purposes.
Dimensions of telemedicine and components.
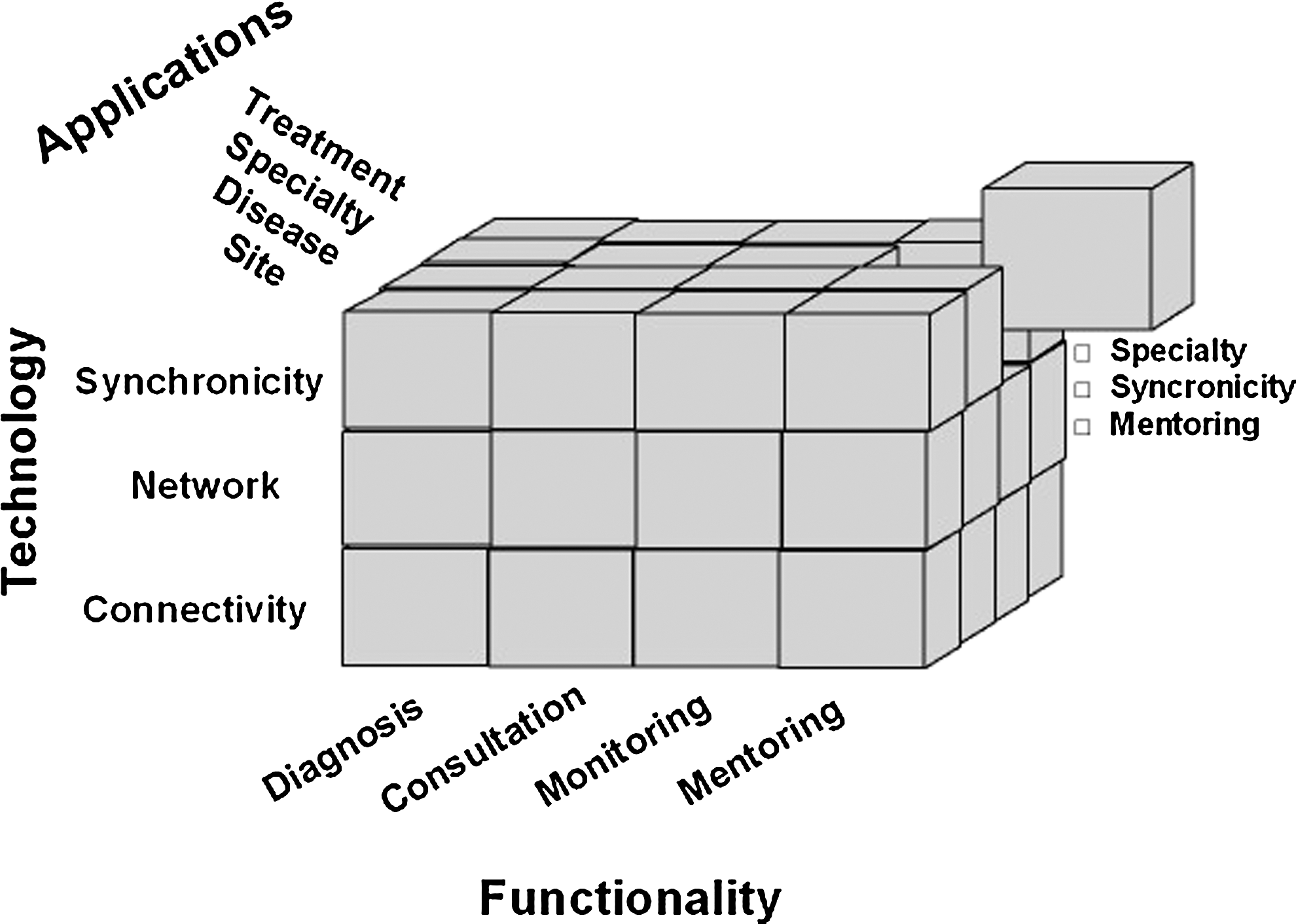
A three-dimensional model for telemedicine.
Figure 9 provides a heuristic representation of the hierarchy, starting with the three dimensions of telemedicine and the components of each dimension. Not shown in this figure are the constituent parts of each component. Figure 10 combines this information into a single three-dimensional model. Both representations could be used in the initial stage of operationalizing the specific nature of an intervention under investigation and its measurement. Similarly, both models allow for further specification of the independent variables (measuring the target intervention at the appropriate level of granularity or specificity) as extensions of the model and as indicated by the research objectives. This is particularly relevant where certain components (such as applications) consist of a large number of constituent parts, including medical specialties and subspecialties. However, it is not necessary to include this level of detail in the graphical depiction of this taxonomy as it would render it unmanageable. In fact, the user of the model should exercise judgment as to the appropriate level of detail necessary to test target hypotheses. Therefore, for parsimony and clarity, we limit the taxonomy to three basic dimensions and their respective components. Unavoidably, the final placement of nonoverlapping components under their respective dimensions may not be possible without empirical testing of this model.
The simplest way to use the model is to select or isolate one cube and subsequently identify all variables of interest on the basis of their derivation from three dimensions of the cube, that is, application, technology, and functionality. For instance, beginning with application, one might substitute a specific clinical specialty such as telepediatrics for the generic “application.” The second step consists of identifying the specific component of the technological dimension for this application, followed by the specific component of functionality. This process can be illustrated further with concrete examples from the published literature. The examples are selected on the basis of our familiarity with the details of the research design. They should provide the reader with additional insight as to using the taxonomy for approaching and developing a research problem.
The first example is a study by Cruz et al., 21 designed to assess the effects of camera resolution and bandwidth on facial affect recognition—an important process and clinical variable in mental health. In terms of the taxonomy's functionality dimension, the study was concerned with the consulting and diagnosis components. From a diagnostic perspective, psychiatrists use nonverbal expressions as cues to the internal affective state of an individual, which aids in identification of pathologic processes in cognition, mood, and motor functioning (related perhaps to factors such as agitation or drug side effects). The application dimension in this instance is clearly telepsychiatry. The technology involved two components—synchronicity (as only real-time videoconferencing was studied) and connectivity. The connectivity component was reflected in the comparison between a one-chip VHS-grade camera and a three-chip Beta-grade camera as well as two bandwidths with each camera (768 vs. 128 kilobits per second).
A study by Johnson et al. 22 focused on the effects of data compression on diagnostic accuracy of virtual pathology slides. The functionality dimension was diagnosis as pathologists viewed and compared a series of benign and malignant frozen section breast biopsy specimen. The application dimension addressed two variables—medical specialty (telepathology) and disease entity (breast cancer). It is an empirical question whether compressing these types of specimens may yield different results than those resulting from compressing bladder biopsy specimens, for example. Finally, the technology dimension focused on connectivity given that one of the main reasons for examining the effects of compression is to assess the feasibility of lower bandwidth vis-a-vis loss of information. Uncompressed virtual slides require substantial bandwidth for efficient transmission. If they can be compressed without sacrificing diagnostic accuracy, lower bandwidth could be used at lower cost.
A final example 23 compared cancer patients in two groups, all with an ostomy upon hospital discharge. One group received “traditional” home healthcare after being discharged from the hospital. The other received a combination of traditional home health augmented by nursing. In this case, the functionality dimension of interest was monitoring as the task of home health nurses was to monitor patients' adjustment to and care of the ostomy. The application dimension was primarily treatment modality (traditional vis-a-vis hybrid nursing), although site of care (home only versus home + remote video) and disease entity (cancer ostomy) were secondary components in this study. The technology component was less prominent in this study but did touch upon connectivity as telemonitoring used a home health unit connected to regular phone lines that provided two-way video and monitored physiologic functions such as blood pressure.
Summary and Conclusions
Given telemedicine's proliferation and progress to date coupled with the almost universal adoption of ICT in all sectors of society, including health, there is little or no doubt regarding its continued growth, advocates' concern about its slow diffusion notwithstanding. It seems evident that some time ago, the point of no return was crossed in telemedicine development based upon the extensive reliance by healthcare institutions on ICT in various facets of care delivery, including electronic health records, appointment scheduling, billing, and the emerging use of clinical decision support systems and medication prescribing. Even as we acknowledge the slow diffusion of telemedicine, it is hard to imagine how a modern health system can function without ICT. Nonetheless, we stand on the cusp of major change and innovation in telemedicine and in healthcare generally, and we only have glimpses of what the future will bring. The research we do today and the empirical and experiential knowledge we accumulate are bound to affect both the shape of the future and the speed with which we approach it.
The current confusion in the nomenclature and classification hinder telemedicine research and implementation. Regarding research, it frustrates our efforts to reach a reasonable understanding of what we already know and what we need to know. Equally important, it impedes progress toward development and implementation of a research agenda geared toward reaching answers to questions regarding the true benefits and costs of telemedicine. Regarding implementation, the lack of clarity interferes with informed and prudent decision making by policymakers, payers, program developers, and providers.
The scientific foundation of telemedicine is going to depend on our ability to (1) articulate a clear operational definition of the concept of telemedicine with all its complexity and facets, explicitly describing what it is and what it is not in precise terms, as well as explicating its component parts, (2) identify theoretically relevant units and objects of analysis and specify how they should be measured, (3) deploy telemedicine systems in full fidelity and specificity to ensure that we have the proper reference to telemedicine when we use the term in research and/or in policy development and implementation, (4) employ robust research methodologies, including randomized clinical trials to measure its true clinical and economic effects, and finally, (5) produce the necessary scientific and policy-relevant evidence not only to confirm its merit (of lack thereof) but also to identify current inadequacies and problems that must be remedied or alleviated to move the field forward.
It is time to pursue clarity and consensus regarding what constitutes the content of telemedicine, telehealth, e-health, and m-health, as well as the substance of other new conceptualizations and the related neologisms that may emerge. We are beginning to see other neologisms in use, such as “connected health” (or c-health) and “ubiquitous health” (or u-health). These have varying degrees of utility. The term i-health (or Internet health), for example, did not get much traction and failed to catch on. On the other hand, informatics, the science of collection, classification, storage, retrieval, and dissemination of information, is now incorporated in academic curricula. Health informatics is a subset of informatics. Bioinformatics is gaining recognition for solving problems in the life sciences and the creation of extensive biological databases for genomes, protein sequences, and the like. 24
Some terms have been advanced by academicians or professionals and some by business or commercial interests. Each new term should be justified on the basis of some unique attribute(s). Regardless, we need to understand the differences and commonalities between these terms, and it remains to be seen whether proliferation in nomenclature will ultimately contribute to a better understanding of the field or add to the confusion. Those of us who stubbornly hold on to the telemedicine label continue to believe in the dynamic nature of medicine and medical information whether delivered in person or at a distance.
We hope that the proposed taxonomy presented here will not only clarify the proliferation of nomenclature in telemedicine, but also, more importantly, provide a useful guide for research and policy making. Like other taxonomies, the one proposed here is not intended and it cannot be a finished product. Instead, we offer it to subject matter experts in various aspects of telemedicine for their assessment, testing, revisions, and verification. As suggested by NASA, “a good taxonomy is not perfect.” 25 It is best developed as in an iterative fashion, while engaging a wide range of content types. That is how the telemedicine taxonomy will bear fruit.
Footnotes
Acknowledgments
The authors acknowledge with gratitude several colleagues who read earlier drafts of this manuscript and offered valuable comments and ideas for its improvement. In alphabetical order, these include Michael Ackerman, David Bott, Charles Doarn, Donald Lindberg, Ronald Merrell, Tim Reardon, and Jay Sanders.
Disclaimer
The authors state that they did their best to address the concerns and issues raised by the reviewers. The authors, however, declare that whatever problems or errors remain in this document are entirely their own responsibility.
Disclosure Statement
No competing financial interests exist.
*
This follows an earlier attempt to develop a taxonomy of telemedicine. See Tulu B., Chatterjee, S, and Maheshwari, M., Telemedicine Taxonomy: A Classification Tool. Telemedicine and e-Health 2007; 13(3): 349-358.