
Abstract
Background
Ensuring equal access to good quality healthcare remains a core aim of the National Health Service. 1 Effective communication between patients and healthcare staff is key to the delivery of this aim. Traditionally, communication occurs by face-to-face contact or written correspondence. However, there has been increasing interest in the use of simple digital communication technologies (including mobile phone and texting, e-mail, and the World Wide Web). These technologies have the potential to be more rapid, responsive, and cost-effective in improving the quality of healthcare by enhancing the level of communication across organizational boundaries of healthcare provision, such as the primary–secondary care interface. Communication problems across this interface have long been identified as a source of frustration to patients and clinicians alike. 2 Furthermore, studies have shown that using such technologies can produce care clinically similar to that from face-to-face consultations with health professionals, improve patients' access to care, and reduce hospital and travel costs. 3
Overcoming geographical barriers to access is one of the principal challenges for providing health services to remote and rural areas. 4 However, despite the promise of the “digital age,” its full potential in terms of healthcare and improved access to healthcare is not currently being realized. This is likely because of a variety of reasons, including technology limitations, although lack (or perceived lack) of technology skills and confidence in both patients and healthcare providers remains a major barrier to more widespread use. 5,6
There has been a considerable increase in the use of communication technologies within the general public, and while it might be assumed that general skill levels are high, there are few published data on patients' knowledge and skills in this area. Specific training may overcome skills deficiency, but it remains likely that the successful widespread implementation of new technologies into healthcare services will depend in a large part on the existing abilities of patients and healthcare providers.
This study aimed to assess the perceived usage of, and attitudes toward, communication technologies (mobile phone and texting, e-mail, and the Web) in patients attending a cardiology clinic with a view to guiding future health service redesign.
Materials and Methods
Setting
Raigmore Hospital is situated in the north of Scotland (Highland Region) and serves a population of over 300,000 dispersed over a large geographical area (10,085 square miles). Approximately 70% of patients live within 1-h travel time from the major hospital with good roads and public transport, but much of the rest of the population have considerable geographical hurdles to attending the clinic, including transport by plane and ferry from island locations. There are no peripheral specialist cardiology clinics in this area, and therefore all patients travel to Raigmore Hospital for specialist cardiology review.
Design
A self-completion questionnaire-based survey was conducted on a convenience sample of patients attending a general cardiology clinic between February and May 2009. All patients attending the clinic were included, and questionnaires were distributed by the clerical staff at the clinic. These were adult patients (>16 years old) with a range of cardiologic conditions. This included “new” and “return” patients.
Questionnaire Design
In the absence of a validated instrument a questionnaire was developed de novo in several iterative stages including a pilot study (n=80) (data not shown). The results from this pilot study allowed further questionnaire redesign until the final version was agreed upon (see Appendix). The questions asked about patients' access to and use of technology at home. Most questions required a yes/no response or used a 4-point rating scale. Respondent data included age, gender, travel time to the clinic, mode of travel, and whether the respondent was accompanied to the clinic.
Ethical Considerations
The opinion of the North of Scotland Ethics Committee was that this survey represented service evaluation rather than a research study, and therefore full ethical approval was not required.
Data Collection and Statistical Analysis
Data were transposed from self-completed paper questionnaires into a Microsoft Excel spreadsheet. The p values using an appropriate statistical test were used to assess the influence of age (unpaired t test), gender (chi squared test), and distance from the hospital (unpaired t test) on the use of the Internet, mobile phone, text messages, and e-mail. For testing frequencies of usage for each technology analysis of variance was used. Significance was taken at the 0.05 level.
Results
Patient Demographics
In total, 221 patient responses were studied. One hundred twenty-four (57%) were male. The average age was 62.1±14.1 years (range, 16–89 years). The self-reported places of residence were as follows: countryside, 40 (18%); city, 77 (35%); town, 36 (16%); and village, 68 (31%). The median travel time to hospital was 30 min (range, 0–1 h). The majority (172 [78%]) of patients used private transport to attend hospital, 23 (10%) used public transport, and 7 (3%) used hospital transport or ambulance.
Technology Usage
The majority of patients had a CD or DVD player at home (166 [75%] and 163 [74%], respectively). Many patients (136 [62%]) had a home computer, and 111 (50%) (Fig. 1) reported having broadband access. Communication technology usage is reported in Table 1. For patients (n=179) who reported on the strength of mobile phone signal in their house, the quality of reception was reported as good for 111 (66%), variable for 43 (25%), or none for 15 (9%). With regard to patients' overall use of the four means of communication technologies, 14.0% never use two out of the four, 14.7% never use three out of the four, and only 0.7% never use any.
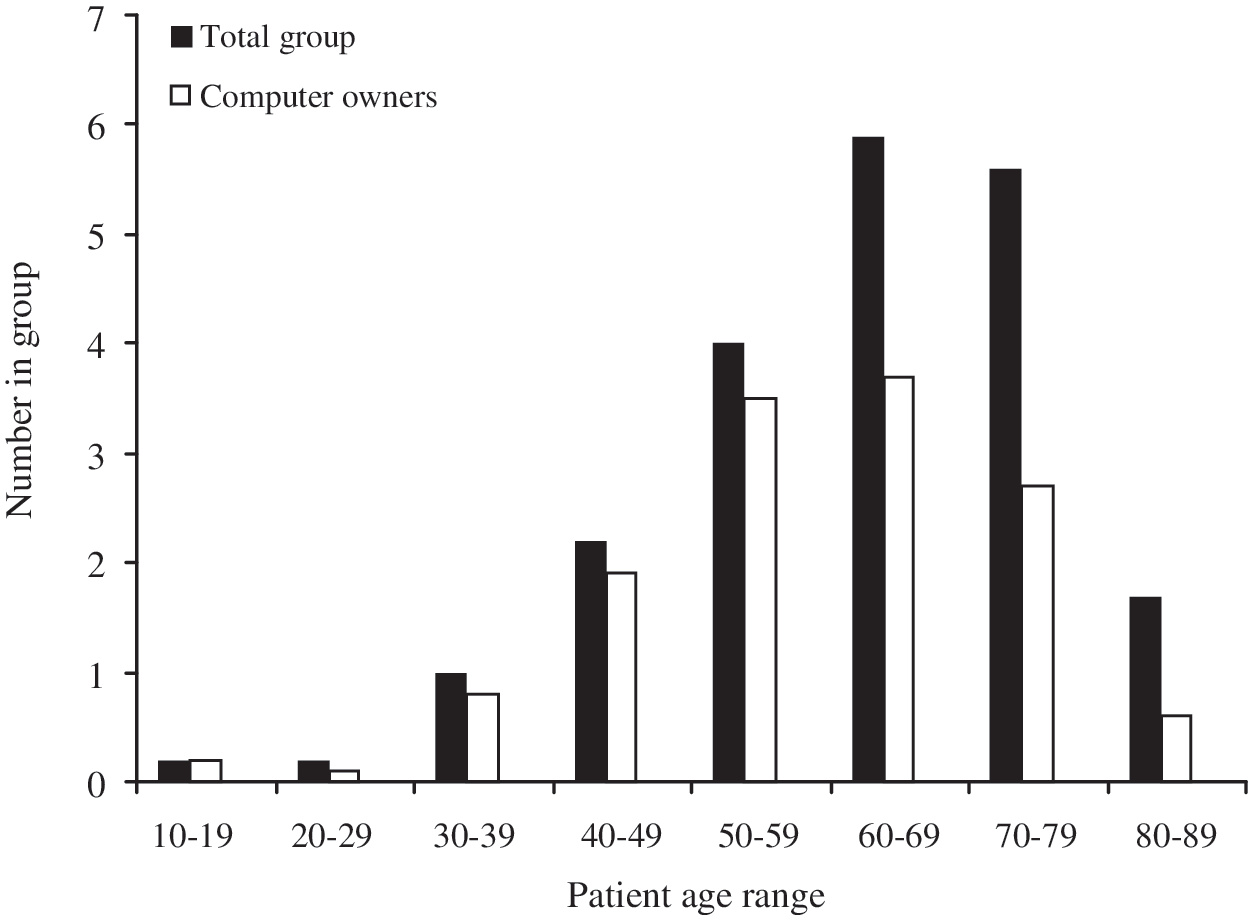
Age and home computer ownership frequency histogram.
Frequency of Technology Usage
The majority of unreported respondents had answered negative to having this technology available.
Influence of Age Gender and Distance from Hospital on Use of Technology
Gender and distance from the main urban center were not related to use of the Internet or mobile phone usage (or mobile texting function) (all p>0.05). However, age was closely correlated with usage of communication technologies. On average, participants who used the communication technology were younger than those who did not for the Internet (56±14 versus 68±10; p<0.001), mobile phone (59±14 versus 73±12 years; p<0.001), mobile texting function (54±13 versus 68±10 years; p<0.001), and e-mail (56±14 versus 69±11 years; p<0.001).
Furthermore, age was found to be a key factor in determining the frequency of use of mobile phones (p<0.001) and texting (p<0.001) but not the frequency of using the Internet (p=0.43) and e-mail (p=0.76).
Desire to be Able to use E-mail to Contact the Doctor or Nurse
Many respondents (80 [36%]) reported a wish to contact a doctor or nurse between clinic appointments by e-mail, 93 (42%) did not wish to do this, and the remainder did not respond to this question. Patients who had a computer at home were much more likely to wish to use e-mail between appointments compared with those patients without a computer at home (76/136 [56%] versus 3/78 [4%]; p<0.001). Once again, age was a key factor in determining whether patients desired to use e-mail to contact a doctor or nurse (p<0.001).
Discussion
Increased use of communication technologies has the potential to improve patient care. 7 Implementation of these can be difficult, and patient skills and confidence with them will vary. Within the variables investigated in the present study, age was the strongest predictor of use of communication technologies (mobile phone and texting, e-mail, and Internet). Age was also a predictor of frequency of use of mobile phone and texting but not for e-mail and Internet. Patients who lived in more remote areas were no more likely to use communication technologies than those who lived in more urban areas.
Successful and widespread implementation of communication technologies in healthcare is likely to depend on part on the availability within the general public. In our cohort only 62% of patients had a home computer, and only 50% had broadband connectivity, and this is likely to limit the immediate ability to develop Web- or e-mail-based healthcare solutions to the majority of our population. However, the proportion of younger patients with computers is much higher, and as this cohort of patient ages there will be an increase in the proportion of patients with access to computers and mobile phones and the skills to use them.
The potential benefits for the delivery of healthcare services by greater use of technology are considerable. Traditional face-to-face medical outpatient clinics are a common way of assessment and monitoring patients and have been in place for many years, but many patients are seen in the clinic with little or no positive outcome in terms of treatment decisions, with some patients being seen as a matter of “routine.” 8 Thus, traditional “doctor-led” clinics may not be an efficient model of care. Alternative methods for reviewing patients may include telephone consultations, telemedicine, e-mail, or other Web-based communication. These are of particular interest in remotes areas where long distances can exist between patients and their healthcare providers.
Rural Issues
Access to healthcare professionals is more difficult in remote areas for a variety of reasons. 9 The most recent Scottish Household Survey highlights that less than half of people in remote rural areas find access to hospital outpatient departments “very or fairly convenient”; public transport is also an issue, with 51% of remote and rural areas stating public transport services are convenient compared with 88% in large urban areas and 79% in accessible small towns. 4 Distance from specialists and specialist facilities—for example, cardiac catheterization facilities—is inversely proportional to the likelihood of patients receiving specialist investigation. 10 In some cases (e.g., chronic heart failure) this can result in poorer outcomes for patients in remote areas. 11 However, there is an increasing awareness that technology may help overcome barriers to healthcare delivery and equity of access particularly in remote areas. 12
The Role of Teleclinics and Communication Technology
Teleclinics and communication technology use may be of most benefit to rural patients in that they greatly reduce or abolish travel times. Instead of patients requiring days off work to attend a clinic, they can potentially receive specialist clinical review via videoconferencing at a local venue. Furthermore, between formal clinic appointment times, it may be difficult to reach a physician at a convenient time for both physician and patient. The use of e-mail or Web-based communication may better enable communication between the patient and the doctor, obviating the necessity of both parties being available at the same time. This potentially could increase adherence to treatment plans and thus improve overall health. In one study in patients with congestive cardiac failure, the introduction of telemedicine increased medication compliance and improved physical and mental well-being at a relatively low cost. 13 In cases where individuals do not have Internet access the nearest healthcare centers may facilitate contact between the patient and hospital doctors, and where there is a lack of patient skills this could be facilitated by local healthcare professionals (e.g., community nurses).
Acceptability of Telecommunication
Acceptability of new services will be important in their subsequent implementation. The use of text messages to remind patients for hospital appointments in pediatric services in Hull resulted in a decrease in nonattendance. It is important that over 90% of these patients were happy to receive a text reminder of appointments. With regard to videoconsultations a review of patients using psychiatric services noted that some patients preferred videoconferencing compared with traveling to the clinic. 14 Although some individuals perceive such appointments as impersonal, they felt that an adequate doctor–patient relationship was established. This was particularly the case in patients who were previously known to the doctor where a relationship had been formed prior to the videoconferencing appointment, 14 suggesting that videoconferencing may be more appropriate for review patients rather than new patient consultations. Nevertheless, the benefits of more frequent or convenient communication with a doctor appeared to be more important than potential subtle reductions in quality of consultation (i.e., the patients were less affected by the way in which doctors interacted with them but rather whether this interaction occurred at all). 15
However, telecommunication is obviously less robust in terms of physical examination, and there is a danger that physical signs will be missed. 16 Furthermore, patients and physicians share some concerns regarding communication technology. 17 Security and confidentiality are a particular concern with e-mail and Web. Physicians report concern regarding developing a good rapport with patients and the danger of missing nonverbal queues, although case selection should reduce these risks. In some instances physicians feared that the introduction of telemedicine would increase clinical workload. This concern was surrounding the hours that would be spent reviewing e-mails and responding to individuals. 18 Good documentation of working practice and appropriately supported service redesign should address these issues.
Implications for Older Patients
This current study has demonstrated that older patients are less likely to use communication technologies in day-to-day living, and there is a concern that older patients will be denied the benefits from using healthcare technologies. However, studies have shown that if support is given, new technologies can be successfully used even in very elderly populations. 16 Another concept is that of “tele-assistance” where individuals in the community facilitate communication between physicians via telemedicine; these individuals could be community nurses, general practitioners, or others, although using non-healthcare professionals may be ethically challenging, and confidentiality of patients should always be protected.
The Future
The use of technology in daily life is likely to continue to increase and with it the proportion of the population with specific communication technology skills. Already there are many examples of the use of communication technology in the delivery of healthcare (e.g., mobile phones, online booking, and repeat prescriptions). However, many of these technologies have been used in younger patients (e.g., young diabetic patients) and therefore may not be so easily implemented in a general clinic population—indeed, in our cohort age was the dominant influence on the use of communication technologies. Furthermore, high-tech monitoring of patients both in the hospital and in a non-hospital setting will continue to be developed. 19,20
Limitations
This was a single center study, and therefore the results may not be applicable to other centers. Nevertheless this was a study of all comers and therefore represented a breadth of patients in terms of age and geographical locations. Indeed, although other studies have investigated the use of technologies in younger patients, our cohort was unselected and therefore represents a more general cardiac clinic population. A further potential limitation is that this questionnaire was delivered prior to the patient attending the clinic, and the subsequent clinic visit may have had an influence on the views and responses of patients, in particular the desire to use technology when communicating with healthcare professionals. The communication technology skills of our healthcare staff have not been assessed.
Conclusions
This study has identified that the use of communication technologies is not widespread within the cardiology outpatient community. Age is the strongest predictor of use of communication technology, with younger patients more likely to use e-mail, the Web, mobile phone, and texting. This study has highlighted that there may be several potential barriers to the widespread implementation of communication technology to a general cardiology clinic population. Cognizance should be taken of these findings when attempting service redesign.
Footnotes
Disclosure Statement
No competing financial interests exist.