
Abstract
Introduction
Telehealth is the delivery of healthcare services from a distance, using information and communication technology (ICT). It became a separate field of study in the 1970s, 1 but its innovation experienced a major increase in the 1990s, primarily due to the development of new technologies such as cellular phones and the Internet. 2 The field was originally known as telemedicine but has been expanded to telehealth, although these terms continue to be used interchangeably. 3 U-health, e-health, telehealth, and telemedicine are all closely related in concept as a healthcare service because the terminologies were coined to refer to a system of healthcare services using ICT. “U-health” is short for “ubiquitous healthcare,” and this widely used term has substituted for the terms “telehealth,” “telecare,” “telemedicine,” and “e-health” in Korea. It is similar to the previously used terms but has a more comprehensive meaning, encompassing concepts such as the ability to deliver healthcare services using ICT in the five domains of space, time, provider, consumer, and type of service 4 in more expanded meaning compared with the traditional healthcare. For example, it encompasses the concept of anywhere, anytime, anybody, and all kinds of health information technology.
Telehealth technology is being increasingly incorporated by home agencies in the management of chronic diseases, which are one of the main causes of death in almost every developed country. 5 Among them, chronic obstructive pulmonary disease (COPD) affects an estimated 210 million people globally and causes some 3 million deaths annually. 6 COPD creates a serious burden on patients, providers, and healthcare systems. 7 It has been shown that telehealth services are effective in preventing hospitalization and visits to an urgent care unit and even in extending the patients' predicted lifespan. 8 –12 One clinical experiment suggested that integrated home telemedicine services and care coordination can support health professionals working with COPD patients and significantly improve the patients' health. 13 The use of ICT offers considerable advantages: (1) It automatically records all the interactions with patients (including phone calls) and schedules follow-up visits in the case of untreated symptoms. (2) The care team can have ubiquitous access to the most up-to-date patient information, allowing for improved care coordination. (3) The number of patients who can be provided with closer follow-up increases without increasing the workload of health professionals (specialists and case managers). It is likely that without the technological advances in information and communication, such a high degree of personalized patient care services would not be possible.
However, the success of u-health services is closely related to how well patients adopt and utilize the technology. There has not been a thorough study on the relationship between the level of effectiveness and its acceptability by the patients, particularly in regard to COPD patients, even though the benefit of such a study on further development and integration of u-health services is undeniable. Therefore, this study investigated the level of u-health service acceptance by COPD patients, their satisfaction, and additional desired functions, particularly with the currently provided service of telephone education and home visits.
The questions this research aimed to answer were as follows: 1. How well is the u-health service accepted? 2. What is the overall satisfaction level of COPD patients who use the u-health services, that is, tele-education and home visits? 3. What are their expectations regarding u-health services? 4. What cost of u-health services do patients consider acceptable?
Subjects and Methods
This study measured the acceptability of u-health devices and their major functions, specifically, telemonitoring, tele-education, and home visit services. The acceptability was quantified by the patient satisfaction level, intent to use the services, and the cost they were willing to pay for the service. A variation of a quasi-experimental design was used to classify the subjects into the following three groups: Experimental Group 1 (EG1) only received status monitoring services through u-health devices, Experimental Group 2 (EG2) received the monitoring services as well as the u-health device and mobile phones (audio services), and Experimental Group 3 (EG3) received all of those services as well as video phones (video services). Patients were asked by their physicians to participate in the study and received basic education regarding u-health services and the measurement devices from outpatient nurses. Within 1 week of the nurses' initial visits, technicians installed the u-health devices in the subjects' homes, and nurses visited again to provide follow-up education and conduct the initial survey. EG3 subjects, because of the additional video services they received, required a separate visit from a local telecommunication company, and these individuals received biweekly tele-education services from a specially trained nurse. Six months after the start of the study, all subjects were visited by a nurse for a secondary questionnaire survey.
Research Subjects and Experiment Design
The research protocol was approved by the Institutional Review Board of a tertiary-level medical institution affiliated with a university prior to choosing the research subjects, who were 207 patients diagnosed with COPD and receiving treatment from the hospital's respiratory internal medicine department. Each patient's attending physician explained the advantages and disadvantages of participating in this study and then received the patient's consent. The criteria for participating in this study were as follows: the patients were in Stages I–IV of COPD diagnosis, their status monitoring could take place regularly, their physical state was relatively stable, and they were able to undergo basic tests and operate the monitoring devices. Among those who met the criteria, patients who (1) experienced difficulty in carrying out their normal day-to-day routines because of aggravated respiratory symptoms, (2) could not receive outpatient tests and tracking, (3) resided alone (safety liability), (4) had a history of mental illness, and (5) could not operate medical and communication devices were excluded from the study. Study subjects were assigned to one of the three experimental groups by random draw. Among the initial 207 subjects who began the study, 144 subjects were able to continue their participation, and 63 subjects were excluded from the study because of reasons such as withdrawing their consent, early withdrawal (within a month after the starting of the experiments), exacerbation of disease, inability to manage the monitoring devices, and terminating communication.
To ensure consistency, the experimental protocol was standardized and distributed among the research staff (Table 1), and the methodology was specifically developed for data collection (Table 2). The overall workflow of u-health services is shown in Figure 1.
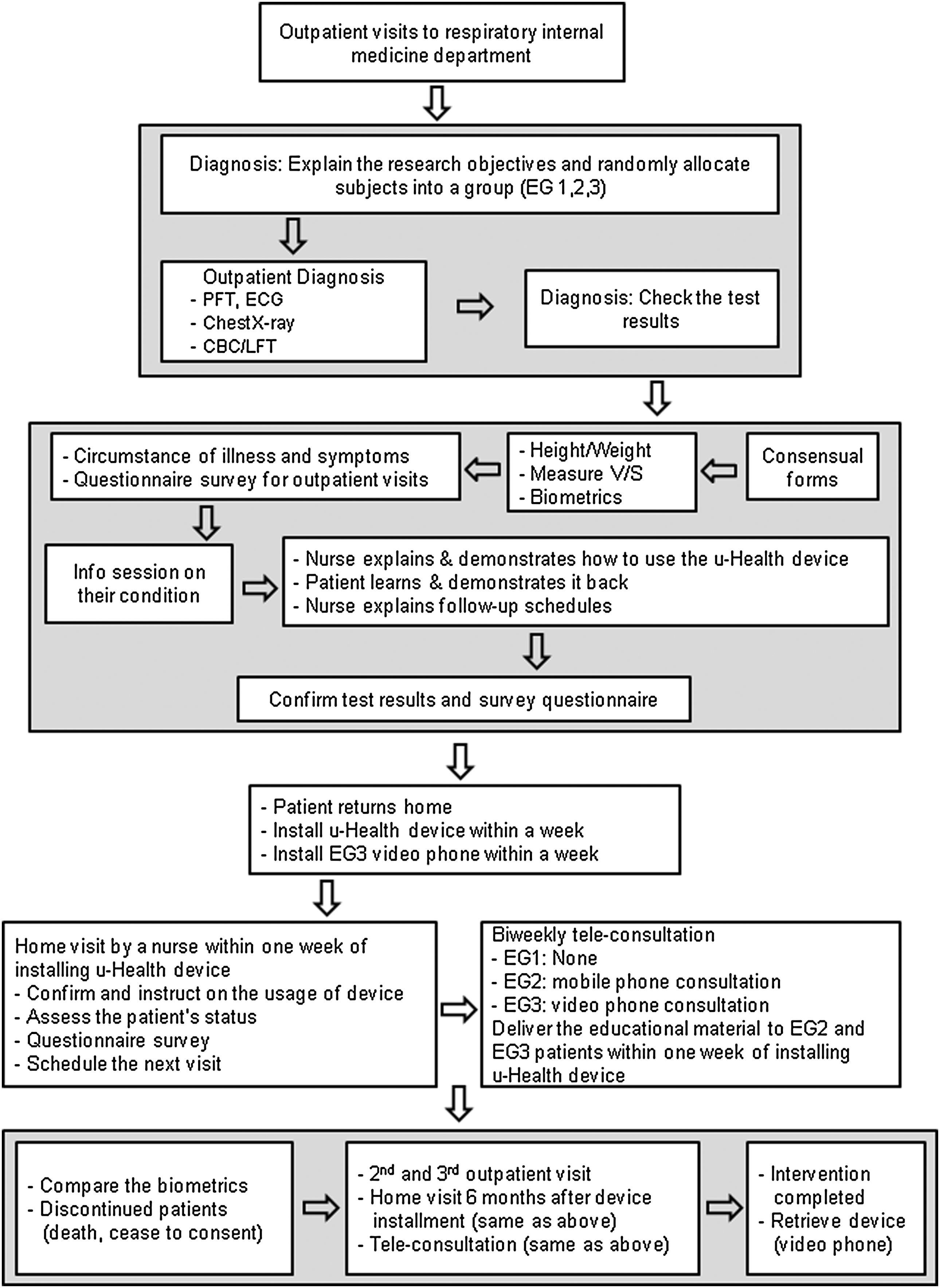
Workflow of chronic obstructive pulmonary disease u-health service. CBC, complete blood count; ECG, electrocardiogram; EG, experimental group; LFT, liver function test; PFT, pulmonary function test.
Standardized Experimental Protocol
Measurement Tools for the Research
COPD, chronic obstructive pulmonary disease.
The teleconsultation specifications and protocol were as follows:
1. The objectives of teleconsultation
a. Assess problems and challenges regarding the COPD patients' u-health devices after installation. b. Comprehend the needs of each patient. c. Provide emotional support.
2. Methods of teleconsultation
a. Regular teleconsultation (once a month). The teleconsultation nurse contacts the patient once a month through the patient's mobile phone or video phone, assesses the challenges, and educates the patient. b. Unscheduled teleconsultation (inbound calls, on-call). Patients contact the teleconsultation nurse when they have specific questions regarding their symptoms and devices. 3. Teleconsultation protocol. The algorithm for teleconsultation sequences is shown in Figure 2,
14
and a sample telephone triage algorithm is shown in Figure 3. The detailed protocol used in the actual teleconsultation is shown in Table 3. The content of teleconsultation is shown in Table 4. Hard copies of the educational materials were distributed to patients via the postal service and were used at the time of the teleconsultation by both the nurses and the patients.

Algorithm for routine teleconsultation for chronic obstructive pulmonary disease (COPD) patients.

Algorithm for telephone triage for COPD symptoms. PCP, primary care provider; SOB, shortness of breath.
Protocol for Teleconsultation
Results
General Characteristics of the Subjects
This research started on November 1, 2008. The development and provision of the u-health device and services lasted for 2 years. The data collection began on July 2, 2009 and ended on December 31, 2010. The general characteristics of the subjects are shown in Table 5.
General Characteristics of Subjects (n=144)
EG1, EG2, and EG3, experimental group 1, 2, and 3, respectively.
Satisfaction Level in Home Visits
After the initial installation of the u-health devices in the subjects' homes, an initial home visit by a nurse took place within the first week, and a second home visit occurred 6 months afterward to survey the level of satisfaction with the home visit services of u-health. The majority of the 144 subjects answered “very satisfied” or “satisfied” as to whether they were satisfied with the service (Table 6). When asked what feature of the service was most helpful, 21 answered “the detailed explanation,” 15 answered “answers to their specific questions,” 17 answered “instructions on using the devices,” and 17 answered “emotional support.”
Satisfaction Level in Home Visits (n=144)
Satisfaction Level with Teleconsultation
After installation of the u-health devices in the subjects' homes, EG2 and EG3 subjects received teleconsultation, guided by the protocol, once every 2 weeks. After 6 months of service, the subjects were asked questions regarding their level of satisfaction, comfort, and need, as well as the helpfulness of the devices. The majority of the 66 subjects answered that they found the teleconsultation very satisfactory or satisfactory, showing a relatively high level of satisfaction with the service (Table 7). When asked what feature of the service was most helpful, 15 answered “the detailed explanation,” 11 answered “answers to their specific questions,” 5 answered “instructions on using the devices,” and 3 answered “emotional support.”
Satisfaction Level in Teleconsultation (n=66)
Additional participant comments and suggestions regarding the teleconsultation service included requests for detailed instructions on what to do when an emergency occurred, a monthly explanation on how to use the devices and interpreting the results, additional consultation depending on their symptoms, and 24-h consultation availability.
Inclination Toward Using U-Health Services
When subjects were asked whether they would be inclined to use u-health devices after the experiment ended, 75.7% answered yes (Table 8). Furthermore, they showed a high inclination toward using home visits and teleconsultation services.
Inclination to Using u-Health Services
N/A, not applicable.
Desired Fee for U-Health Services
The subjects answered that they would be willing to pay US $421.28 (450,000 KRW) for the u-health devices or rent the device at US $98.05 (100,000 KRW) per month. For the home visit service, they were willing to pay US $21.53 (23,000 KRW) per visit; for teleconsultation, US $0.53 (600 KRW) per minute or US $26.57(29,000 KRW) per month; and for overall u-health services, approximately US $44.26 (50,000 KRW) per month (Table 9).
Desired Cost for u-Health Services
Converted from KRW to USD based on the exchange rate as of June 7, 2011.
Discussion
Telehealth technologies are effective in the treatment and monitoring of COPD and are a proven alternative to conventional care systems. 19 COPD patients found the telehomecare program easy to integrate into their daily routines and that the program provided significant clinical benefits, particularly in the reduced number of home visits and hospitalizations. 20 –24 Interviews of elderly patients revealed favorable attitudes toward using telemedicine monitors, referring to the ability to quickly connect to a nurse and receive swift responses to their concerns and questions as a primary reason. It must be noted that both nurses and patients reported that telehealth technology in its current form should serve in conjunction with actual home visits by nurses to attain maximum benefits. Our study further verified the critical role of telehealth services, including monitoring and education, and its potential to supplement and replace a significant proportion of on-site health visits. 25 –27
Based on the continuous observation of the physician specializing in COPD who participated in this research, there was almost no symptom exacerbation of the patients during the research period. There were no emergency room visits or hospital re-admissions, which was a very interesting phenomenon. However, based on the data collected in this study, the authors cannot prove that the u-health initiative was the cause of this outcome. However, it appears that the psychological stability that is generated with the support of u-health services may have produced these positive results.
The following has been published by the u-Health Center affiliated with Seoul St. Mary's Hospital Catholic University, based on internal research results coupled with simulation research performed by an external institute. The u-healthcare reduced medical costs by an average of US $7,400 per person over the 35 years while increasing the average lifespan by 5 months on average, resulting in an overall predicted reduction of US $28,000 in healthcare costs. Although a robust return on investment analysis of COPD u-health services is outside the scope of this study, considering the positive predictions based on the research, u-health services for COPD are expected to bring similar benefits by reducing medical costs.
Compared with other studies, we understand that the contribution of our work is contained in the following: 1. The addition of telehealth to COPD patient care resulted in increased efficiency though the integrated platform and services. Initial home telemedicine experiences were based on specific services such as telemonitoring, telephone follow-up, or televisits. Follow-up research projects were designed to study the telemedicine program providing a combination of services tailored to the specific needs of each patient group and healthcare organization taking place through multiple visits.
28
In addition to studying the use of telemonitoring devices such as spirometry and pulse oximetry, this research investigated the benefits of integrating a peak-flow meter into the set of devices. The study showed that a composite u-healthcare service of telemonitoring and home visits is far more effective than the conventional tele- and Internet-based services, where a simple question-and-answer form of interactions take place. 2. Although past studies focused on the effect of telemonitoring interventions, insufficiently detailed data on interactions between the subjects and nurses were reported.
29
In this study, a standardized protocol and an algorithm for COPD patient education were developed in order to systematically investigate the effect of telemonitoring. Furthermore, the patient response data were quantified using a prespecified metric, and the workflow of the COPD u-health intervention was designed a priori to maintain consistency throughout the project. 3. Previous studies have focused on the economic analysis and minimization of cost in a general clinical context. However, the main technological barrier to the development of integrated home telemedicine systems is the high cost of telemedicine devices. Therefore, this study investigated u-health services with reasonable cost for COPD patients in South Korea directly through interviews with patients. The resulting data will contribute to further development and integration of home telemedicine systems for the general population of South Korea.
The authors agree that it is imperative to have a control group to verify the reliability and validity of the results for basic science. However, it is almost impossible to have a control group that is comparable to the experimental group, as there are numerous confounding factors surrounding and impacting the conditions of the experiments. Especially when the intervention is delivered by providing education, it is more feasible to conduct quasi-experimental research than pure experimental research. Also, it is very difficult and sometimes even unethical to allocate the subjects to the control group in a clinical situation. As such, characteristic of quasi-experimental studies, this research was limited by a lack of controls. Additionally, strict randomization of placing subjects into different groups was compromised, resulting in the lack of the assumption that variables were introduced into each experimental group uniformly. Therefore, it is recommended that when implementing the results of our research, these limitations as well as the general limitation of all clinical research (such as the difficulties in obtaining a patient's consent and randomizing the group assignments) must be considered. Considering these limitations, the results of this research could only be applied with confidence to populations with similar characteristics.
This study was the first to be conducted on COPD u-health services in Korea. The services are in the beginning phase, so it is not yet possible to perform a clear economic analysis. In the future, the authors plan to complete a full-fledged economic analysis of u-health services for chronic diseases, with the goal of proving the cost-effectiveness of u-health and therefore its eligibility for commercialization.
Conclusions
To quantify the acceptability of u-health services, this study investigated the level of satisfaction, inclination for ongoing use, and acceptable fee structure related to major u-health services such as remote monitoring and additional services including home visits and teleconsultations. 1. After 6 months of u-health home visits, the majority of the research subjects answered “very satisfied” or “satisfied” in regard to the quality of service, helpfulness, their level of comfort, and their needs. Their inquiries were resolved through home visits and detailed explanations and making available accurate instructions for device usage as well as receiving emotional support. All these factors contributed to the positive reception of u-health services. 2. Both the EG2 and EG3 groups showed high levels of satisfaction after using the u-health service for 6 months in regard to the service, their level of comfort, the helpfulness of the service, and their needs. Similar to home visits, the positive reception of home education services was aided by addressing their inquiries, providing detailed explanations, accurate instructions for device usage, and emotional support. 3. At the termination of the research, a high level of inclination was shown toward continued use of u-health services, including the devices, home visits, teleconsultation, and tele-education. 4. The acceptable fees for u-health services averaged US $421.28 (450,000 KRW) for purchasing the device and US $98.05 (100,000 KRW) per month for renting the device. For the other services, the desired fee was an average of US $21.53 (23,000 KRW) per home visit, US $0.53 (600 KRW) per minute for teleconsultation, and US $44.26 (50,000 KRW) per month for overall u-health services.
In conclusion, u-health service recipients showed a high level of satisfaction with in-home visits and teleconsultation and were highly inclined to continue receiving these services. Their positive reception was attributed to correct usage of the devices and active participation. Furthermore, by surveying the desired cost of the services, preliminary data for the economic aspect of u-health services are now available for future research and development. By effectively combining the home visit and teleconsultation services, the quality of u-health services will be improved, and increased efficiency is predicted when integrated into the treatment of and education for other chronic illnesses, resulting in higher acceptability by the users of u-health services. We hope that the result of this research will add the comprehensive advantages and availability of COPD u-health services and provide a foundation for further research and development.
Footnotes
Acknowledgments
This research was supported by a grant (10 High-Tech Urban B02) from High-Tech Urban Development Program funded by the Ministry of Land, Transport, and Maritime Affairs of the Korean government.
Disclosure Statement
No competing financial interests exist.