
Abstract
Introduction
There are 25.8 million people in the United States who have diabetes, with 1.9 million new cases diagnosed in people 20 years of age and older each year. 1 The annual economic cost of diagnosed diabetes in 2007 was estimated to be $174 billion. 1 Diabetes is associated with an increased risk of serious and sometimes life-threatening complications. Research suggests that patients with formal diabetes education, compared with those without, have superior self-care skills and increased adherence as indicated by lower blood glucose and hemoglobin A1c (A1C) levels. 2 Diabetes self-management education (DSME) improves glycemic control, self-care, and emotional well-being and decreases the cost of care. 3
Many factors may affect the use of DSME, including local availability. 4 Residents in underserved areas frequently have poor access to diabetes services. Telemedicine has been used to address poor access to DSME. Studies using telemedicine to provide DSME suggest that the use of this technology can effectively deliver DSME and can potentially increase delivery of DSME. 4 Surveys completed by individuals with diabetes, physicians, and diabetes educators have demonstrated the acceptance of media sources by patients; however, diabetes educators and physicians tended to underestimate this acceptance. 4 This suggests that alternative strategies based on interactive electronic media are likely to be well received. 4 With only one-third to one-half of people with diabetes in the United States receiving DSME, diabetes educators need to consider incorporating new technologies to help patients receive the diabetes education they need. 4
We have previously reported the successful use of telemedicine in providing diabetes education to patients on an individual (1:1) basis. 3 Participants indicated that they felt comfortable with teleconferencing and found it convenient. Most indicated a willingness to use it again. 3 We now describe the use of teleconferencing to provide DSME in a group setting and the tools used to support this application.
Subjects and Methods
Group DSME (diabetes education class) was provided to individuals face-to-face at our diabetes center in Syracuse, NY (control subjects) or via telemedicine from our center in real-time to a rural health center that provided care to underserved individuals in Oswego, NY. Participants had not previously participated in a diabetes education class or received any type of diabetes education in the previous year. All patients with diabetes from the remote site in Oswego who were referred by their physicians for diabetes education during the time of the study were enrolled (two or three patients per class, one class per month). Control subjects were similarly referred by their physicians for diabetes group education, and those whose class took place during the monthly telehealth time slot participated. Control patients were scheduled for classes based on their time availability. Classes were conducted by a dietitian, a nurse, and an exercise specialist (exercise physiologist/physical therapist); all were certified diabetes educators (CDEs). The same three, experienced educators taught the classes throughout the study. All materials required for the sessions were provided in advance to the rural telemedicine site.
Prior to diabetes education, there was an individual 1-h initial diabetes educational assessment visit in accordance with the national standards for DSME. 5 At this visit a diet and exercise history was obtained. This was done by teleconferencing for the participants in Oswego. After the initial assessment, patients participated in a 6-h “Living with Diabetes” class. This session was conducted by a nurse CDE who discussed the following topics: an overview of diabetes, diabetes medications, insulin, recognition and management of hypoglycemia, diabetes-related complications, sick-day management, and how to deal with diabetes in special circumstances. At the beginning of this visit, height, weight, and A1C were obtained. The participants also completed the Problem Areas in Diabetes (PAID) survey 6 and the Diabetes Treatment Satisfaction Questionnaire (DTSQ). 7
The PAID survey is a 20-item measure that describes common problematic situations for individuals with type 1 or type 2 diabetes, each representing a unique area of diabetes-specific emotional distress. These range from anger and interpersonal distress to frustration with aspects of the diabetes regimen. On a 6-point Likert scale, patients rate the degree to which each item is currently problematic for them, with 1 being no problem to 6 being a serious problem. The higher the score, the more diabetes-related stress. 6 The DTSQ was designed to assess diabetes treatment satisfaction in specific areas and perceived frequencies of hyperglycemia and hypoglycemia. Each of the eight items is scored on a scale of 0–6. For most questions the higher the score, the greater the satisfaction with treatment. When the perceived frequency of hyperglycemia and hypoglycemia is being addressed, a higher score indicates a problem. 7
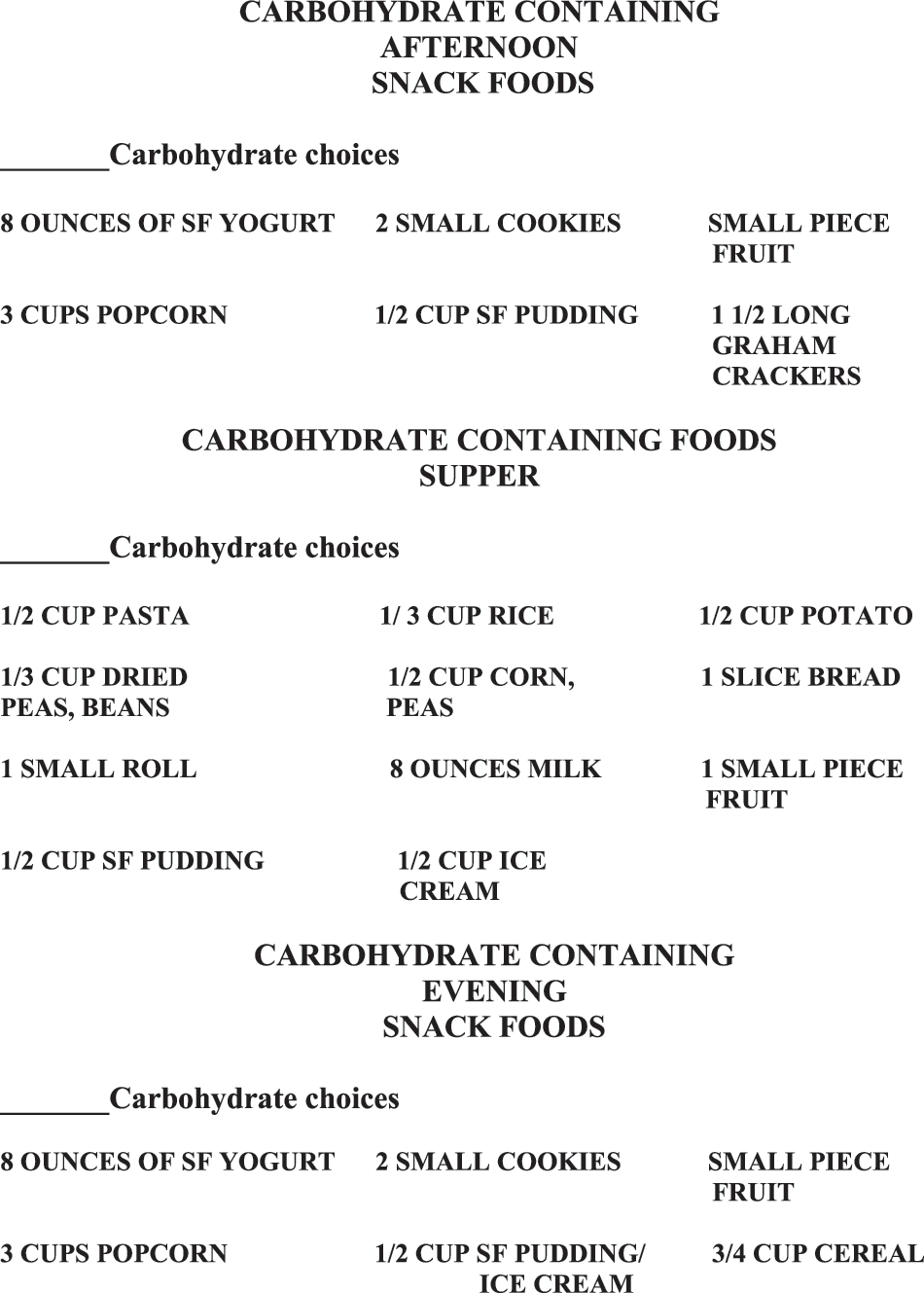
The “Living with Diabetes” class also included instruction from a dietitian (CDE) and physical therapist (CDE), who covered meal planning and physical activity. The nutrition section of the class reviewed the relationship between foods eaten and their effect on blood glucose levels and diabetes with the focus on carbohydrate consistency. After the didactic section of the nutrition component, participants created their own meal plan focusing on carbohydrate consistency. They were asked to review their food diary and highlight those foods that contain carbohydrate (Fig. 1). From the food diary, participants estimated the number of carbohydrate servings they were currently eating at each meal and snack and completed the meal plan worksheet (Fig. 2). With the assistance of a document camera, food models were used to demonstrate appropriate portion sizes. Once the current carbohydrate intake was estimated, the educator reviewed the importance of having the daily distribution of carbohydrates match their medication and exercise regimen to help improve their glycemic control. Participants negotiated new carbohydrate goals depending on their individual needs, including goal for weight management and patterns of high/low blood glucose (Fig. 2). Using their new carbohydrate goals, participants created sample menus (Fig. 3). At the end of the nutrition section, the food diaries and new meal plan were collected and reviewed by the dietitian for adequacy. The foods that were high in fat were circled in red. Food diaries and the new meal plans were mailed to participants with a letter containing suggestions for improvements.

Eating habits worksheet.
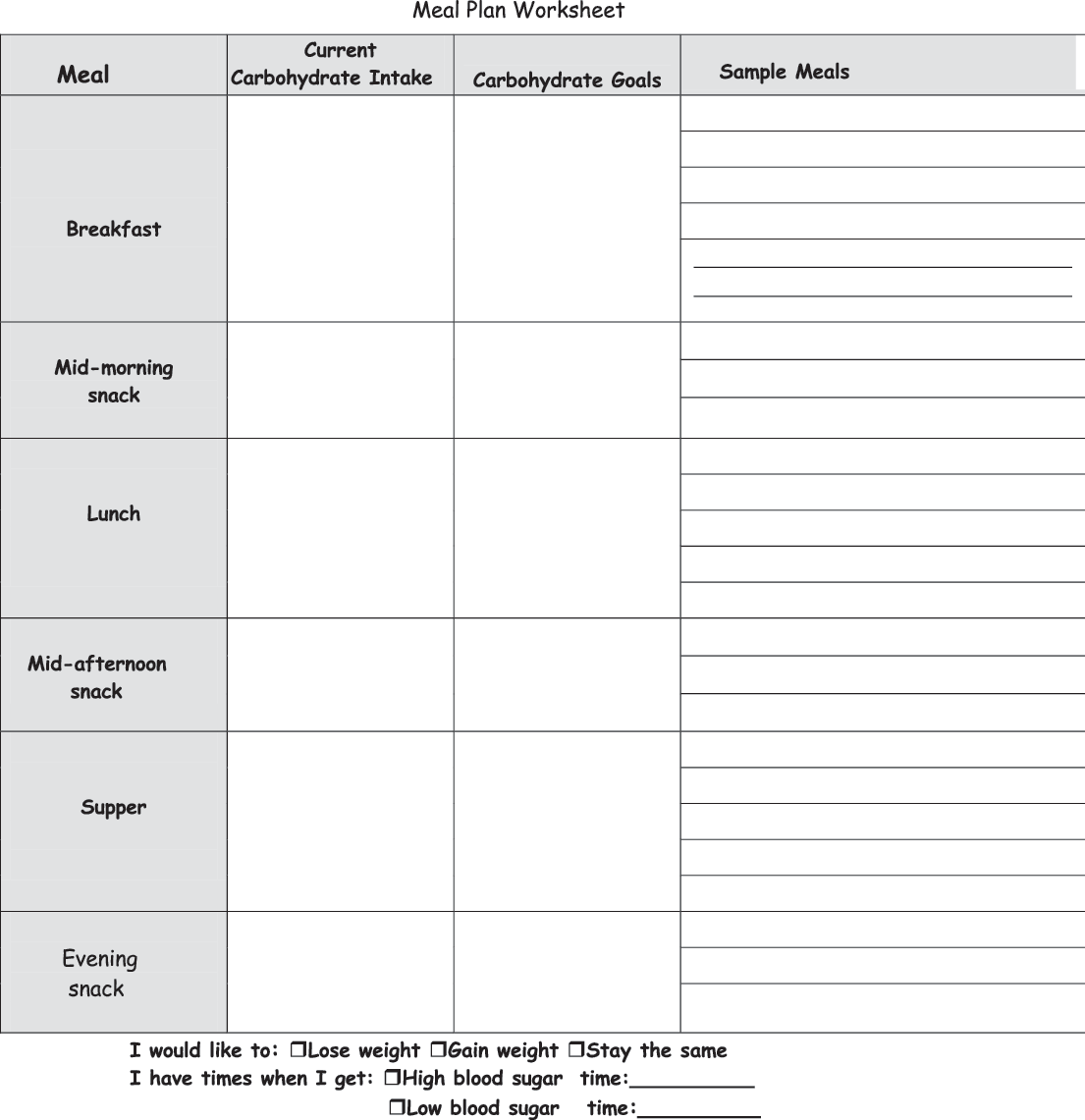
Meal planning worksheet.

Menu selections. SF, sugar-free.

The exercise section was conducted in a similar manner. An exercise history was taken during the initial assessment visit (Fig. 4). The exercise specialist reviewed the relationship between exercise and diabetes, and participants used their worksheet to create an exercise prescription according to guidelines offered by the exercise specialist. The activity plan was individualized according to the needs of each individual (Fig. 5). After the exercise prescription was reviewed for safety and adequacy, the exercise prescription was mailed to the participants. At the completion of this class, a post-test was administered to assess knowledge in all content areas. Participants completed the goal setting form (Fig. 6), in which participants were asked to set specific diabetes-related goals. In addition to choosing specific goals, participants were requested to document how frequently they checked their feet.
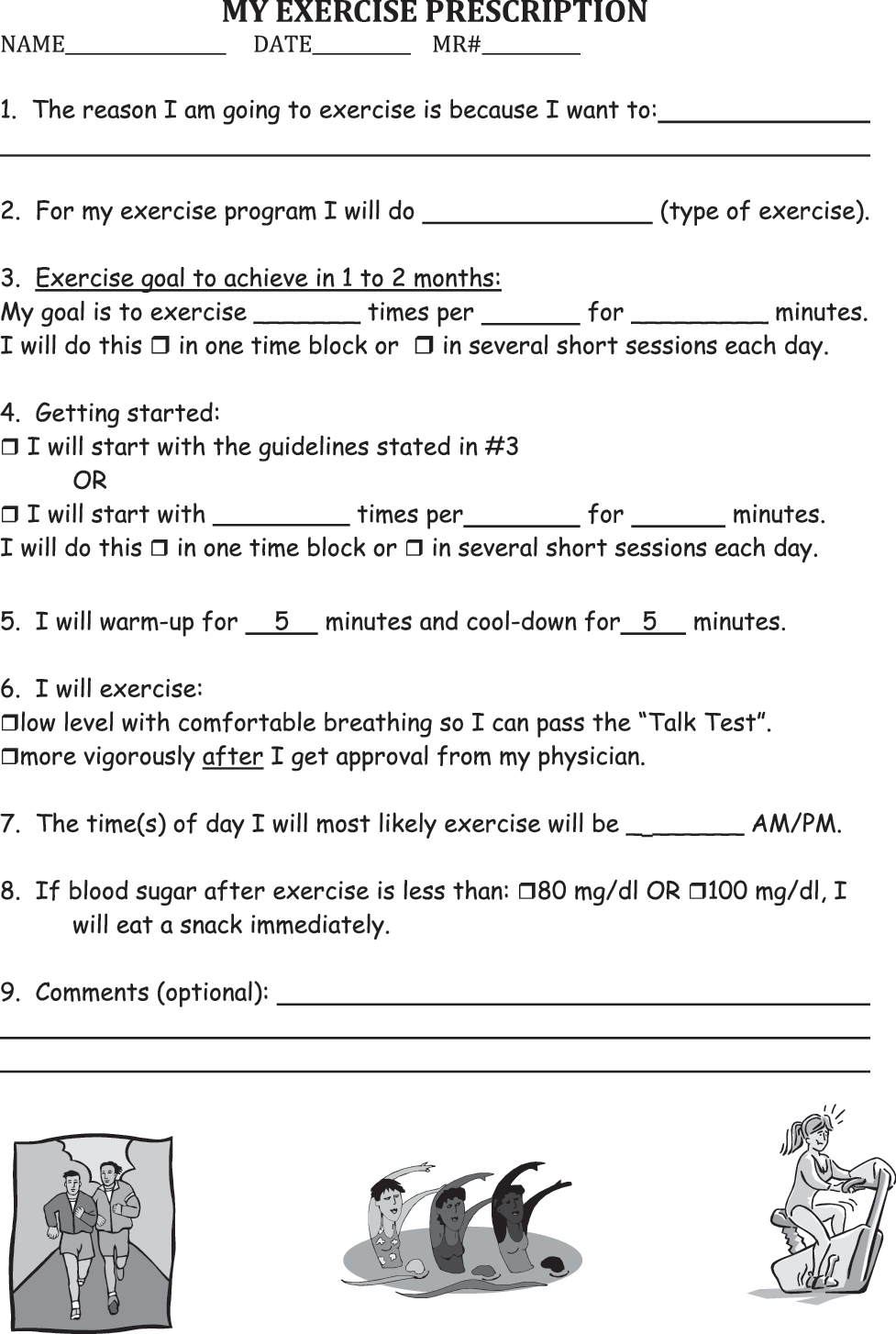
Exercise prescription.
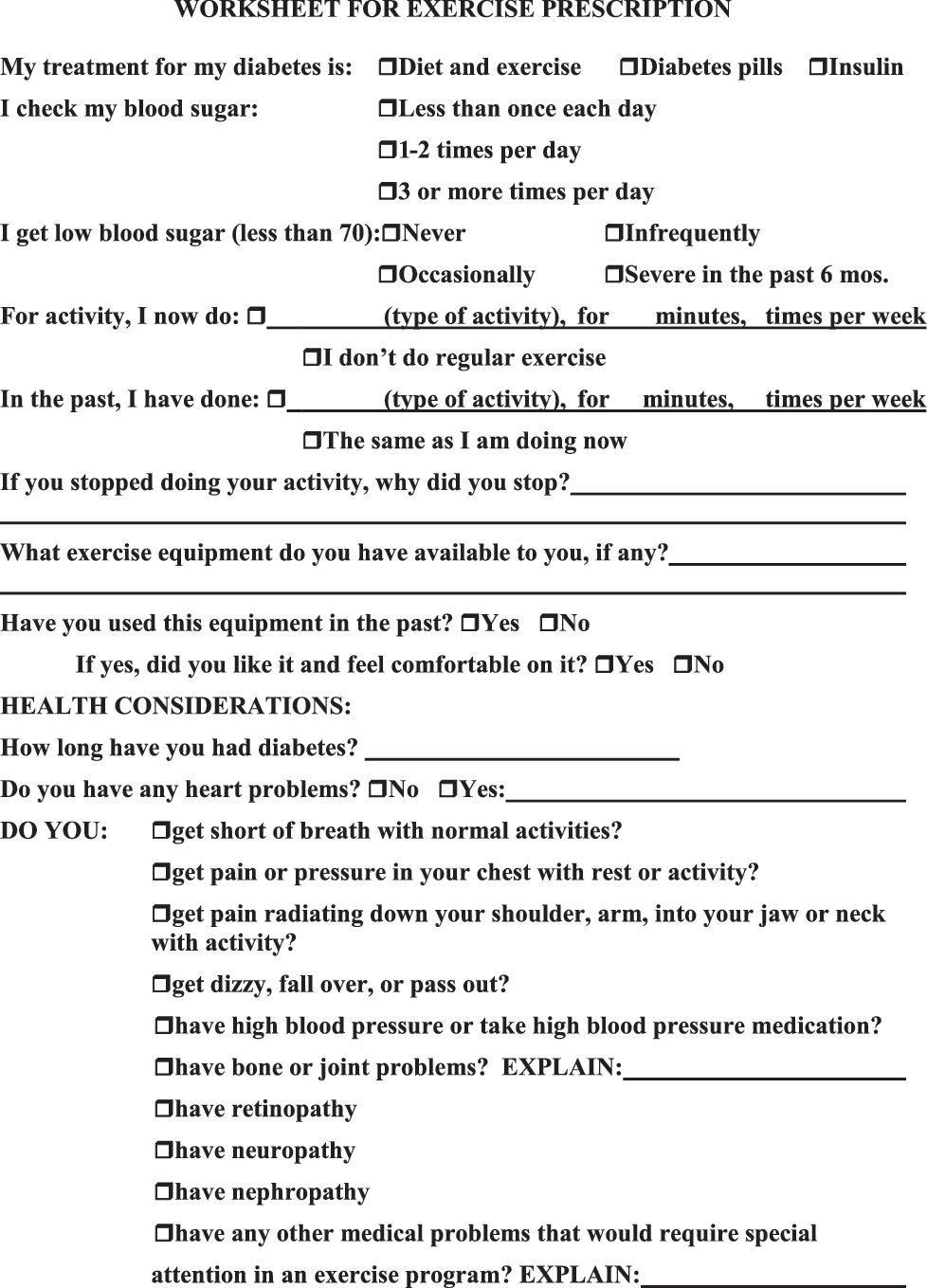
Exercise prescription worksheet.

Telemedicine “Living with Diabetes” goals.
One month after completion of the “Living with Diabetes” class, participants attended a follow-up class (“Living with Diabetes Follow Up” class), in which the previously discussed content areas were reviewed and discussed. Participants were encouraged to ask questions.
At 3 and 6 months after the follow-up class, the participants returned for an individual post-assessment visit, where weight and A1C were obtained and the PAID survey and DTSQ were completed. Participants from the remote site completed the telemedicine satisfaction survey. Individual goal achievement and the frequency of foot exams were assessed.
Patients at the remote site received real-time group diabetes telemedicine education via a point-to-point Integrated Services Digital Network line connection using an Intel® ProShare® Video System with camera.
Statistical Analysis
Categorical and continuous baseline characteristics were compared with Pearson's chi-squared test and Student's t test, respectively. However, Fisher's exact test was used to account for small expected cell counts (e.g., <5), and Wilcoxon's test was used for skewed distributions such as duration of diabetes.
Multilevel models were implemented to compare rates of change in outcomes between telemedicine group therapy and face-to-face treatment modalities over a 6-month assessment period. Multilevel models consisted of fixed effects for group, time, and a group by time interaction and a random intercept to account for dependence among observations within participants. Means, standard errors, and confidence intervals were calculated by writing estimate (i.e., contrasts) statements within Proc Mixed (SAS, Cary, NC). Graphical and numerical exploratory data analyses were conducted to ascertain the nature of the correlational structure of outcomes and the linearity of outcome trajectories over time and to ensure residuals did not grossly deviate from normality.
While the multilevel model handles incomplete data without resorting to list-wise deletion of cases and provides for unbiased parameter estimates under a missing at random assumption, the validity of the missing at random assumption cannot be determined from the data obtained. Methods such as pattern-mixture models can be used to classify and assess missing data patterns. Given the relatively small sample size and pilot nature of this study, we chose to assess the sensitivity of missing data on results by applying a less complex method. Our multilevel models used on the entire cohort were also applied to the subset of individuals who had complete data. Relative differences in fixed effect slope estimates between cohorts were calculated for each group, and applicable differences were followed up with further analyses.
Results
Table 1 shows baseline characteristics of participants. There were no significant differences in the participants at baseline. The mean age of participants was 54.9±10.9 years (mean±standard deviation) in the face-to-face group and 49.8±11.5 years in the telemedicine group (p=0.091). The duration of diabetes was 10.3±10.5 years in the face-to-face group versus 6.6±8.0 years in the telemedicine cohort (p=0.084). Although 43% of participants were male in the face-to-face group versus 29% in the telemedicine group, this difference was not statistically significant (p=0.25).
Baseline Characteristics of Participants
Data are mean±standard deviation values.
A1C levels improved slightly in each group (face-to-face and telemedicine), but the difference was not significant between groups or within groups (Fig. 7). There was no significant change in weight between groups or within groups (p=0.138). In this pilot project, the number of participants may have been too small to detect such differences.

Hemoglobin A1c levels at baseline and 3 months and 6 months post-intervention. The bars represent 95% confidence intervals. SE, standard error.
Figure 8 shows that each group had significant improvements in PAID scores indicating less diabetes-related distress, with no difference between groups. This suggests better psychological adjustment to diabetes in participants who receive diabetes education either face-to-face or via telemedicine.
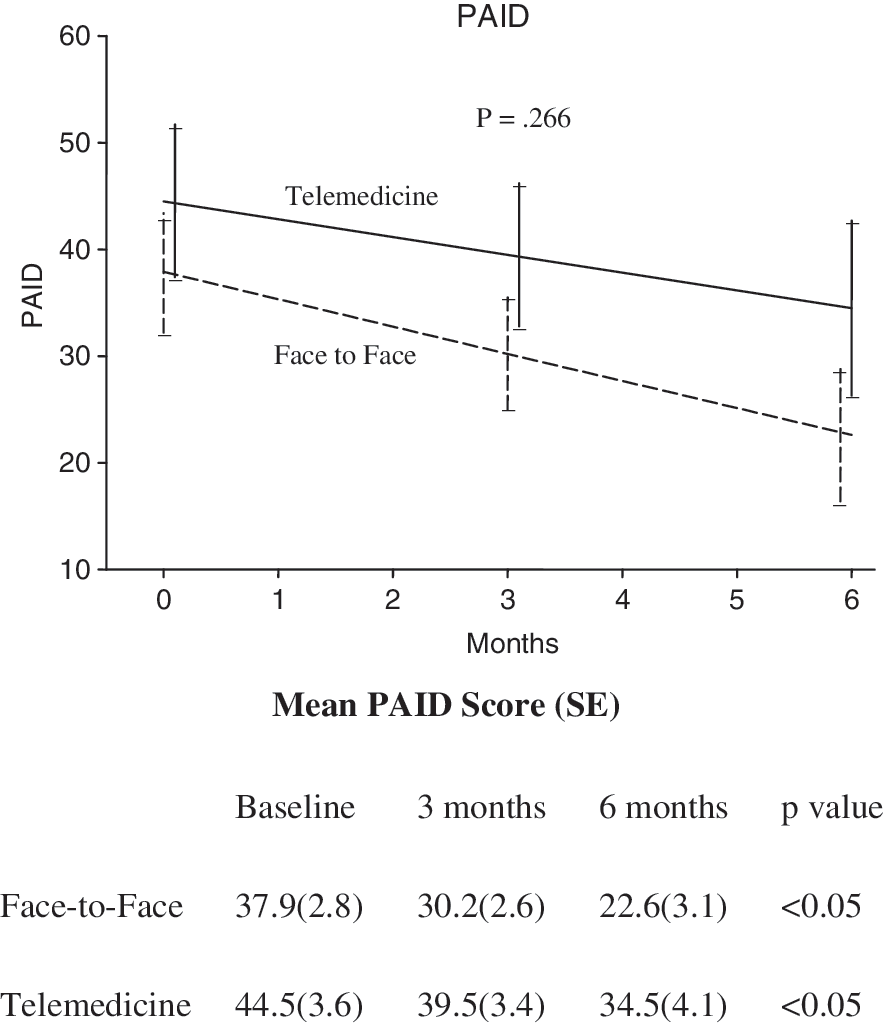
Problem Areas In Diabetes (PAID) scores at baseline and 3 months and 6 months post-intervention. The data are reported as mean±SE values.
Diabetes treatment satisfaction as measured in the DTSQ improved in the face-to-face group but not in the telemedicine group (p<0.001) (Fig. 9). The group that had face-to-face education received their medical care at our diabetes center, and the telemedicine group received their medical care from their primary care providers. Whether this affected DTSQ scores is unknown.
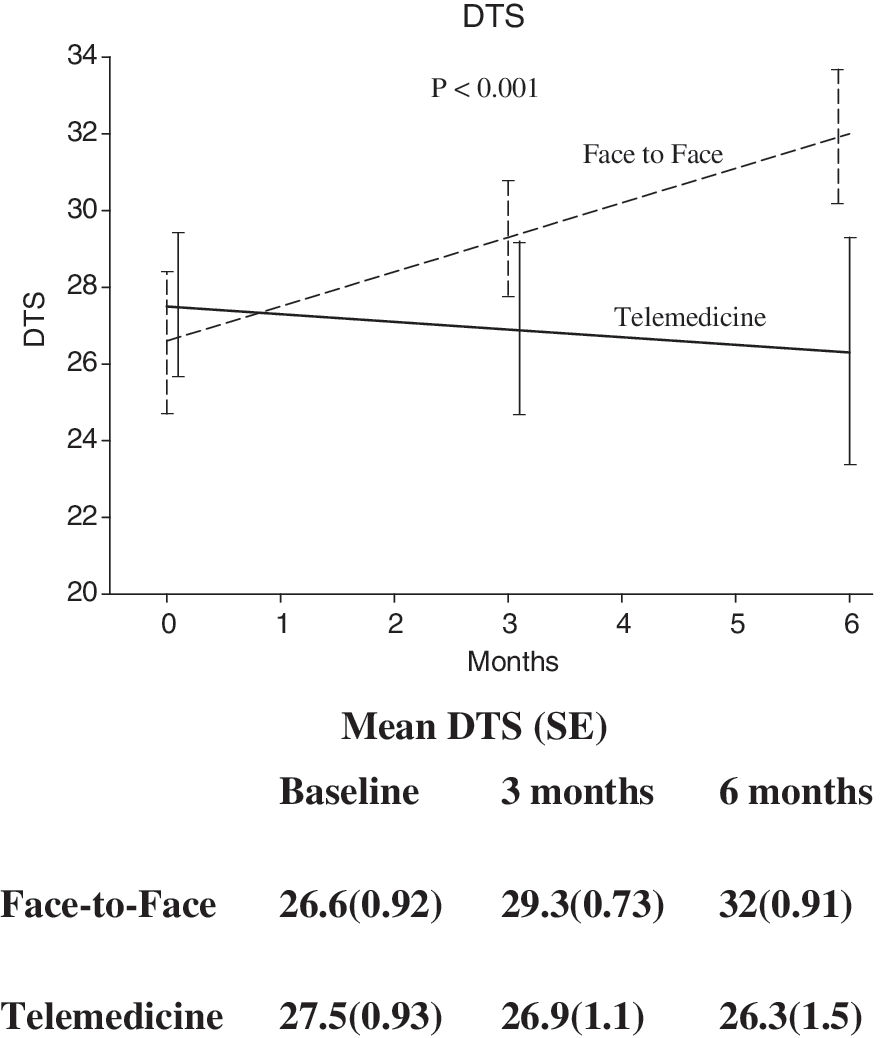
Diabetes Treatment Satisfaction (DTS) Questionnaire scores at baseline and 3 months and 6 months post-intervention. The data are reported as mean ± SE values.
Table 2 shows that for participants who received diabetes education via teleconferencing, satisfaction was high. Most participants found this form of instruction comfortable and convenient and were highly satisfied. They had little concern about their medical privacy not being protected.
Patient Telemedicine Satisfaction Survey
SD, standard deviation.
Discussion
Methods of delivering diabetes education have evolved over time. Self-management education, which is critical for people with diabetes, can occur in a variety of settings, ranging from primary care physicians' offices and designated diabetes centers to community settings. The use of telemedicine should be more widely considered to help reach the one-half to two-thirds of the people in the United States who do not receive diabetes education. 4 In our program, the same education materials were used when providing education with teleconferencing or face-to-face. Packets of materials (i.e., Figs. 1 –6) were delivered to the remote site, with materials for each session clearly marked. Our pilot study indicated that the materials we used for diabetes self-management instruction are acceptable for telemedicine use.
There are challenges that need to be addressed when first using telemedicine for group DSME. First, it is very important to have a good understanding of the equipment. One needs the ability to troubleshoot when technical problems arise. If there is insufficient technical expertise at the remote site, the sessions may be delayed, and patient satisfaction can be adversely affected. Second, a committed healthcare provider at the distant site is needed to control the equipment and help the participants when needed. Responsibilities include obtaining the height, weight, and A1C and collection of all data. When we did not have a committed person available at the remote site, initiation and completion of the sessions were more difficult.
This was a pilot study, and the conclusions that can be drawn are limited by the small number of participants. We were not able to reach enough power to detect a difference between groups because recruitment was low at the remote site. Perhaps, if we had a higher number of participants we may have detected a difference between the groups or detected a significant improvement in A1C after diabetes education as we did in our study in which participants received 1:1 diabetes education via telemedicine versus face-to-face. Similarly, although gender differences were not detected, these analyses were limited by the small number of participants.
Another methodological challenge was that the study was not randomized. It was not feasible to ask participants from Syracuse to travel to Oswego to receive diabetes education. This lack of randomization may have contributed to the higher diabetes treatment satisfaction score in the face-to-face group. This group received medical care at a diabetes center and benefited from a team, case management approach to diabetes care. The remote site group received diabetes care from their primary care providers.
Summary
The results from this pilot study suggest that telemedicine is an effective tool for providing group diabetes education to individuals with poor access to education programs. Diabetes educators have an important role to play in developing this mode of diabetes education and making it available to people with diabetes. With current technological advances, mechanical connection problems are declining, and the cost of transmission is decreasing, further increasing the feasibility of this approach.
Footnotes
Acknowledgments
The authors thank Dr. Dennis Norfolk and Mary Hitchcock, R.N., at Oswego County Opportunities for their assistance. This work was supported, in part, by the New York State Department of Health.
Disclosure Statement
No competing financial interests exist.